
Abstract
Although the exact pathogenesis of subacute sclerosing panencephalitis (SSPE) remains to be determined, our previous data suggested a genetic contribution to the host susceptibility to SSPE. During chronic viral infection, virus-specific cytotoxic T lymphocytes display poor effector functions. Since co-inhibitory molecules are involved in the suppression of T lymphocytes, we investigated whether single nucleotide polymorphisms (SNPs) of genes encoding co-inhibitory molecules contributed to a susceptibility to SSPE. Association studies on a total of 20 SNPs in 8 genes (CTLA4, CD80, CD86, PD1, PDL1, PDL2, BTLA and HVEM) and subsequent haplotype analysis of 4 SNPs in the PD1 genes were performed in Japanese and Filipino SSPE patients and controls. Then, we investigated a functional difference in promoter activity of two haplotypes and compared the expression levels of PD1 between SSPE and controls. The frequency of GCG(C) haplotype of PD1 containing −606G allele was significantly higher in SSPE patients than in controls both in Japanese and in Filipinos. The promoter activity was significantly higher in the construct with −606G allele than in that with −606A allele. The expression levels of PD1 were significantly higher in SSPE patients than in the controls. Our results suggested that the PD1 gene contributed to a genetic susceptibility to SSPE.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Subacute sclerosing panencephalitis (SSPE) is a fatal degenerative neuronal disease caused by persistent infection with a measles virus (MV), the nature of which is quite different from that of common wild types. The viruses isolated from SSPE brains, called SSPE viruses, are defective, and have extensive mutations within the envelope-associated genes, especially the M gene. While comparison of gene sequence between SSPE virus and clinical isolate of MV prevailing at roughly the same time and places as the primary infection in each patient indicated that they had a common origin (Rima et al. 1997; Ayata et al. 1998), there are specific mutations among SSPE viruses (Rima and Duprex 2005), which are considered to occur during the viral persistence in the brain. Their exact role in the pathogenesis of SSPE remains to be elucidated.
In addition to viral factors, host factors seem to contribute to the development of SSPE (Gascon 1996; Schneider-Schaulies et al. 1999). Epidemiologic studies have shown that contraction of measles before 2 years of age increases the risk of SSPE, suggesting that immaturity of the host immune system and central nervous system (CNS) plays an important role in host susceptibility for the development of SSPE. In previous studies, we demonstrated that the genotype combination of interleukin-4 gene promoter −589 TT and an allele of interferon regulatory factor 1 gene GT repeat polymorphism, and the homozygotes of −88 T allele of MxA gene encoding an antivirally active protein, MxA, were more frequent in SSPE patients than in controls (Inoue et al. 2002; Torisu et al. 2004), but these findings were not replicated in Filipinos probably due to a greater contribution of environmental factors (Pipo-Deveza et al. 2006).
Chronic infections are often characterized by varying degrees of functional impairment of virus-specific T cells, which is a principal reason for the inability of the host to eliminate the persisting pathogen. SSPE patients showed an impairment of MV-specific cytotoxic T cells (Dhib-Jalbut et al. 1988) and a defect in MV-specific interferon (IFN)-γ production (Hara et al. 2000). The ultimate fate of cellular immune responses is determined by the balance between positive and negative signals delivered by co-stimulatory and co-inhibitory molecules to T cells (Nurieva et al. 2006). The co-inhibitory pathways include cytotoxic T lymphocyte antigen 4 (CTLA-4)-CD80/CD86, as well as programmed cell death 1 (PD-1)-programmed cell death-ligand 1 (PD-L1)/PD-L2, and B and T lymphocyte attenuator (BTLA)-herpes virus entry mediator (HVEM) (Chen 2004). CTLA-4 functions as a master switch on T-cell activation/inactivation (Waterhouse et al. 1995). Recent reports indicate that PD-1 is markedly upregulated on surface of exhausted virus-specific CD8+ T cells in mice with lymphocytic choriomeningitis virus infection (Barber et al. 2006) and in humans with human immunodeficiency virus (HIV) infection (Day et al. 2006; Petrovas et al. 2006) and hepatitis C virus (HCV) infection (Golden-Mason et al. 2007; Penna et al. 2007).
It has been reported that common mutations of genes encoding co-inhibitory molecules influence susceptibility to chronic viral infections. CTLA4 genotypes were associated with the resolution of chronic hepatitis C virus infection (Yee et al. 2003) and progression of HIV-1 disease (Shao et al. 2006). CD80 genotypes were associated with cytotoxic immune responses in HCV infection (Saito et al. 2004). To determine the role of CTLA4, CD80, CD86, PD1, PDL1, PDL2, BTLA and HVEM genes as a host genetic factor for the development of SSPE, we have performed an association study on SNPs of these genes in the Japanese and Filipino SSPE patients and controls. Since a haplotype of the PD1 gene containing −606G allele showed a significant association with SSPE in both populations, we further investigated functional differences between PD1 promoter regions having −606G and −606A, and compared the gene expression levels of PD1 in peripheral blood mononuclear cells (PBMCs) between SSPE patients and controls.
Materials and methods
Subjects
The study population comprised 40 unrelated SSPE patients (27 males and 13 females) and 50 unrelated normal school children in Japan, and 60 (41 males and 19 females) SSPE patients and 120 unrelated children in Philippines. All the SSPE patients fulfilled the diagnostic criteria, that is, clinical features, increased MV antibody titer in the CSF, and typical EEG showing periodic slow wave complexes early in the disease. The mean age at onset of SSPE was 8.0 years (±3.1 SD) in Japanese and 9.7 years (±4.1 SD) in Filipino. Thirty-five (87.5%) Japanese patients had contracted natural measles occurring between ages 0.4 and 4 years (1.3 ± 0.9 years). The history of natural measles was unknown in the other five Japanese patients, including one with a history of live attenuated measles vaccination. Fifty (83.3%) Filipino patients had contracted measles between age 0.4 and 8 years of age, of which 36 (60%) contracted measles before age 2. Twenty patients (33%) received vaccination during infancy. The age of SSPE patients, when studied, ranged between 5 and 26 years (median 11 years, mean ± SD 12.4 ± 5.1 years) in Japanese and between 3 and 24 years (median 12 years, mean ± SD 11.5 ± 4.9 years) in Filipino. The Japanese controls were randomly selected from among normal school children around 10 years of age and were not matched for age. The Filipino controls were age- and sex-matched with SSPE cases. Informed consent was obtained from their parents. The current study was approved by the Ethics Committee of Kyushu University, Japan and the Research Implementation and Development Office of the University of the Philippines College of Medicine. For a quantitative RT-PCR, 28 Japanese SSPE patients (19 males, 9 females; 12.4 ± 5.1 years) whose cDNAs were available, and 16 age-matched controls (7 males, 9 females, 15.5 ± 9.0 years), were enrolled.
SNPs selection
We used data on common SNPs from HapMap (Japanese samples, October 2005 release) to identify tag SNPs except for those of PD1 gene. As genotype data of SNPs of PD1 gene were not available in HapMap database, we utilized those from our previous study and selected 4 SNPs (Ni et al., 2007). Tag SNPs were selected using the pairwise method with the program Tagger (de Bakker et al. 2005), an implement of HapMap website. The minimum allele frequency was set at 0.05 and r 2 threshold was set at 0.8. To include regulatory or possible promoter region, a margin of ~2,000 bp was taken around the transcribed region of each gene. We identified 4 tag SNPs of CTLA4, 17 of CD80, 7 of CD86, 10 of PDL1, 16 of PDL2, 3 of BTLA and 3 of HVEM. For CTLA4, we added CT60 (rs3087233) using the force includes option in the Tagger program because of their clinical interest (Ueda et al. 2003). We analyzed all tag SNPs of CTLA4, BTLA and HVEM. Among the tag SNPs of CD80 and CD86 genes, we selected one tag SNP located in the coding region of each gene based on the previous study (Matsushita et al. 2000). For PDL1 and PDL2 gene, we selected two tag SNPs each based on our previous data (Ni et al. 2007).
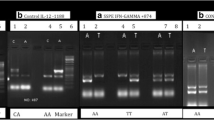
Genotype analysis of SNPs
Genomic DNA for SNP analysis was extracted from peripheral blood using a QIAmp DNA Blood Kit (Qiagen, Tokyo, Japan). Genotyping of each subject was performed by TaqMan method. TaqMan SNP Genotyping assay (Applied Biosystems, Foster City, CA, USA) was performed following the manufacturer’s instructions. PCR was carried out with mixes consisting of 8 ng of genomic DNA, 5 μl of TaqMan master mix, 0.5 μl of 20× assay mix and double distilled H2O up to 10 μl of final volume. The following amplification protocol was used: denaturation at 95°C for 10 min, followed by 40 cycles of denaturation at 92°C for 15 s, annealing, and extension at 60°C for 1 min. After PCR, the genotype of each sample was submitted automatically to the measurement of allelic specific fluorescence on the ABI PRISM 7700 Sequence Detection Systems using the SDS 2.2.2 software for allelic discrimination (Applied Biosystems).
Haplotype analysis of SNPs in the PD1 gene
We performed haplotype analysis using four SNPs in the PD1 gene. Haplotype frequencies were estimated using the Estimating Haplotype Frequencies (EH) software program (ftp://linkage.rockefeller.edu/software/rh). Linkage disequilibrium (LD) coefficients D′ values, Odd’s ratio and 95% confidence interval were calculated using data in the EH software program.
Functional analysis of PD1 gene promoter −606G/A
A fragment of the PD1 gene promoter (−1,225 to −65) having either −606G or −606A was amplified by PCR, using the following primers: 5′-GGAGTGGCCCTTGTTCATA-3′ (forward) and 5′-AACTGTCCCAGGTCAGGTTG-3′ (reverse). Each amplified fragment was inserted into the SacI and XhoI sites of a firefly luciferase-expressing plasmid, pGL4-luc2 vector (Promega, Madison, WI, USA). These plasmid constructs were verified by sequencing. Plasmids were purified using the EndoFree Plasmid Maxi Kit (Qiagen, Tokyo, Japan). HEK293 Cells were plated at 2 × 105 cells per well in 24-well plates. One day later, 200 ng of each plasmid construct and 20 ng of the Renilla luciferase control vector (pRL-TK) were transfected to the cells with Effectene (Qiagen, Crawley, UK). Luciferase activities in the transfected cells were measured using the Dual-Glo Luciferase Reporter Assay System (Promega) following the given protocol. Assays for the firefly and Renilla luciferase activities were performed sequentially using the MicroLumat Plus LB96V (Berthold, Bad Wildbad, Germany) as previously described (Sasaki et al. 2004). The values from three separate assays were compared between constructs.
The putative promoter region of PD1 gene was predicated using the TSSG (http://www.softberry.com/berry.phtml?topic=tssg&group=programs&subgroup=promoter). The nucleotide sequence of the PD1 gene promoter has been deposited in GenBank database under the accession number NT_005416.
Quantitative real-time PCR
Total RNA from peripheral blood mononuclear cells (PBMCs) was extracted using Isogen (Nippon Gene, Osaka, Japan) and first-strand cDNA was synthesized using a first-strand cDNA synthesis kit (Amersham Biosciences). We quantified mRNA by the TaqMan real-time RT-PCR method (Applied Biosystems, Foster City, CA, USA) using a Sequence Detector 7700 (Applied Biosystems). Each specimen was run in duplicate. A pre-developed TaqMan Assay kit was used for the PCR primers and a target probe for the PD1 gene (Assay ID; Hs00169472, Applied Biosystems) and GAPDH gene (Applied Biosystems).
Sequence analysis of the PD1 gene
We performed sequencing of the PD1 gene in 40 Japanese and 60 Filipino SSPE patients in order to seek mutations. The promoter region (about 1,000 bp), all exons and their flanking intronic areas (about 200–500 bps from the junctions) were amplified by PCR and analyzed by direct-sequencing with an ABI PRISM 3100 Genetic Analyzer (Perkin-Elmer, Foster City, CA, USA).
Statistical analyses
For SNP analysis, the Hardy–Weinberg equilibrium of alleles in controls was assessed by means of 2 × 2 χ2 statistics. Differences in the allele frequencies between two groups were evaluated by means of the χ2 analysis with a 2 × 2 contingency table. A P value of 0.05/4 (=0.0125), 0.05/3 (=0.017), 0.05/2 (=0.025) and 0.05 was considered to be significant, taking Bonferroni’s multiple adjustments into consideration of number of polymorphisms tested per gene. For comparison of promoter activities and relative gene expression levels, we applied Mann–Whitney U test.
Results
Association study of SNPs of genes encoding co-inhibitory molecules and haplotype analysis of PD1 gene in Japanese
The information of the analyzed SNPs are summarized in Table 1. The frequencies of each allele of the SNPs in Japanese SSPE patients and controls are shown in Table 2. The distributions of the genotypes in the controls were in Hardy–Weinberg equilibrium. The frequencies of G allele of rs36084323 and rs34819629 of the PD1 gene in SSPE patients were significantly higher than those in controls (P = 0.017 and P = 0.007, respectively). There were no significant differences in allele frequencies of SNPs of the other genes between SSPE patients and controls.
A significant LD was observed among four SNPs spanning 9.6 kb of PD1 gene in Japanese (D′ = 0.91–1.00). To investigate if a particular haplotype constituted by the four SNPs was associated with SSPE, haplotype frequencies were estimated and association analysis was done (Table 3). The LD block contained two major estimated haplotypes, GCGC and ATAT, accounting for about 95 and 92% of all haplotypes in the patients and the controls, respectively. We observed the frequency of GCGC haplotype was significantly higher in SSPE patients than in controls (P = 0.022, odds ratio: 1.5, confidence interval: 1.1–2.5) and ATAT haplotype was significantly lower in SSPE patients than in controls (P = 0.009, odds ratio: 2.1, confidence interval: 1.3–3.9).
Association study and haplotype analysis of PD1 gene in Filipinos
Since we observed a significant association between PD1 gene and SSPE in Japanese, we undertook SNP association study and haplotype analysis of PD1 gene in Filipino. The frequencies of each allele of the four SNPs of PD1 gene in Filipino SSPE patients and controls are shown in Table 4. There were no significant differences in allele frequencies of the four SNPs of PD1 genes between Filipino SSPE patients and controls. A significant LD (D′ = 0.86–0.96) was observed among three SNPs (rs36084323, rs35933396 and rs34819629) of PD1 in Filipinos. The block contained three major estimated haplotypes, GCG, ATA, and ATG, accounting for about 87 and 97% of all haplotypes in the patients and the controls, respectively (Table 3). We observed the frequency of GCG haplotype was significantly higher in Filipino SSPE patients than in controls (P = 0.01, odds ratio: 1.8, confidence interval: 1.1–3.9).
Transcription activity of the PD1 promoter
Since the frequencies of GCG(C) haplotype of the PD1 gene containing −606G allele were significantly different between the patients and the controls both in Japanese and Filipino, we investigated functional differences between PD1 promoter regions having −606G and −606A using a dual luciferase reporter assay. The promoter activities of the two constructs are shown in Fig. 1. The level of expression from the construct with the −606G allele was significantly higher than that from the construct with the −606A allele. These results indicated that −606G had higher PD1 promoter activity than −606A. According to TSSG, −606G/A SNP resides in the putative binding site for UCE.2 transcription regulators (GGCCG at position −610 to −606).

a Promoter activity differences between the PD1 −606 G and −606 A alleles. The −606 G allele was associated with higher promoter activity than the −606 A allele (*P < 0.001). Data are corrected for transfection efficiency, and represent the mean ± SD of three independent experiments with similar results. P values were from Mann–Whitney U test. b Sequence alignment of the promoter region of the PD1 gene. Putative transcription factor (UCE.2) binding site is underlined
Expression levels of the PD1 gene in PBMCs
The relative expression level of PD1 to GAPDH was significantly higher in the PBMCs from the SSPE patients than in those from the controls (P < 0.001; Mann–Whitney U test, Fig. 2).

Expression levels of PD1 in PBMCs from SSPE patients (n = 28) and normal controls (n = 16). Box and whisker plots show the 10th, 25th, 50th (median), 75th, and 90th percentile values. Log-transformed values of the relative expression level of PD1 to GAPDH are shown. The values in parentheses indicate the number of the samples. The relative expression levels of PD1 were significantly higher in SSPE patients than in controls (*P < 0.001). P values were from Mann–Whitney U test
Sequence analysis of the PD1 gene
No mutation was observed in the promoter region, exon-intron junctions and translated region of exons 1–5 of the PD1 gene in all SSPE patients, as compared with the registered genomic DNA sequence (GenBank accession number NT_005416.12).
Discussion
In the current study, we first demonstrated an association between the GCG(C) haplotype of the PD1 gene with high promoter activity and SSPE both in Japanese and Filipinos. We found that PD1 expression level in PBMCs was significantly increased in SSPE patients. These results support that PD-1 may be involved in the pathogenesis of SSPE.
The inhibitory receptor PD-1 (also called PDCD1 or CD279) is a member of the CD28 family and is inducibly expressed on T cells, natural killer T cells (NKT), B cells, monocytes and dendritic cells (DCs) (Chen 2004; Okazaki et al. 2002). PD-1 interacts with its ligands PD-L1 (CD274 or B7-H1) and PD-L2 (CD273 or B7-DC). PD-L1 is constitutively expressed on hematopoietic and nonhematopoietic cells, and in immunoprivileged sites (eye, placenta), and is highly expressed in inflammatory environments. Upon general activation of the immune response, professional antigen-presenting cells (APCs) and T cells further augment their PD-L1 expressions (Okazaki and Honjo 2006; Sharpe et al. 2007). By contrast, PD-L2 is inducibly expressed only on macrophages, DCs and bone marrow derived cultured mast cells (Ueda et al. 2003; Waterhouse et al. 1995). PD-1 is the only inhibitory receptor of the co-inhibitory molecules whose ligands are expressed both in lymphoid and nonlymphoid organs. This might explain why the PD1-PDL1 pathway has been postulated to regulate immune responses both in lymphoid and non-lymphoid organs including brain (Okazaki and Honjo 2006).
Polymorphisms in PD1 gene have been associated with several autoimmune diseases, including systemic lupus erythematosis (SLE), type 1 diabetes, rheumatoid arthritis and multiple sclerosis, suggesting a key function of PD-1 signaling in the pathogenesis of human autoimmune diseases (Ferreiros-Vidal et al. 2004; Kong et al. 2005; Kroner et al. 2005; Lin et al. 2004; Nielsen et al. 2003; Prokunina et al. 2002). An intronic SNP (PD-1.5, G7146A, rs11568821) in PD1 is located in a binding site for the transcription factor Runx1 and may regulate the amount or stability of PD-1 mRNA (Prokunina et al. 2002). This polymorphism, however, did not exist in Japanese population as well as Chinese population (Kong et al. 2005; Ni et al. 2007). Previous reports demonstrated that −606G/A (previously called PD-1.1 at −531G/A from the transcriptional start site) was associated with rheumatoid arthritis in Chinese (Kong et al. 2005). In this study, we demonstrated that a haplotype having −606G allele with high promoter activity was associated with the development of SSPE. We also performed sequence analysis of PD1 gene in Japanese and Filipino SSPE patients, but no mutations were identified in the promoter region, exons, and their flanking intronic sequences.
A line of evidence suggest that the PD-1–PD-L pathway plays a central role for the T cell dysfunction and lack of viral control in established chronic infection (Sharpe et al. 2007). PD-1-knockout mice exhibit better control of adenovirus infection (Iwai et al. 2003). PD-1 expression is up-regulated on exhausted virus-specific T cells causing reversible immune dysfunction and disease progression both in chronic lymphocytic choriomeningitis virus (LCMV) infection in mice (Barber et al. 2006) and HIV and chronic HCV infections in humans (Day et al. 2006; Golden-Mason et al. 2007; Penna et al. 2007; Petrovas et al. 2006). In the present study, relative PD1 expression in PBMCs was higher in SSPE patients than in controls, which was consistent with the higher frequency of GCG(C) haplotype with high promoter activity in SSPE patients. Although we did not examine the PD1 expression of MV-specific CD8+ T cells, the data suggest that PD1 may cause an impairment of the MV-specific immune response in SSPE patients.
MV seems to gain access to the CNS at the time of primary infection, as the MV genome was detected on reverse transcription PCR in CSF samples not only from patients with measles encephalitis and SSPE but also from those with acute measles (Nakayama et al. 1995). In SSPE brains, neurons, oligodendrocytes, astrocytes, and microvascular endothelial cells have been found to be infected (Allen et al. 1996). Impaired T cell response to MV might facilitate viral entry to and persistent replication in the CNS, which are the initial step and the chronic phase of persistent MV infection in the CNS, respectively. Persistent infection of LCMV clone 13 in mice caused immunosuppression and promoted the establishment of persistent MV infection in the CNS after subsequent MV challenge (Oldstone et al. 2005). LCMV has been shown to cause exhaustion of CD8+ T cells through up-regulation of PD-1 (Barber et al. 2006). Accordingly, individuals with GCG(C) haplotype with high promoter activity might be more susceptible to MV persistence in the CNS because MV-specific T cell response is likely to be precluded by excessive inhibitory signals from PD-1.
The limitation in this study includes the small sample sizes due to the rarity of SSPE whose incidence is estimated to be 0.1–6 cases per million population per year (Editorials 1990). Since the association detected between PD1 gene and SSPE in this study is significant but not strong enough to exclude the possibility of false-positive results due to the limitation of statistical power, studies with other larger samples would be needed to validate it.
In summary, among SNPs of the genes encoding co-inhibitory molecules, frequencies of GCG(C) haplotype of PD1 gene associated with high promoter activity were significantly higher in SSPE patients in Japanese and Filipinos. The expression levels of PD1 gene in PBMCs were significantly increased in Japanese SSPE patients. These findings indicated that PD1 might confer host genetic susceptibility to SSPE in both populations.
References
Allen IV, McQuaid S, McMahon J, Kirk J, McConnell R (1996) The significance of measles virus antigen and genome distribution in the CNS in SSPE for mechanisms of viral spread and demyelination. J Neuropathol Exp Neurol 55:471–480
Ayata M, Kimoto T, Hayashi K, Seto T, Murata R, Ogura H (1998) Nucleotide sequences of the matrix protein gene of subacute sclerosing panencephalitis viruses compared with local contemporary isolates from patients with acute measles. Virus Res 54:107–115
Barber DL, Wherry EJ, Masopust D, Zhu B, Allison JP, Sharpe AH, Freeman GJ, Ahmed R (2006) Restoring function in exhausted CD8 T cells during chronic viral infection. Nature 439:682–687
Chen L (2004) Co-inhibitory molecules of the B7-CD28 family in the control of T-cell immunity. Nat Rev Immunol 4:336–347
Day CL, Kaufmann DE, Kiepiela P, Brown JA, Moodley ES, Reddy S, Mackey EW, Miller JD, Leslie AJ, DePierres C, Mncube Z, Duraiswamy J, Zhu B, Eichbaum Q, Altfeld M, Wherry EJ, Coovadia HM, Goulder PJ, Klenerman P, Ahmed R, Freeman GJ, Walker BD (2006) PD-1 expression on HIV-specific T cells is associated with T-cell exhaustion and disease progression. Nature 443:350–354
de Bakker PI, Yelensky R, Pe’er I, Gabriel SB, Daly MJ, Altshuler D (2005) Efficiency and power in genetic association studies. Nat Genet 37:1217–1223
Dhib-Jalbut S, Jacobson S, McFarlin DE, McFarland HF (1988) Impaired measles-specific cytotoxic T-cell response in subacute sclerosing panencephalitis. Ann N Y Acad Sci 540:645–648
Editorials (1990) SSPE in the developing world. Lancet 336:600
Ferreiros-Vidal I, Gomez-Reino JJ, Barros F, Carracedo A, Carreira P, Gonzalez-Escribano F, Liz M, Martin J, Ordi J, Vicario JL, Gonzalez A (2004) Association of PDCD1 with susceptibility to systemic lupus erythematosus: evidence of population-specific effects. Arthritis Rheum 50:2590–2597
Gascon GG (1996) Subacute sclerosing panencephalitis. Semin Pediatr Neurol 3:260–269
Golden-Mason L, Palmer B, Klarquist J, Mengshol JA, Castelblanco N, Rosen HR (2007) Upregulation of PD-1 expression on circulating and intrahepatic hepatitis C virus-specific CD8+ T cells associated with reversible immune dysfunction. J Virol 81:9249–9258
Hara T, Yamashita S, Aiba H, Nihei K, Koide N, Good RA, Takeshita K (2000) Measles virus-specific T helper 1/T helper 2-cytokine production in subacute sclerosing panencephalitis. J Neurovirol 6:121–126
Inoue T, Kira R, Nakao F, Ihara K, Bassuny WM, Kusuhara K, Nihei K, Takeshita K, Hara T (2002) Contribution of the interleukin 4 gene to susceptibility to subacute sclerosing panencephalitis. Arch Neurol 59:822–827
Iwai Y, Terawaki S, Ikegawa M, Okazaki T, Honjo T (2003) PD-1 inhibits antiviral immunity at the effector phase in the liver. J Exp Med 198:39–50
Kong EK, Prokunina-Olsson L, Wong WH, Lau CS, Chan TM, Alarcon-Riquelme M, Lau YL (2005) A new haplotype of PDCD1 is associated with rheumatoid arthritis in Hong Kong Chinese. Arthritis Rheum 52:1058–1062
Kroner A, Mehling M, Hemmer B, Rieckmann P, Toyka KV, Maurer M, Wiendl H (2005) A PD-1 polymorphism is associated with disease progression in multiple sclerosis. Ann Neurol 58:50–57
Lin SC, Yen JH, Tsai JJ, Tsai WC, Ou TT, Liu HW, Chen CJ (2004) Association of a programmed death 1 gene polymorphism with the development of rheumatoid arthritis, but not systemic lupus erythematosus. Arthritis Rheum 50:770–775
Matsushita M, Tsuchiya N, Oka T, Yamane A, Tokunaga K (2000) New polymorphisms of human CD80 and CD86: lack of association with rheumatoid arthritis and systemic lupus erythematosus. Genes Immun 1:428–434
Nakayama T, Mori T, Yamaguchi S, Sonoda S, Asamura S, Yamashita R, Takeuchi Y, Urano T (1995) Detection of measles virus genome directly from clinical samples by reverse transcriptase-polymerase chain reaction and genetic variability. Virus Res 35:1–16
Ni R, Ihara K, Miyako K, Kuromaru R, Inuo M, Kohno H, Hara T (2007) PD-1 gene haplotype is associated with the development of type 1 diabetes mellitus in Japanese children. Hum Genet 121:223–232
Nielsen C, Hansen D, Husby S, Jacobsen BB, Lillevang ST (2003) Association of a putative regulatory polymorphism in the PD-1 gene with susceptibility to type 1 diabetes. Tissue Antigens 62:492–497
Nurieva R, Thomas S, Nguyen T, Martin-Orozco N, Wang Y, Kaja MK, Yu XZ, Dong C (2006) T-cell tolerance or function is determined by combinatorial costimulatory signals. EMBO J 25:2623–2633
Okazaki T, Honjo T (2006) The PD-1-PD-L pathway in immunological tolerance. Trends Immunol 27:195–201
Okazaki T, Iwai Y, Honjo T (2002) New regulatory co-receptors: inducible co-stimulator and PD-1. Curr Opin Immunol 14:779–782
Oldstone MB, Dales S, Tishon A, Lewicki H, Martin L (2005) A role for dual viral hits in causation of subacute sclerosing panencephalitis. J Exp Med 202:1185–1190
Penna A, Pilli M, Zerbini A, Orlandini A, Mezzadri S, Sacchelli L, Missale G, Ferrari C (2007) Dysfunction and functional restoration of HCV-specific CD8 responses in chronic hepatitis C virus infection. Hepatology 45:588–601
Petrovas C, Casazza JP, Brenchley JM, Price DA, Gostick E, Adams WC, Precopio ML, Schacker T, Roederer M, Douek DC, Koup RA (2006) PD-1 is a regulator of virus-specific CD8+ T cell survival in HIV infection. J Exp Med 203:2281–2292
Pipo-Deveza JR, Kusuhara K, Silao CL, Lukban MB, Salonga AM, Sanchez BC, Kira R, Takemoto M, Torisu H, Hara T (2006) Analysis of MxA, IL-4, and IRF-1 genes in Filipino patients with subacute sclerosing panencephalitis. Neuropediatrics 37:222–228
Prokunina L, Castillejo-Lopez C, Oberg F, Gunnarsson I, Berg L, Magnusson V, Brookes AJ, Tentler D, Kristjansdottir H, Grondal G, Bolstad AI, Svenungsson E, Lundberg I, Sturfelt G, Jonssen A, Truedsson L, Lima G, Alcocer-Varela J, Jonsson R, Gyllensten UB, Harley JB, Alarcon-Segovia D, Steinsson K, Alarcon-Riquelme ME (2002) A regulatory polymorphism in PDCD1 is associated with susceptibility to systemic lupus erythematosus in humans. Nat Genet 32:666–669
Rima BK, Duprex WP (2005) Molecular mechanisms of measles virus persistence. Virus Res 111:132–147
Rima BK, Earle JA, Baczko K, ter Meulen V, Liebert UG, Carstens C, Carabaña J, Caballero M, Celma ML, Fernandez-Muñoz R (1997) Sequence divergence of measles virus haemagglutinin during natural evolution and adaptation to cell culture. J Gen Virol 78:97–106
Saito T, Ji G, Shinzawa H, Okumoto K, Hattori E, Adachi T, Takeda T, Sugahara K, Ito JI, Watanabe H, Saito K, Togashi H, Ishii K, Matsuura T, Inageda K, Muramatsu M, Kawata S (2004) Genetic variations in humans associated with differences in the course of hepatitis C. Biochem Biophys Res Commun 317:335–341
Sasaki Y, Ihara K, Matsuura N, Kohno H, Nagafuchi S, Kuromaru R, Kusuhara K, Takeya R, Hoey T, Sumimoto H, Hara T (2004) Identification of a novel type 1 diabetes susceptibility gene, T-bet. Hum Genet 115:177–184
Schneider-Schaulies J, Niewiesk S, Schneider-Schaulies S, ter Meulen V (1999) Measles virus in the CNS: the role of viral and host factors for the establishment and maintenance of a persistent infection. J Neurovirol 5:613–622
Shao W, Lazaryan A, Dorak MT, Penman-Aguilar A, Wilson CM, Margolick JB, Goedert JJ, Prins M, Tang J, Kaslow RA (2006) Cohort- and time-specific associations of CTLA4 genotypes with HIV-1 disease progression. Aids 20:1583–1590
Sharpe AH, Wherry EJ, Ahmed R, Freeman GJ (2007) The function of programmed cell death 1 and its ligands in regulating autoimmunity and infection. Nat Immunol 8:239–245
Torisu H, Kusuhara K, Kira R, Bassuny WM, Sakai Y, Sanefuji M, Takemoto M, Hara T (2004) Functional MxA promoter polymorphism associated with subacute sclerosing panencephalitis. Neurology 62:457–460
Ueda H, Howson JM, Esposito L, Heward J, Snook H, Chamberlain G, Rainbow DB, Hunter KM, Smith AN, Di Genova G, Herr MH, Dahlman I, Payne F, Smyth D, Lowe C, Twells RC, Howlett S, Healy B, Nutland S, Rance HE, Everett V, Smink LJ, Lam AC, Cordell HJ, Walker NM, Bordin C, Hulme J, Motzo C, Cucca F, Hess JF, Metzker ML, Rogers J, Gregory S, Allahabadia A, Nithiyananthan R, Tuomilehto-Wolf E, Tuomilehto J, Bingley P, Gillespie KM, Undlien DE, Ronningen KS, Guja C, Ionescu-Tirgoviste C, Savage DA, Maxwell AP, Carson DJ, Patterson CC, Franklyn JA, Clayton DG, Peterson LB, Wicker LS, Todd JA, Gough SC (2003) Association of the T-cell regulatory gene CTLA4 with susceptibility to autoimmune disease. Nature 423:506–511
Waterhouse P, Penninger JM, Timms E, Wakeham A, Shahinian A, Lee KP, Thompson CB, Griesser H, Mak TW (1995) Lymphoproliferative disorders with early lethality in mice deficient in Ctla-4. Science 270:985–988
Yee LJ, Perez KA, Tang J, van Leeuwen DJ, Kaslow RA (2003) Association of CTLA4 polymorphisms with sustained response to interferon and ribavirin therapy for chronic hepatitis C virus infection. J Infect Dis 187:1264–1271
Acknowledgments
The authors thank Drs. H. Hattori (Osaka City University Medical School), S. Yamashita (Kanagawa Children’s Medical Center), K. Nihei (National Children’s Hospital), N. Koide (National Iwaki Hospital), H. Aiba (Shizuoka Children’s Hospital), T. Okada (Kochi Medical School), F. Hamada (Hosogi Hospital), N. Koyama (Toyohashi Municipal Hospital), Y. Hirata (Hamamatsu Medical Center), C. Baba (Red Cross Nagasaki Atomic Bomb Hospital), A.Ono (Saiseikai Izumio Hospital), A. Tomoda (Kumamoto University), M. Funahashi (Tokyo Children’s Rehabilitation Hospital), T. Kurokawa (National Nishi–Beppu Hospital), R. Sakuta (Dokkyo University Koshigaya Hospital), M. Miyazaki (Tokushima University), K. Shioya (National Nichinan Hospital), N. Nagano (Asahikawa City Hospital), T. Ishizu (National Saishunso Hospital), K. Gondo, Y. Tokunaga (Kyushu University), and K. Watanabe (Kagoshima Municipal Hospital) for providing patient samples. This study was supported in part by a Grant-in-Aid for Scientific Research from the Ministry of Education, Culture, Sports, Science and Technology (No. 16390304), Health and Labour Sciences Research Grant for Research on Measures for Intractable Diseases (Prion Disease and Slow Virus Infections) from the Ministry of Health, Labour and Welfare of Japan, and grants from National Institutes of Health and University of the Philippines, Manila, Philippines. This study was supported in part by a Grant-in-Aid for Scientific Research from the Ministry of Education, Culture, Sports, Science and Technology (No. 16390304), Health and Labour Sciences Research Grant for Research on Measures for Intractable Diseases (Prion Disease and Slow Virus Infections) from the Ministry of Health, Labour and Welfare of Japan, and grants from National Institutes of Health and University of the Philippines, Manila, Philippines. A part of results in this manuscript had been presented at the 12th annual meeting of Japanese Society for Neuroinfectious Diseases (October 12, 2007: Fukuoka, Japan).
Conflict of interest statement
The authors report no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ishizaki, Y., Yukaya, N., Kusuhara, K. et al. PD1 as a common candidate susceptibility gene of subacute sclerosing panencephalitis. Hum Genet 127, 411–419 (2010). https://doi.org/10.1007/s00439-009-0781-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00439-009-0781-z