
Abstract
There is a high incidence of parental reporting of abnormal swallowing and feeding function and the negative impacts thereof on children. As such there is a need for well validated assessments in the area of pediatric swallowing and feeding. While instrumental assessments are well validated, there is limited information available to guide the selection and use of non-instrumental assessments for swallowing and feeding function. The aim of this study was to identify and report on non-instrumental assessments available to clinicians for pediatric swallowing and/or feeding function in order to support clinical decision making. A systematic literature search was performed by two independent reviewers using Medline and Embase databases, to find non-instrumental assessments for pediatric swallowing and feeding function. Published assessments were also included in the study by searching well-known publishers and relevant feeding and swallowing textbooks. Assessments were summarized and evaluated according to respondent type, target populations, assessment design, domains of assessment and scoring. Thirty assessments were included in the final review. All assessments had either caregiver or clinician respondents. There was high variability in target populations, assessment designs and areas of assessment. Twenty-four of the 30 assessments did not provide instruction for scoring or interpreting scores. There is high variability among the many assessments available to clinicians in the area of feeding and swallowing function in pediatrics. There appears to be limited information available on the validity and reliability of these assessments. Thus, most assessments need to be used with caution. Further research is needed to evaluate the psychometric properties of the assessments.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Oropharyngeal dysphagia can refer to problems with chewing and preparing food, transporting a bolus from the oral cavity to the back of the tongue, moving food into the esophagus, or unsafe and inefficient swallowing [1]. The term oropharyngeal dysphagia is not commonly used in pediatric populations as oropharyngeal and esophageal dysfunction are intrinsically linked in this population [2]. Swallowing dysfunction in the general population has been linked to poorer patient outcomes including higher rates of malnutrition [3], higher mortality rates [4, 5], increased medical complications [6, 7], longer hospitalisations [4, 7, 8], poorer immune responses [6], higher support required post hospital discharge [6, 7], and overall poorer quality of life (QoL) [4, 6]. In addition to the poor health outcomes that are associated with swallowing difficulties, pediatric populations, face physical, and developmental challenges if their nutritional and caloric intake is not sufficient [9–13].
In addition to swallowing difficulties, children may also be at risk of reduced nutrition and caloric intake due to feeding difficulties. Feeding difficulties in pediatrics may be broadly defined as difficulties eating adequately which may result in reduced absorption or consumption of food, impacting on physical and/or psychosocial function [14]. Feeding difficulties in children or infants have been associated with negative parent–child interactions, anxiety, stress, social avoidance, and specific fears (phobias) [15–18].
Studies have previously estimated that around 20–45 % of parents within the general population report that their children have some form of feeding or swallowing difficulty [19–22], and that between 3 and 10 % of children have significant swallowing or feeding difficulties resulting in significant health or developmental consequences [23]. Swallowing and feeding difficulties are also projected to increase due to improved survival rates of infants born prematurely or with complex medical conditions [19]. Given the high rates of swallowing and feeding difficulties and the negative consequences of these conditions, it is important to use assessments with sound psychometric properties in order to support early identification and optimize treatment outcomes [19, 24–28]. Current evidence for swallowing and feeding difficulties in pediatric populations recommends the use of a multidisciplinary team approach for both conducting comprehensive assessments and delivery of interventions [19, 25, 29]. The use of videofluoroscopy and fiberoptic endoscopic evaluation of swallowing to assess swallow function (or dysfunction) is well supported in the literature [6, 27–31]. However, there is a lack of discussion and support for the use of standardized, psychometrically sound measures of swallowing or feeding function, such as non-instrumental assessments, which can augment or serve as alternatives to instrumental assessment in order to reduce unnecessary cost and the use of invasive procedures [32–36].
This systematic review is a first step in addressing the need to identify and report on the characteristics of non-instrumental assessments in the areas of both pediatric swallowing and feeding functions that are available to clinicians. The terms swallowing and feeding function (i.e., normal swallowing and feeding) and swallowing and feeding dysfunction (i.e., swallowing and feeding difficulties or disorders) are used throughout this manuscript and include behavioral aspects of feeding.
Methods
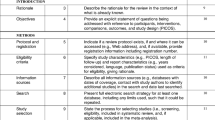
This review was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [37]. A systematic literature search was conducted using Medline and Embase online databases (Table 1). From this search, all appropriate journal abstracts up to June 2013 were included. Both databases were searched using medical subject headings (MeSH) or Thesaurus terms and free text. Two independent abstract reviewers selected abstracts and original publications of non-instrumental assessments according to the inclusion and exclusion criteria as described in Table 2. Reference lists of included articles were also searched for further publications and assessments. Eligibility of publications was appraised independently by both reviewers; consensus was reached through discussion where there was disagreement on eligibility.
The non-instrumental assessments were then identified by searching for the original, first publication that described the selected assessment, and when this failed, by contacting the authors directly. To ensure that the search was comprehensive, well-known publishers for assessment tools and textbooks around the topic of pediatric swallowing or feeding were also searched so as to capture relevant assessments that have been published in sources other than research databases. The assessments were then considered for eligibility according to inclusion and exclusion criteria as listed in Table 3. For assessments to be included, they were required to (a) have at least 50 % of the items related to swallowing or feeding; (b) be designed for use with pediatric populations; and (c) needed to be of a non-instrumental assessment design (i.e., the assessment was not used in instrumental assessment processes or for retrospective video assessment). Guidelines for clinicians for case history taking and surveys were excluded. Eligibility of these assessments and analysis of the characteristics and assessment domains were independently appraised by two reviewers, who again reached consensus through discussion. Figure 1 provides an overview of the process of inclusion according to the PRISMA flow diagram [39].

Flow diagram of the reviewing process according to PRISMA. Study flow diagram showing the process of inclusion for assessments. The flow diagram follows the structure as recommended by PRISMA [39]
Results
Systematic Literature Search
The systematic searches in Medline and Embase yielded 2201 records. A total of 76 original non-instrumental assessments were retrieved from the database, publisher, and textbook searches and the reference lists of the included articles. The assessments were evaluated using the inclusion criteria for assessments (Table 3).
Of the 76 assessments, 46 were excluded as they did not meet the inclusion criteria (see Table 4). The 46 assessments were excluded for the following reasons: 27 were excluded as less than 50 % of the assessment items were not related to feeding and/or swallowing; 6 assessments did not assess the target population of children or infants; and 13 assessments were excluded as they did not meet the requirements for non-instrumental assessments. A total of 30 non-instrumental assessments were identified as meeting all inclusion criteria as they investigated feeding or swallowing function in children of various aetiologies in various domains of feeding or swallowing functioning (see Table 5).
Respondents and Assessment Style
The assessments were designed to be completed by two types of respondents: caregivers (Table 6) or clinicians (Table 7). Of the 30 included assessments, 11 were identified as caregiver assessments; 9 of which took a case history style approach to asking questions and two focused on observation instead (Table 6). Eighteen assessments were designed to be completed by clinicians; these assessments all used clinical observations of swallowing or feeding function or set clinical tasks (Table 7). One assessment could be completed by either caregivers or clinicians and utilised a case history style of assessment (Table 8).
Target Populations
While all assessments were developed to investigate swallowing or feeding function in pediatric populations, various target groups (including diagnostic and age groups) were identified (Tables 6, 7 and 8). Nine assessments were developed to assess the swallowing and feeding difficulty of infants and children from birth to 2 years with no specific illness: Clinical Evaluation of Pediatric Dysphagia [40], Clinical Feeding Evaluation of Infants [82], Clinic/Bedside Oral-Sensorimotor Feeding Assessment Worksheet [81], Developmental Pre-Feeding Checklists [65], Early Feeding Skills Assessment (EFS) [84], Oral Motor and Feeding Evaluation [77], Pediatric Dysphagia Clinical Evaluation [68], Schedule for Oral Motor Assessment (SOMA) [98], and Systematic Assessment of the Infant at Breast (SAIB) [100]. Three assessments were developed to assess swallowing and feeding function in infants born prematurely: Feeding Questionnaire [88], Neonatal Oral-Motor Assessment Scale (NOMAS) [92], and Preterm Infant Breastfeeding Behavior Scale (revised) (PIBBS) [97]. One assessment was specifically developed to investigate infants (of unspecified gestational ages) with severe swallowing and feeding difficulties: Pediatric Assessment Scale for Severe Feeding Problems (PASSFP) [95].
Six assessments were developed to assess children with no specified illnesses other than having potential swallowing or feeding difficulties: Behavior Focused Feeding Assessment [76], Brief Assessment of Motor Function (Oral Motor Deglutition scale) (BAMF-OMD) [78], Children’s Eating Behavior Inventory (CEBI) [80], Feeding Strategies Questionnaire [89], Mealtime Behavior Questionnaire [90], and Parental Feeding Questionnaire [94]. Three assessments were developed to assess swallowing or feeding difficulties in children with autism spectrum disorders (ASD) as the target population: BAMBI, Eating Profile [85], and Screening Tool of Feeding Problems, modified for children (STEP-Child) [99]. Four assessments were developed to assess swallowing and feeding difficulties in children with cerebral palsy (CP) or other neurological conditions as the target populations: Feeding and Swallowing Questionnaire [86], Multidisciplinary Feeding Profile (MFP) [91], Oral Motor Assessment Scale (OMAS) [93], and Pre-Speech Assessment Scale (PSAS) [96]. Two assessments were developed to assess swallowing or feeding function in children with “developmental delay” as the target population: behavioral assessment scale of oral functions in feeding (BASOFF) [77] and Dysphagia Disorder Survey (DDS) [83]. One assessment was developed to assess swallowing or feeding difficulties in children with chronic illnesses as the target population: About Your Child’s Eating (AYCE) [75], and one assessment was developed to assess swallowing or feeding difficulties in children with phenylketonuria as the target population: Feeding Assessment [87].
Age ranges for all the assessment varied greatly, ranging from birth of premature infants to adults (Fig. 2). Twelve assessments targeted infants and children between birth and 2 years of age (only); a time where typically developing children are still developing their ability to swallow and feed [1]: Clinical Evaluation of Pediatric Dysphagia, Clinical Feeding Evaluation of Infants, Developmental Pre-Feeding Checklists, EFS, Feeding Questionnaire, NOMAS, Oral Motor and Feeding Evaluation, PASSFP, PSAS, PIBBS, SOMA, and SAIB. Seven assessments investigated swallowing and feeding function in a range of ages beginning within 0–2 years and continuing up to childhood or adulthood: BASOFF, BAMF- OMD, Clinic/Bedside Oral-Sensorimotor Feeding Assessment Worksheet, Feeding and Swallowing Questionnaire, Feeding Assessment, Parental Feeding questionnaire, and Pediatric Dysphagia Clinical Evaluation. Finally, 11 assessments investigated swallowing or feeding function in populations with ages beginning in early childhood and extending through to middle childhood or up to adulthood: Behavior Focused Feeding Assessment, BAMBI, CEBI, Eating Profile, Feeding Strategies Questionnaire, Mealtime Behavior Questionnaire, OMAS, AYCE, DDS, MFP, and STEP-Child.

Overview of non-instrumental assessment tools for swallowing and feeding function in children: Age ranges are shown for each assessment. Arrows indicate assessments with age ranges extending higher than 18 years. Where no specific ages were given, the terms used within the text have been provided (where possible) and estimates of appropriate ages have been given according to the authors’ discretion
Assessment Design
There were many different response options used in the assessments including binary scoring, ordinal scales, ratio scales, visual analogue scales (VAS), questions with multiple options, and open questions; 17 of the 30 assessments used a combination of multiple response options (Tables 6, 7, 8). The length of assessments also varied; one assessment consisted of a single scale and seven items (OMAS), while another had 12 subscales and 157 items (Eating Profile) (Tables 6, 7, 8). Twenty-three of the 30 assessments did not specify the time required to administer the assessment; however, the administration times that were reported ranged from 5 min (BAMF-OMD and PASSFP) to 2 ½–3 h (PSAS).
Scoring
Six assessments provided instruction for scoring and were designed with cut-off scores to distinguish between normal versus abnormal swallowing or feeding function: Mealtime Behavior Questionnaire, OMAS, PSAS, PASSFP, SOMA, and STEP-Child. Sixteen of the 30 assessments used qualitative descriptors rather than a numerical scoring system: Behavior Focused Feeding Assessment, Clinical Evaluation of Pediatric Dysphagia, Clinical Feeding Evaluation of Infants, Clinic/Bedside Oral-Sensorimotor Feeding Assessment Worksheet, Developmental Pre-Feeding Checklists, Eating Profile, EFS, Feeding and Swallowing Questionnaire, Feeding Assessment, Feeding Questionnaire, NOMAS, Oral Motor and Feeding Evaluation, Parental Feeding Questionnaire, Pediatric Dysphagia Clinical Evaluation, PIBBS, and SAIB. The remaining eight assessments provided no instruction for interpretation of the results.
Assessment Domains
The following assessment domains were identified: oral motor skills, behaviors related to swallowing or feeding function, environmental factors related to functional swallowing and feeding, physical swallowing or feeding skills, QoL in relation to swallowing or feeding difficulties, and sensory aspects of swallowing or feeding function (Table 9). Twenty-three assessments included items specific to the domain of swallowing or feeding skills, 17 assessments included items specific to oral-motor skills, 10 included items specific to behavioral aspects of swallowing or feeding, six included items specific to environmental aspects of swallowing and feeding, five included items related to sensory aspects of swallowing or feeding, and two included items specific to QoL aspects of swallowing or feeding. Twenty-three of the 30 assessments covered more than one domain, with two of the assessments covering four of the six domains.
Discussion
Variations Among Assessments
The swallowing and feeding assessments included in this review demonstrated variability in terms of target populations, the design of each assessment, and the assessment domains. This variation likely reflects the need to capture a wide range of children with swallowing or feeding difficulties across multiple domains (e.g., a combination of behavioral and sensory difficulties) and who have multiple risk factors (e.g., neurological conditions and a developmental disorder) [27, 101]. As a result, the variation among these assessments reflects the diversity and complexity of the target populations and is also likely to reflect the diversity of both the professionals involved and their clinical settings, each with their unique approach to clinical practice and resource restrictions (such as availability of time, equipment, or finances).
Validity and Reliability
The aim of this report was to provide clinicians with an overview of a broad range of non-instrumental swallowing and feeding assessments. While this manuscript does not investigate the psychometric quality of the assessments, the review of the assessments made it apparent that there is a proliferation of feeding assessments that have been developed for infants and children with limited research investigating the quality of the psychometric properties of these assessments. This gap became apparent with the lack of information available to support standardized interpretation of many of the assessment scores, and also in a lack of consideration for validity and reliability of many of the assessments during their development.
It is also concerning to note that many assessments within this review appear not to have been assessed for validity and reliability within the populations they are being used, raising the question as to whether they should be used at all. A recent psychometric review has been conducted on the quality of psychometric properties of measures assessing swallowing function in children with CP and other neurological conditions [30]. However, more research is needed to cover areas of swallowing and/or feeding function in other populations. It is recommended that further evaluation of the quality of psychometric properties of these assessments is to be performed using a standardized appraisal tool that is valid and reliable itself, such as the consensus‐based standards for the selection of health measurement instruments (COSMIN) in order to inform clinicians about the reliability and validity of the assessments that they use [102, 103].
With so little research into the reliability and validity of existing assessments, it would be beneficial to prioritise research on developing the psychometric characteristics of existing assessments to build this area of research to a higher, more rigorous, and evidence-based standing. Selecting the most robust clinical assessments based on the quality of its psychometric properties will result in more sound clinical reasoning, selecting appropriate interventions based on valid and reliable assessment scores, and greater confidence in documenting clinical progress and changes over time [104].
Conclusion
Many non-instrumental assessments are available to clinicians to evaluate swallowing and feeding function in pediatric populations. These assessments vary widely in design, assessment domains, and target groups or populations. A lack of instruction for use and interpretation of assessment scores was evident, indicating that many of these assessments may be at risk for inconsistent use and misinterpretation of results. This review highlights characteristics of the assessments for clinicians to support them in selecting appropriate assessments for clinical practice. This paper also highlights the need for future research to comprehensively evaluate the quality of psychometric properties of the retrieved assessments as many tools appeared to lack robust data on their reliability and validity. As the use of assessments without known psychometric properties may result in outcome data that are not evidence-based and cannot be interpreted correctly, a psychometric review will assist in guiding future choices in the assessment and treatment planning.
Abbreviations
- AEPS:
-
Assessment, Evaluation, and Programming System for Infants and Children—Second Edition
- ASD:
-
Autism spectrum disorder
- AYCE:
-
About Your Child’s Eating
- BAMBI:
-
Brief Autism Mealtime Behavior Inventory
- BAMF-OMD:
-
Brief Assessment of Motor Function (Oral Motor Deglutition scale)
- BASOFF:
-
Behavioral assessment scale of oral functions in feeding
- BED:
-
Bedside Evaluation of Dysphagia—Revised Edition
- CCITSN:
-
Carolina Curriculum for Infants and Toddlers with Special Needs
- CCTI:
-
Colorado Childhood Temperament Inventory
- CEBI:
-
Children’s Eating Behavior Inventory
- CEBQ:
-
Children’s Eating Behavior Questionnaire
- CFQ:
-
Child Feeding Questionnaire
- CMFBQ:
-
Child Mealtime Feeding Behavior Questionnaire
- CTCAE:
-
Common Terminology Criteria for Adverse Events
- DASH-3:
-
Developmental Assessment for Individuals with Severe Disabilities—Third Edition
- DAYC-2:
-
Developmental Assessment of Young Children—Second Edition
- DEP:
-
Dysphagia Evaluation Protocol
- DDS:
-
Dysphagia Disorder Survey or Dysphagia Disorders Survey
- DINE:
-
Dyadic Interaction Nomenclature for Eating
- DSFS:
-
Drooling Severity and Frequency Scale
- EFS:
-
Early Feeding Skills Assessment
- FES:
-
Family Environment Scale
- FDA-2:
-
Frenchay Dysarthria Assessment—Second Edition
- FSQ:
-
Feeding and Swallowing Questionnaire
- FSQ:
-
Feeding Strategies Questionnaire
- GVA:
-
Gisel Video Assessment
- IFSQ:
-
Infant Feeding Style Questionnaire
- IFTI:
-
Infant-Toddler and Family Instrument
- MFP:
-
Multidisciplinary Feeding Profile
- NOMAS:
-
Neonatal Oral-Motor Assessment Scale
- NR:
-
Not Reported
- OAG:
-
Oral Assessment Guide for children and young people
- OD:
-
Oropharyngeal Dysphagia
- OMAS:
-
Oral Motor Assessment Scale
- PASSFP:
-
Pediatric Assessment Scale for Severe Feeding Problems
- PIBBS:
-
Preterm Infant Breastfeeding Behavior Scale (revised)
- PMAS:
-
Parent Mealtime Action Scale
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)
- PSAS:
-
Pre-Speech Assessment Scale
- QoL:
-
Quality of Life
- SAFE:
-
Swallowing Ability and Function Evaluation
- SAIB:
-
Systematic Assessment of the Infant at Breast
- SOMA:
-
Schedule for Oral Motor Assessment
- STEP-Child:
-
Screening Tool of Feeding Problems, modified for children
- SWAL-QoL:
-
Swallowing Quality of Life Questionnaire (adapted for use with pediatric patients)
References
Groher M, Crary M. Dysphagia: Clinical management in adults and children. 1st ed. Maryland Heights: Mosby Elsevier; 2010.
European society for swallowing disorders, 3rd congress. Paediatric dysphagia—Position statements [Position Statement]. 2013. www.myessd.org.
Arribas L, Hurtos L, Milà R, Fort E, Peiró I. Factores pronóstico de desnutrición a partir de la valoración global subjetiva generada por el paciente (vgs-gp) en pacientes con cáncer de cabeza y cuello. Nutrición Hospitalaria. 2013;28:155–63.
Altman KW, Yu G, Schaefer SD. Consequence of dysphagia in the hospitalized patient: impact on prognosis and hospital resources. Arch Otolaryngol Head Neck Surg. 2010;136:784–9.
Lecleire S, Di Fiore F, Antonietti M, Ben Soussan E, Hellot M-F, Grigioni S, Déchelotte P, Lerebours E, Michel P, Ducrotté P. Undernutrition is predictive of early mortality after palliative self-expanding metal stent insertion in patients with inoperable or recurrent esophageal cancer. Gastrointest Endosc. 2006;64:479–84.
Grobbelaar EJ, Owen S, Torrance AD, Wilson JA. Nutritional challenges in head and neck cancer. Clin Otolaryngol Allied Sci. 2004;29:307–13.
Macht M, Wimbish T, Clark B, Benson AB, Burnham EL, Williams A, Moss M. Postextubation dysphagia is persistent and associated with poor outcomes in survivors of critical illness. Crit Care. 2011;15:R231.
Guyomard V, Fulcher RA, Redmayne O, Metcalf AK, Potter JF, Myint PK. Effect of dysphasia and dysphagia on inpatient mortality and hospital length of stay: a database study. J Am Geriatr Soc. 2009;57:2101–6.
Nair RH, Kesavachandran C, Shashidhar S. Spirometric impairments in undernourished children. Indian J Physiol Pharmacol. 1999;43:0019–5499.
Loughlin G. Respiratory consequences of dysfunctional swallowing and aspiration. Dysphagia. 1989;3:126–30. doi:10.1007/BF02407130.
Yehuda S, Rabinovitz S, Mostofsky DI. Nutritional deficienies in learning and cognition. J Pediatr Gastroenterolo Nutr. 2006;43:S22–5.
Fanjiang G, Kleinman RE. Nutrition adn performance in children. Curr Opin Clin Nutr Metab Care. 2007;10:342–7.
Kohda E, Hisazumi H, Hiramatsu K. Swallowing dysfunction and aspiration in neonates and infants. Acta Otolaryngol. 1994. doi:10.3109/00016489409124331.
American Psychiatric Association. Feeding and eating disorders. Diagnostic and statistical manual of mental disorders 2013. doi:10.1176/appi.books.9780890425596.dsm10.
Bryant-Waugh R, Markham L, Kreipe RE, Walsh BT. Feeding and eating disorders in childhood. Int J Eat Disord. 2010;43:98–111.
Dubois L, Farmer A, Girard M, Peterson K, Tatone-Tokuda F. Problem eating behaviors related to social factors and body weight in preschool children: A longitudinal study. Int J Behav Nutr Phys Act. 2007;4:9.
Ekstein S, Laniado D, Glick B. Does picky eating affect weight-for-length measurements in young children? Clin Pediatr. 2010;49:217–20.
Nicholls D, Christie D, Randall L, Lask B. Selective eating: symptom, disorder or normal variant. Clin Child Psychol Psychiatry. 2001;6:257–70.
Arvedson JC. Assessment of pediatric dysphagia and feeding disorders: clinical and instrumental approaches. Dev Disabil Res Rev. 2008;14:118–27.
Equit M, Palmke M, Becker N, Moritz A-M, Becker S, von Gontard A. Eating problems in young children: a population-based study. Acta Paediatr. 2013;102:149–55.
McDermott BM, Mamun AA, Najman JM, Williams GM, O’Callaghan MJ, Bor W. Preschool children perceived by mothers as irregular eaters: physical and psychosocial predictors from a birth cohort study. J Dev Behav Pediatr. 2008;29:197–205.
Wright CM, Parkinson KN, Shipton D, Drewett RF. How do toddler eating problems relate to their eating behavior, food preferences, and growth? Pediatrics. 2007;120:e1069–75.
Lindberg L, Bohlin G, Hagekull B. Early feeding problems in a normal population. Int J Eat Disord. 1991;10:395–405.
Dobbelsteyn C, Peacocke SD, Blake K, Crist W, Rashid M. Feeding difficulties in children with charge syndrome: prevalence, risk factors, and prognosis. Dysphagia. 2008;23:127–35.
Cerezo CS, Lobato DJ, Pinkos B, LeLeiko NS. Diagnosis and treatment of pediatric feeding and swallowing disorders: the team approach. ICAN: Infant. Child Adolesc Nutr. 2011;3:321–3.
Rogers B, Arvedson J. Assessment of infant oral sensorimotor and swallowing function. Ment Retard Dev Disabil Res Rev. 2005;11:74–82.
Prasse JE, Kikano GE. An overview of pediatric dysphagia. Clin Pediatr. 2009;48:247–51.
Dusick A. Investigation and management of dysphagia. Semin Pediatr Neurol. 2003;10:255–64.
Ashland J. Speech, voice, and swallowing assessment. In: Pereira KD, Mitchell RB, editors. Pediatric otolaryngology for the clinician. New York City: Humana Press; 2009. p. 21–8.
DeMatteo C, Matovich D, Hjartarson A. Comparison of clinical and videofluoroscopic evaluation of children with feeding and swallowing difficulties. Dev Med Child Neurol. 2005;47:149–57.
Newman LA, Keckley C, Petersen MC, Hamner A. Swallowing function and medical diagnoses in infants suspected of dysphagia. Pediatrics. 2001;108:e106.
Bell HR, Alper BS. Assessment and intervention for dysphagia in infants and children: beyond the neonatal intensive care unit. Semin Speech Lang. 2007;28:213–22.
Seiverling L, Williams K, Sturmey P. Assessment of feeding problems in children with autism spectrum disorders. J Dev Phys Disabil. 2010;22:401–13.
Studnik S, Simkiss D. What is the evidence for atypical feeding behaviour assessment tools in children with an autistic spectrum disorder? Arch Dis Child. 2011;96:A40.
Nadon G, Ehrmann Feldman D, Gisel E. Revue des méthodes utilisées pour évaluer l’alimentation des enfants présentant un trouble envahissant du développement. Archives de Pédiatrie. 2008;15:1332–48.
Benfer KA, Weir KA, Boyd RN. Clinimetrics of measures of oropharyngeal dysphagia for preschool children with cerebral palsy and neurodevelopmental disabilities: a systematic review. Dev Med Child Neurol. 2012;54:784–95.
Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, Clarke M, Devereaux PJ, Kleijnen J, Moher D. The prisma statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J Clin Epidemiol. 2009;62:e1–34.
Oxford dictionaries online (2014) In: Simpson J, Weiner E (eds.). Oxford English Dictionary Oxford University Press, Oxford
Moher D, Liberati A, Tetzlaf j, Altman DG (2009) Preferred reporting items for systematic reviews and meta-analyses: The prisma statement. In: Group TP (ed.). PLoSMed 6.
Hall KD. Pediatric dysphagia: Resource guide. San Diego: Singula Thomson Learning; 2001. p. 92–106.
Tobin DL. A breastfeeding evaluation and education tool. J Hum Lactation. 1996;12:47–9.
Langdon C, Jardine K, Cichero J (2013) The essential dysphagia handbook: Claire Langdon, Karen Jardine and Julie Cichero.
Hardy E (1999) Bedside evaluation of dysphagia—revised. Pro-ed incorporated.
Johnson-Martin NM, Attermeier SM, Hacker BJ. The carolina curriculum for infants and toddlers with special needs (ccitsn). 3rd ed. Baltimore MD: Brookes Publishing Co; 2004.
Logemann JA. Evaluation and treatment of swallowing disorders. 2nd ed. Austin: PRO-ED Inc; 1998.
Ainuki T, Akamatsu R. Development of the child mealtime feeding behavior questionnaire. ICAN: infant. Child Adolesc Nutr. 2013;5:14–21.
Johnson SL, Birch LL. Parents’ and children’s adiposity and eating style. Pediatrics. 1994;94:653–61.
Wardle J, Guthrie CA, Sanderson S, Rapoport L. Development of the children’s eating behaviour questionnaire. J Child Psychol Psychiatry. 2001;42:963–70.
Rowe DC, Plomin R. Temperament in early childhood. J Pers Assess. 1977;41:150–6.
U.S Department of Health and Human Services. Common terminology criteria for advrse events (ctcae). National Institutes of Health National Cancer Institute; 2009.
Corbin-Lewis K, Liss JM, Sciortino KL. Clinical anatomy & physiology of the swallow mechanism. Stamford: Cengage Learning; 2004.
Dykes MK, Mruzek DW (2012) Developmental assessment for individuals with severe disabilities—third edition: Examiner’s manual. Pro-ed incorporated.
Voress JK, Maddox T (2012) Developmental assessment of young children-second edition. Pro-ed incorporated.
Ireland PJ, Johnson S, Donaghey S, Johnston L, McGill J, Zankl A, Ware RS, Pacey V, Ault J, Savarirayan R, Sillence D, Thompson E, Townshend S. Developmental milestones in infants and young australasian children with achondroplasia. J Dev Behav Pediatr. 2010;31:41–7.
Scott A, Johnson H. A practical approach to the management of saliva. 2nd ed. Austin: Pro-ed; 2004. p. 140–7.
Thomas-Stonell N, Greenberg J. Three treatment approaches and clinical factors in the reduction of drooling. Dysphagia. 1988;3:73–8.
Stark LJ, Jelalian E, Powers SW, Mulvihill MM, Opipari LC, Bowen A, Harwood I, Passero MA, Lapey A, Light M, Hovell MF. Parent and child mealtime behavior in families of children with cystic fibrosis. J Pediatr. 2000;136:195–200.
Smith A, Rosen AB, Dellarosa D (1998) Dysphagia evaluation protocol manual. Pearson.
Moos RH, Moos B. Family environment scale manual and sampler set: development, applications and research. 4th ed. Palo Alto: Mind Garden Inc; 2009.
Cichero J, Langmore S. Imaging assessments. In: Cichero J, Murdoch B, editors. Dysphagia: Foundation, theory and practice. Hoboken, New Jersey: John Wily & Sons; 2006.
Enderby P, Palmer R (2008) Frenchay dysarthria assessment—second edition. Pro-ed incorporated.
Gisel E. Patrick J (1988) Identification of children with cerebral palsy unable to maintain a normal nutritional state. The Lancet. 1988;331:283–6.
Thompson AL, Mendez MA, Borja JB, Adair LS, Zimmer CR, Bentley ME. Development and validation of the infant feeding style questionnaire. Appetite. 2009;53:210–21.
Provence S, Apfel NH. Infant-toddler and family instrument (IFTI). Batimore MD: Brookes Publishing Co; 2001.
Morris SE, Klein MD. Pre-feeding skills: a comprhensive resource for mealtime development. 2nd ed. Tucson: Thrapy Skill Builders; 2000. p. 175–84.
Eilers J, Berger AM. Petersen MC (1988) Development, testing, and application of the oral assessment guide. Oncol Nurs Forum. 1988;15:325–30.
Sjogreen L, Engvall M, Ekstrom AB, Lohmander A, Kiliaridis S, Tulinius M. Orofacial dysfunction in children and adolescents with myotonic dystrophy. Dev Med Child Neurol. 2007;49(1):18–22.
Shipley KG, McAffee JG, Assessment in speech-language pathology. A resource manual. 4th ed. Clifton Park: Delmar Cengage Learning; 2009.
Hendy HM, Williams KE, Camise TS, Eckman N, Hedemann A. The parent mealtime action ssale (pmas). Development and association with children’s diet and weight. Appetite. 2009;52:328–39.
Shipster C, Morgan A, Dunaway D. Psychosocial, feeding, and drooling outcomes in children with beckwith wiedemann syndrome following tongue reduction surgery. Cleft Palate Craniofac J. 2012;49(4):e25–34.
Johnson H, Scott A. Saliva management. In: Cichero J, Murdoch B, editors. Dysphagia: Foundation, theory and practice. Hoboken, New Jersey: John Wiley & Sons Ltd; 2006.
Ross-Swain D, Kipping P, Yee P (2003) Safe: Swallowing ability and function evaluation, Pro-ed incorporated.
Hardy E, Morton N (1999) Swallowing disorders treatment complete kit—second edition, Pro-ed incorporated.
Clayburgh D, Milczuk H, Gorsek S, Sinden N, Bowman K, MacArthur C. Efficacy of tonsillectomy for pediatric patients with dysphagia and tonsillar hypertrophy. Archives of Otolaryngology. Head Neck Surg. 2011;137:1197–202.
Bukowski WM, Davies CM, Davies WH, Noll RB. Mealtime interactions and family relationships of families with children who have cancer in long-term remission and controls. J Am Diet Assoc. 1993;93:773–6.
Arvedson JC, Brodsky L. Pediatric swallowing and feeding: Assessment and management. 2nd ed. Albany, NY: Thomson Delmar Learning; 2002. p. 325–595.
Stratton M. Behavioral assessment scale of oral functions in feeding. Am J Occup Ther. 1981;35:719–21.
Sonies BC, Cintas HL, Parks R, Miller J, Caggiano C, Gottshall SG, Gerber L. Brief assessment of motor function: content validity and reliability of the oral motor scales. Am J Phys Med Rehabil. 2009;88:464–72.
Lukens CT, Linscheid TR. Development and validation of an inventory to assess mealtime behavior problems in children with autism. J Autism Dev Disord. 2008;38:342–52.
Archer LA, Rosenbaum PL, Streiner DL. The children’s eating behavior inventory: reliability and validity results. J Pediatr Psychol. 1991;16:629–42.
Wolf LS, Glass RP. Feeding and swallowing disorders in infancy: Assessment and management. San Antonio: The Psychological Corporation; 1992.
Arvedson J (2008) Evaluation of pediatric feeding and swallowing: ASHA Professional Development, p. 65.
Sheppard JJ, Hochman R, Baer C. The dysphagia disorder survey: validation of an assessment for swallowing and feeding function in developmental disability. Res Dev Disabil. 2014;35:929–42.
Thoyre S, Shaker C, Pridham K. The early feeding skills assessment for preterm infants. Neonatal Netw. 2005;24:7–16.
Nadon G, Feldman DE, Dunn W, Gisel E. Mealtime problems in children with autism spectrum disorder and their typically developing siblings: a comparison study. Autism. 2011;15(1):98–113.
Wilson EM, Hustad KC. Early feeding abilities in children with cerebral palsy: a parental report study. J Med Speech-Lang Pathol. 2009;17(1):31–44.
Harris G, Booth IW. The nature and management of eating prolems in pre-school children. In: Cooper PJ, Stein A, editors. Feeding problems and eating disorders in children and adolescents. Switzerland: Harwood Academic Publishers; 1992.
Demauro SB, Patel PR, Medoff-Cooper B, Posencheg M, Abbasi S. Postdischarge feeding patterns in early- and late-preterm infants. Clin Pediatr. 2011;50(10):957–62.
Berlin KS, Davies WH, Silverman AH, Rudolph CD. Assessing family-based feeding strategies, strengths, and mealtime structure with the feeding strategies questionnaire. J Pediatr Psychol. 2011;36:586–95.
Berlin KS, Davies WH, Silverman AH, Woods DW, Fischer EA, Rudolph CD. Assessing children’s mealtime problems with the mealtime behavior questionnaire. Child Health Care. 2010;39:142–56.
Kenny D, Koheil R, Greenberg J, Reid D, Milner M, Moran R, Judd P. Development of a multidisciplinary feeding profile for children who are dependent feeders. Dysphagia. 1989;4:16–28.
Palmer MM, Crawley K, Blanco IA. Neonatal oral-motor assessment scale: a reliability study. J Perinatol. 1993;13:28–35.
Ortega Ade O, Ciamponi AL, Mendes FM, Santos MT. Assessment scale of the oral motor performance of children and adolescents with neurological damages. J Oral Rehabil. 2009;36:653–9.
Tauman R, Levine A, Avni H, Nehama H, Greenfeld M, Sivan Y. Coexistence of sleep and feeding disturbances in young children. Pediatrics. 2011;127:e615–21.
Crist W, Dobbelsteyn C, Brousseau AM, Napier-Phillips A. Pediatric assessment scale for severe feeding problems: validity and reliability of a new scale for tube-fed children. Nutrition in Clinical Practice. 2004;19(4):403–8.
Morris SE. Pre-speech assessment scale: A rating scale for the measuremnt of pre-speech behaviours from birth through two years. 2nd ed. Clifton: J. A. Preston Corp; 1982.
Nyqvist KH, Rubertsson C, Ewald U, Sjoden PO. Development of the preterm infant breastfeeding behavior scale (pibbs): a study of nurse-mother agreement. J Hum Lactation. 1996;12:207–19.
Reilly S, Skuse D, Mathisen B, Wolke D. The objective rating of oral-motor functions during feeding. Dysphagia. 1995;10:177–91.
Seiverling L, Hendy HM, Williams K. The screening tool of feeding problems applied to children (step-child): psychometric characteristics and associations with child and parent variables. Res Dev Disabil. 2011;32:1122–9.
Shrago L, Bocar D. The infant’s contribution to breastfeeding. J Obstet Gynecol Neonatal Nurs. 1990;19:209–15.
Burklow K, Phelps A, Schultz J, McConnell K, Rudolf C. Classifying complex pediatric feeding disorders. J Pediatr Gastroenterol Nutr. 1998;27:143–7.
Mokkink LB, Terwee CB, Patrick DL, Alonso J, Stratford PW, Knol DL, Bouter LM, Henrica CWDV (2012) Comsin checklist manual. Amstrdam, The Netherlands
Mokkink LB, Terwee CB, Patrick DL, Alonso J, Stratford PW, Knol DL, Bouter LM, Henrica CWdV. The cosmin checklist for assessing the methodological quality of studies on measurement properties of health status measurement instruments: An international delphi study. Qual Life Res. 2010;19:539–49.
Cordier R, Speyer R, Chen Y-W, Wilkes-Gillan S, Brown T, Bourke-Taylor H, Doma K, Leicht A. Evaluating the psychometric quality of social skills measures: a systematic review. PLoS ONE. 2015;. doi:10.1371/journal.pone.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Heckathorn, DE., Speyer, R., Taylor, J. et al. Systematic Review: Non-Instrumental Swallowing and Feeding Assessments in Pediatrics. Dysphagia 31, 1–23 (2016). https://doi.org/10.1007/s00455-015-9667-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00455-015-9667-5