
Abstract
Metastasis remains one of the major challenges before hepatocellular carcinoma (HCC) is finally conquered. This paper summarized a decade’s studies on HCC metastasis at the Liver Cancer Institute of Fudan University. We have established a stepwise metastatic human HCC model system, which included a metastatic HCC model in nude mice (LCI-D20), a HCC cell line with high metastatic potential (MHCC97), a relatively low metastatic potential cell clone (MHCC97L) and several stepwise high metastatic potential cell clones (MHCC97H, HCCLM3, and HCCLM6) from their parent MHCC97 cell. Endeavors have been made for searching human HCC metastasis-related chromosomes/proteins/genes. Monogene-based studies revealed that HCC invasion/metastasis was similar to that of other solid tumors, and the biological characteristics of small HCC were only slightly better than that of large HCC. Using comparative genomic hybridization (CGH), fluorescence in situ hybridization (FISH), genotyping, cDNA microarray, and 2-dimensional gel electrophoresis, we obtained some interesting results. In particular, in collaboration with the National Institute of Health (NIH) in the United States, we generated a molecular signature that can classify metastatic HCC patients, identified osteopontin as a lead gene in the signature, and found that genes favoring metastasis progression were initiated in the primary tumors. We also found that chromosome 8p deletion, particularly in the region of 8p23, was associated with HCC metastasis. Cytokeratin 19 was identified as one of the proteins, which was found in MHCC97H, but not in MHCC97L cells. Experimental interventions using the high metastatic nude mice model have provided clues for the prevention of HCC metastasis. Translation from workbench to bedside demonstrated that serum VEGF, microvessel density, and p53 scoring may be of value for the prediction of postoperative metastatic recurrence. Interferon alpha proved effective for the prevention of recurrence both experimentally and clinically. In conclusion, HCC metastasis that probably initiated in the primary tumor is a multigene-involved, multistep, and changing process. The further elucidation of the mechanism underlying HCC metastasis will provide a more solid basis for the prediction and prevention of the metastatic recurrence of HCC.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Liver cancer is the 3rd most common cause of death from cancer in the world. It has been estimated that there were 548,600 deaths from liver cancer in the year 2000 (Parkin et al. 2001). Unfortunately, the relative 5-year survival of liver cancer remains low; even in the United States, it was only 6% during the period of 1992–1997 (Jemal et al. 2002). In Shanghai, the relative 5-year survival of liver cancer in 1988–1991 was 4.4% (Jin et al. 1998).
Hepatocellular carcinoma (HCC) amounted to 90% of primary liver cancer in China. In recent decades, a gradual increase in 5-year survival has been observed in the inpatients at the authors’ institution. The major factors related to the improvement of survival include small HCC resection and downstaging, followed by resection for initially unresectable HCC (Tang 2003). Unfortunately, the recurrence rate remains high after HCC resection. We reported that the 5-year recurrence rate after curative resection was as high as 61.5% (Tang et al. 1984); even after small HCC resection, it was 43.5% (Tang 1989). Determined by integration of hepatitis B virus DNA and analysis of p53 genotype, we demonstrated that both unicentric and multicentric origins existed in recurrent lesions (Liang et al. 1991; He et al. 1996). Our studies focus on the recurrence that originated from metastasis (unicentric origin). Ten years have gone by since we published the first paper related to HCC metastasis (Jiang et al.1994); much has been done and much remains to be done (Tang et al. 1999). An overview on HCC metastasis studies at the Liver Cancer Institute of Fudan University is presented in this paper.
Materials and methods
Experimental studies included the establishment of a metastatic human HCC model in nude mice and cell lines with metastatic potential; molecular events related to HCC invasion/metastasis; the search for human HCC metastasis-related chromosomes/proteins/genes; microenvironment and HCC invasion, as well as experimental intervention of metastasis.
The methodology included comparative genomic hybridization (CGH), fluorescence in situ hybridization (FISH), genomic microsatellite analysis, cDNA microarray, 2-dimensional gel electrophoresis, immunohistochemistry, polymerase chain reaction (PCR) and others.
Translation from workbench to bedside, including the prediction of metastatic recurrence and prevention of recurrence after curative HCC resection, is also described. Related papers published by the authors’ institution in the last decade are selectively cited. The latest results in this particular field at the authors’ institution are also selectively included.
Experimental studies on gene therapy and tumor vaccine have also been conducted at the authors’ institution; however, most of the experiments were not performed directly in metastatic HCC models, and therefore will not be included in this paper.
Results
Establishment of a stepwise metastatic human HCC model system
Using the orthotopic implantation of 30 surgical specimens of histologically intact tissues, a highly metastatic model of human HCC in nude mice (LCI-D20) was successfully established. A low metastatic model (LCI-D35) was also established as control. All mice with transplanted LCI-D20 tumors exhibited extremely high metastatic ability as well as various manifestations of tumor behavior in HCC patients, including local growth, regional invasion, spontaneous metastasis to liver, lungs, lymph nodes, and peritoneal seeding. High expression of invasion related genes, such as c-fos, c-jun, N-ras, H-ras, and p53 mutation were found in the LCI-D20 model but not in the LCI-D35 model (Sun et al. 1996; He et al. 1997). Changes of serum and tissue levels of plasminogen activator inhibitor-1 (PAI-1) were correlated with tumor progression of the LCI-D20 model (Zheng et al. 1998a). N-acetylglucosaminyltransferase V activity was found to increase in the LCI-D20 model during metastasis (Shao et al. 1999). Using a corneal micropocket model, the vascular response induced by the tumor from the LCI-D20 model was stronger than that of the LCI-D35 model (Sun et al. 1999a). A human HCC cell line with metastatic potential (MHCC97) was then established with the tumor from the LCI-D20 model, which was also not yet found in the literature. Upon subcutaneous or intrahepatic inoculation in nude mice, the xenograft grew and metastasized to lungs (100%). The median range of chromosome number was 60–61 (Tian et al.1999). In order to search for HCC metastasis-related chromosomes/proteins/genes, a stepwise metastatic human HCC model system, with a similar genetic background including a high metastatic subclone (MHCC97H) and a low metastatic subclone (MHCC97L), was successfully established through in vivo selection of MHCC97, and two even higher metastatic potential cell lines (HCCLM3 and HCCLM6) were established from MHCC97H (Li et al. 2001; Li et al. 2003). The metastatic behavior of these cell lines is summarized in Table 1.
The role of single genes in HCC invasion/metastasis
During the 1990s, endeavors were made to clarify the role of genes that related to invasion/metastasis of other solid tumors in HCC metastasis. The results of these monogene-based studies can be summarized as: (1) the molecular events of HCC invasion/metastasis were similar to that of other solid cancers. Genes that positively related to invasion/metastasis included: p53 mutation (Qin et al. 1995), p16 mutation (Qin et al. 1996), H-ras, mdm2 (Qiu et al. 1998), c-erbB-2, transforming growth factor alpha (TGFα) and epidermal growth factor receptor (EGF-R, Wang et al. 1995), matrix metalloproteinase-2 (MMP-2, Bu et al. 1997), urokinase-type plasminogen activator (uPA), its receptor (uPA-R) and inhibitor (PAI-1, Zheng et al. 2000), intercellular adhesion molecule-1 (ICAM-1, Sun et al. 1999), vascular endothelial growth factor (VEGF, Li et al. 1998a), platelet-derived endothelial cell growth factor (PD-ECGF, Zhou et al. 2000a), basic fibroblast growth factor (bFGF, Niu et al. 2000b), etc. Elevated activity of N-acetylglucosaminyltransferase V in human HCC was also observed (Yao et al.1998a). Factors that negatively related to HCC invasion included: nm23-H1 (Zheng et al. 1998; Ye et al. 1998), Kai-1 (Sun et al. 1998), tissue inhibitor of metalloproteinase-2 (TIMP-2), integrin α5 (Yao et al. 1997), E-cadherin (Yao et al. 1998b), etc. Unfortunately, we failed to demonstrate any of the genes mentioned above that specifically related to HCC invasion/metastasis; (2) the studies on the molecular level showed that the expression rates of genes that positively related to HCC invasion was only slightly lower in small HCC than in large HCC, and genes that negatively related to HCC invasion were only slightly higher in small HCC than in large HCC (Table 2), which indicated that the effectiveness of early detection and early treatment of HCC is limited by the biological characteristics of HCC even in patients with small HCC (Tang et al. 1998).
Search for HCC metastasis related chromosomes/proteins/genes
We collaborated with the National Institute of Health (NIH) of the United States, using comparative genomic hybridization (CGH), compared the difference of chromosomal aberrations between primary HCC tumors and their matched metastatic lesions, and found that chromosome 8p deletion was much more frequent in metastatic lesions compared with primary tumors, suggesting that chromosome 8p might comprise some tumor (metastasis) suppressor genes (Qin et al. 1999). Chromosome 8p deletion was also found to be associated with the metastasis of human HCC when the high (LCI-D20) and low (LCI-D35) metastatic models were compared (Qin et al. 2001). A complete genomic imbalance profile in relation to HCC metastasis from the comparative whole genome microsatellite analysis between the primary tumors and matched metastatic lesions of HCC indicated that 8p (8p23.3 and 8p11.2) remains one of the important locations for further study (Zhang et al. 2003). The comparison of molecular cytogenetic characteristics between the two cell lines with different metastatic potentials (MHCC97L and MHCC97H) using CGH and FISH, also suggested that 8p23 might harbor some novel genes related to the HCC metastasis (Yang et al. 2003). Recently, using the microcell-mediated chromosomal transfer (MMCT) technique, we successfully introduced human chromosome 8 into a highly metastatic rat liver cancer cell line and found it could significantly suppress the metastasis of liver cancer, which formed the basis for seeking functional evidence of a metastasis suppressor gene for liver cancer harboring on human chromosome 8 (Liu et al. 2003). We also demonstrated that the expression levels of TEY1 gene, a metastasis suppressor gene for prostate cancer located on 8p, were negatively correlated with the metastatic potentials of HCC cell lines (Liu et al. 2002).
Another even more interesting story also arose from collaboration with the National Cancer Institute (NCI, NIH) in the United States. We analyzed the expression profiles of HCC samples without or with intra-hepatic metastases with the cDNA microarray. Using a supervised machine-learning algorithm, we generated for the first time a molecular signature (with 153 significant genes) that could classify metastatic HCC patients. We found that genes favoring metastasis progression were initiated in the primary tumors. Osteopontin, which was identified as a lead gene in the signature, was over-expressed in metastatic HCC; an osteopontin-specific antibody effectively blocked HCC cell invasion in vitro and inhibited pulmonary metastasis of HCC cells in nude mice. Thus, osteopontin may have potential as a predictor and therapeutic target for metastatic HCC (Ye et al. 2003).
The comparison of gene expression profiles between HCCLM3 and MHCC97L, two clonal cell strains from the same parental cell line but with different metastatic potentials, was also performed by cDNA microarray. Twenty-five differentially expressed genes were identified in HCCLM3, including the decreased expression of Rb2 and increased expression of MAP kinase (Li et al. 2003).
Recently, a comparison of the protein profiles between MHCC97L and MHCC97H was performed using 2-dimensional gel electrophoresis. Cytokeratin 19 (CK19) was identified as one of the most interesting proteins, which was found in MHCC97H, but not in MHCC97L cells. The serum CK19 level correlated well with lung metastasis of the LCI-D20 model, and the increased serum level of CK19 was also associated with the incidence of portal vein tumor embolus in patients with HCC (Li et al. to be published).
Microenvironment and HCC metastasis
The Lung is the most common site of extrahepatic metastasis of HCC. In comparison to the extracts of liver, spleen, and kidney, lung extracts showed a significant ability to promote the migration and invasion of MHCC97H cells. The difference in metastatic ability between MHCC97H and MHCC97L cells was associated with the secretion level of MMPs; lung extracts could upregulate MMPs and pseudopodia formation in these cell lines. An unknown protein H5 with a molecular weight of 291,400 Daltons was preliminary identified as an active molecule in lung extract (Ji et al. 2003).
Experimental intervention using the LCI-D20 model
HCC is mostly a hypervascular tumor, therefore anti-angiogenesis is an important approach for experimental intervention. Several anti-angiogenic agents have been tried in the LCI-D20 model.
-
1.
The inhibitory effect of the angiogenesis inhibitor TNP-470, a fumagillin derivative, on tumor growth (tumor weight being 0.97 g vs 2.04 g in the control) and lung metastasis (8% vs 50%) was demonstrated (Xia et al. 1997).
-
2.
Suramin inhibited tumor growth and metastasis. Compared with control, the tumor volume of the treated mice was much smaller (7.5 vs 10.8 cm3), and lung metastasis rate was decreased (62.5% vs 100%) (Li et al. 1998b).
-
3.
Transfection of dominant-negative flk-1(VEGF receptor) mutant gene showed inhibition of angiogenesis, tumor growth, and metastases. The tumor was tenfold smaller than the control, the lung metastasis rate was decreased from 100% to 20%, and blood vessels were hardly visible as compared with rich neovascularization in the control (Li et al. 1998c).
-
4.
Endostatin also inhibited tumor growth, and the combination with cisplatin enhanced the response. The mean tumor volume (mm3) was 8,376 for the control, 3,777 for endostatin, 1,629 for cisplatin, and 463 for endostatin combined with cisplatin, respectively (Sun et al. 1999b).
-
5.
Cytostatic calcium influx inhibitor carboxyamido-triazole (CAI) also was demonstrated as having an anti-angiogenesis effect(Li et al. 1999a).
-
6.
Interferon alpha1b (IFN alpha) was effective in preventing recurrence in the liver and inhibiting lung metastasis after tumor resection in the liver of the LCI-D20 model in a dose-dependent manner. The mechanism was mediated by anti-angiogenesis (Wang et al. 2000a).
Other experimental intervention using the LCI-D20 model
-
1.
Metalloproteinase inhibitor-BB94 inhibited tumor growth and metastasis. The tumor weight was 2.27 g vs 3.13 g, lung metastasis 44% vs 100%, and survival on day 45 was 100% vs 56%, compared with the control (Bu et al. 1998).
-
2.
Antisense H-ras oligodeoxynucleotides inhibited H-ras expression, induced apoptotic cell death, inhibited the growth rate of LCI-D20 cells in vitro and in vivo, and altered in vivo tumorigenicity (50% vs 100%) and metastatic potential (lung metastases 0% vs 100%) (Liao et al. 2000).
-
3.
Heparin is structurally and functionally similar to that of heparan sulfate, a metabolite of suramin. Heparin inhibited tumor growth (tumor size being 1.50±0.61 cm vs 2.98±0.50 cm in the control), inhibited lung metastasis (20% vs 60%) and prolonged survival (50-day survival 60% vs 0%) (Zheng et al. 1998b).
-
4.
PD-ECGF, which is expressed in HCC, and particularly in tumor thrombus, is able to convert more prodrug (such as Furtulon and capecitabine) into 5-Fu. Using the LCI-D20 model, the lung metastatic rate was 17% in the capecitabine group, 50% in the Furtulon group, and 100% in the 5-Fu and control groups (Zhou et al. 2000b).
-
5.
The inhibitory effects of syntheticβpeptide, a polypeptide that blocks ICAM-1, on invasion and metastasis of liver cancer was demonstrated; when the tumor was resected at an early stage, the lung metastatic rate was 0% compared with 80% in the control (Sun et al. 2000).
-
6.
Cell differentiation agent (CDA-II) also inhibited metastasis in a dose-dependent manner. The down-regulation of the expression of c-myc, N-ras, c-jun, c-fos, mmp-9, integrin β1, and up-regulation of E-cadherin were observed (Liu et al. 2002). Unfortunately, all-trans retinoic acid alone was not effective in inhibiting metastasis in the LCI-D20 model (Wang et al. 2000b).
Translation from workbench to bedside
Studies on the molecular events of HCC metastasis provide clues regarding the development of biomarkers for prediction as well as new targets for the treatment and prevention of metastatic recurrence. Unfortunately, only a few aspects have been translated into clinical routine.
The following blood tests have been tried with potential clinical implications as predictors of metastatic recurrence: AFP mRNA (Wu et al. 2003), thrombomodulin (Zhou et al.2001), MMP-2 (Niu et al.2001), ICAM-1 (Sun et al.1998), PAI-1 (Zheng et al.1999), VEGF (Li et al.1999b; Niu et al.2000a), bFGF (Niu et al. 2000b), etc. Serum ICAM-1 content was higher in patients with metastasis than in those without metastasis (Sun et al. 1999). The combination of several of the items mentioned above increased sensitivity.
Using immunohistochemistry for tumor tissue samples, we found that microvessel density, p53 mutation, p16 mutation, nm23-H1, Kai-1, MMP-2, uPA, ICAM-1, VEGF, and PD-ECGF were of potential use as predictors of metastatic recurrence. Of these, microvessel density (MVD) using anti-CD34 staining related well to the prognosis of small HCC resection; the 5-year disease-free survival of hypovascular HCC was 74.6%, whereas it was only 34.7% in hypervascular HCC (Sun et al. 1999c). The immunohistochemistry scoring of p53 was also demonstrated as an independent prognostic marker for HCC resection (Qin et al. 2002a).
Based on the findings of experimental intervention using IFN alpha, a randomized control trial using long-term IFN alpha 1b (5 μg tiw×18 months, n=117) showed increased overall 3-year survival (82.4% versus 69.4%) and disease-free 3-year survival (55.4% versus 47.8%) after curative resection of HCC as compared with the control (n=116) (Sun et al. to be published).
Discussion
In the past 10 years, studies covering many aspects of HCC metastasis have been conducted at the authors’ institution. Unfortunately, only a few aspects have been translated from the workbench to bedside. Therefore, we still have a long way to go before HCC metastasis is finally conquered.
The impact of the establishment of a metastatic human HCC model system
In the literature, a human HCC model in nude mice with metastatic behavior as well as a human HCC cell line with metastatic potential has been rarely reported. An earlier report of a liver metastatic model of human HCC in nude mice showed that metastasis was mainly found in the liver (Aruga et al. 1993). Another previous report of a human HCC cell line with metastatic potential showed that metastasis was found in lymph nodes (Seki et al. 1999).
At the authors’ institution, human HCC models in nude mice were established in the early 1980s. However, metastatic behavior was not demonstrated in that model (Tang and Ma 1989). In order to carry out studies on HCC metastasis, we needed a patient-like model with metastatic potential. We published our metastatic human HCC nude mice model in 1996 (Sun et al. 1996) and the HCC cell line with metastatic potential in 1999 (Tian et al. 1999). Later, we found that the establishment of a stepwise metastatic human HCC model system (Li et al. 2001; Li et al. 2003) provided a platform for the study of the mechanism of HCC metastasis, for searching HCC metastasis-related chromosomes/proteins/genes, for studies on the interaction between the microenvironment and HCC invasion, as well as HCC metastasis interventions. These models will provide the possibility of investigating HCC metastasis-related genes without the influence of genetic background.
Approaches to searching HCC metastasis-related chromosomes/proteins/genes
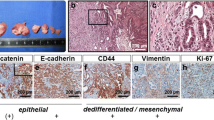
Both the prediction and intervention of HCC metastasis depend on the identification of HCC metastasis-related chromosomes/proteins/genes. Starting in the late 1990s, our strategies changed from a monogene-based study to multigene alteration. Two approaches have been tried: (1) comparisons between HCC without metastasis, HCC with metastasis, and its primary and metastatic lesions (Fig. 1). The merit is that tissue samples were taken directly from patients with different metastatic potentials. As shown in our data, the major difference was found between HCC without metastasis and HCC with metastasis, and only minor differences were found between primary and metastatic lesions of HCC with metastasis. The demerit, however, is that it is difficult to exclude the influence of other kinds of cells or extracellular components, as well as the genetic background of different cell populations; (2) comparisons among human HCC cell lines with similar genetic background but different metastatic potentials (Fig. 2). The influence from other kinds of cells/extracellular components, and particularly the genetic background of the cell population is excluded. Unfortunately, it is difficult to develop a subclone without metastatic potential from a metastatic cell line. It is our opinion that both approaches can be used, at least at the moment. To sum up, the picture shows that HCC metastasis is probably initiated in the primary tumor, but minor changes with further progression could still be found even in different passages of the same cell line.


In recent literature, the reported genetic alteration of HCC mainly focussed on hepatocarcinogenesis (Collonge-Rame et al. 2001; Wang et al. 2001; Xu et al. 2001), and particularly on chromosome 17p13.3 (Zhao et al. 2001; Zhao et al. 2003). For HCC progression and metastasis, there are only a few papers; for example, 13q might play an important role in contributing to a more aggressive tumor behavior (Wong et al. 2002). A possible link between the size of the tumor and the burden of genetic changes was also reported (Kitay-Cohen et al. 2001). Molecular cytogenetic information provided by CGH was claimed to be useful for estimating the prognosis of patients with HCC (Kusano et al. 2002). Proteomics will be an important approach (Seow et al. 2001; Kim et al.2002), but complicated.
Interaction between the microenvironment and HCC invasion
The establishment of a stepwise metastatic model system was achieved mainly through an in vivo selection from lung metastatic lesions. In other words, the gradual change of multigene expression resulted, in part, from the influence of the lung microenvironment. We demonstrated that the lung extract (with an unknown protein H5), but not spleen extract, was able to enhance the motility of MHCC97H as well as pseudopodia formation, which can explain the reason for lung-targeted metastasis. Recently, chemokines and their receptors were claimed to play a critical role in determining the metastatic destination in breast cancer (Muller et al. 2001). Therefore, the interaction between the microenvironment and HCC invasion will be an important study area.
Expectations on predictors of HCC metastasis/prognosis
In late 1990s and early 21st century, biomarkers covering many aspects have been claimed as having the potential to predict metastatic recurrence, particularly those appearing in blood stream, such as AFP mRNA (Wong et al. 1999; Ijichi et al. 2002), anti-p53 (Saffroy et al. 1999), VEGF (Jinno et al. 1998a; Poon et al. 2001a), PD-ECGF (Jinno et al.1998b), bFGF (Poon et al. 2001b), MAGE-1 and MAGE-3 (Mou et al. 2002), telomerase (Kobayashi et al. 2001), mitochondrial DNA (Okochi et al. 2002), etc. However, adverse results have also been reported, such as AFP mRNA (Witzigmann et al. 2002), ICAM-1, and anti-p53 (Parasole et al. 2001). It is understandable that monogene-based studies reflect the complexity of cancer invasion/metastasis with difficulty. The progress of cDNA microarray technology has provided a platform for multigene-based studies and has been employed in the study of cancer metastasis (Clark et al.2000). As shown in the above results, using cDNA microarray, by comparing MHCC97L and HCCLM3, a clonal strain from the same parental cell line but with higher metastatic potential, we were able to identified 25 differentially expressed genes including cell cycle control gene (Rb2), mismatch repair gene (hMSH2), signal transduction gene (protein kinase Cβ2), etc (Li et al.2003). Again, using cDNA microarray, we generated for the first time a molecular signature (with 153 significant genes) that can classify metastatic HCC patients, osteopontin being the lead gene (Ye et al. 2003). Overexpression of osteopontin associated with intrahepatic metastasis, early recurrence, and the poorer prognosis of surgically resected HCC has also appeared in recent literature (Pan et al. 2003). A gene-expression signature with a 70-gene prognosis profile was also reported as a more powerful predictor of prognosis in young patients with breast cancer (van de Vijver et al. 2002). These will probably provide a more better approach to the prediction of HCC metastasis. Summarizing the recent literature, it seems that circulating DNA in plasma and its genetic alteration, with multigene involvement, are two areas of importance (Qin et al. 2002b).
New targets for the intervention of HCC metastasis
Prevention of metastatic recurrence after HCC resection is the major goal for the further improvement of HCC prognosis. Unfortunately, only very few things have been tested through randomized control trials to be of benefit, namely: interferon beta and interferon alpha for HCV-related HCC (Ikeda et al. 2000; Kubo et al. 2002), acyclic retinoic for the prevention of second primary tumors with HCC (Muto et al. 1996; Muto et al. 1999), adoptive immunotherapy (Takayama et al. 2000), and iodine-131-labeled lipiodol (Lau et al. 1999). A review of 13 randomized clinical trial indicated that benefit in terms of survival was noted in six trials, five of which involved modalities other than systemic or hepatic artery chemotherapy or embolisation, including immunological, radiation, and differentiation agents as mentioned above (Schwartz et al. 2002). However, a multicentre trial is still needed (Sun et al. 2003). Meta-analysis showed that adjuvant chemotherapy after resection of HCC even causes deterioration of prognosis in cirrhotic patients (Ono et al. 2001).
Therefore, endeavors in the past decade have focused on identifying the molecular and genetic changes that cause HCC metastasis. These findings could be attractive regarding the development of anti-metastasis treatments. Our data on the experimental intervention on the LCI-D20 model have provided clues with clinical impact. Unfortunately, many stones still remain unturned regarding gene therapy. Recently, “inhibiting HER2 (erbB-2) to treat breast cancer” has been claimed as “the beginning of an important new era in cancer treatment” directed against a molecular determinant that causes malignant transformation (Eisenhauer et al. 2003).
Anti-angiogenesis is one of the important approaches for the control of metastatic recurrence. We also prove that IFN alpha prevents recurrence after curative resection of HCC mediated by anti-angiogenesis. However, the angiogenesis inhibitors, by depriving tumors of oxygen, could have an unintended effect: promotion of metastasis (Steeg 2003).
Conclusion
Based on the studies mentioned above, HCC metastasis that probably initiated in the primary tumor is a multigene-involved, multistep, and changing process, and varies with different metastatic phenotypes. HCC invasion might include genetic alterations in many locations of chromosomes. Chromosome 8p and 17p deserve further investigation. A combination of multiple molecular alterations has significant implications for the prediction of metastatic recurrence. The need to speed-up the process of translating findings from the workbench to bedside is emphasised, particularly those regarding the intervention of HCC metastasis.
References
Aruga A, Takasaki K, Hanyu F (1993) Establishment and characterization of liver metastatic model of human hepatoma in nude mice. Int Hepatol Commun 1:138–145
Bu W, Huang XW, Tang ZY (1997) The role of MMP-2 in the invasion and metastasis of hepatocellular carcinoma. Zhonghua Yixue Zazhi (Natl Med J China) 77:661–664 (Chin)
Bu W, Tang ZY, Sun FX, Ye SL, Liu KD, Xue Q, Chen J, Gao DM (1998) Effects of matrix metalloproteinase inhibitor BB-94 on liver cancer growth and metastasis in a patient-like orthotopic model LCI-D20. Hepato-Gastroenterol 45:1056–1061
Clark EA, Golub TR, Lander ES, et al (2000) Genomic analysis of metastasis reveals an essential role for RhoC. Nature 406:532–535
Collonge-Rame MA, Bresson-Hadni S, Koch S, Carbillet JP, Blagosklonova O, Mantion G, Miguet JP, Heyd B, Bresson JL (2001) Pattern of chromosomal imbalances in non-B virus related hepatocellular carcinoma detected by comparative genomic hybridization. Cancer Genet Cytogenet 127:49–52
Eisenhauer EA (2003) From the molecule to the clinic- Inhibiting HER2 to treat breast cancer (editorial) N Engl J Med 344:841–842
He B, Tang ZY, Liu KD, Zhou G (1996) Analysis of the cellular origin of hepatocellular carcinoma by p53 genotype. J Cancer Res Clin Oncol 122:763–766
He B, Liu YK, Tang ZY, Xue Q (1997) Gene mutation and expression in metastatic model of human hepatocellular carcinoma in nude mice established by orthotopic implantation. Zhonghua Ganzangbing Zazhi (Chin J Hepatol) 5:245–245 (Chin)
Ijichi M, Takayama T, Matsumura M, Shiratori Y, Omata M, Makuuchi M (2002) alpha-Fetoprotein mRNA in the circulation as a predictor of postsurgical recurrence of hepatocellular carcinoma: a prospective study. Hepatology 35:853–860
Ikeda K, Arase Y, Saitoh S, Kobayashi M, Suzuki Y, Suzuki F, Tsubota A, Chayama K, Murashima N, Kumada H (2000) Interferon beta prevents recurrence of hepatocellular carcinoma after complete resection or ablation of the primary tumor—a prospective randomized study of hepatitis C virus-related liver cancer. Hepatology 32:228–232
Jemal A, Thomas A, Murray T, Thum M (2002) Cancer statistics, 2002. CA Cancer J Clin 52:23–47
Ji XN, Ye SL, Li Y, Tian B, Chen J, Gao DM, Bao WH, Liu YK, Tang ZY (2003) Contribution of lung tissue extracts to invasion and migration of human hepatocellular carcinoma cells with various metastatic potentials. J Cancer Res Clin Oncol 129:556–564
Jiang XP, Liu KD, Zhou XD, Tang ZY, Zhang ZF, Zhang Y, Wu XF (1994) Identification of a new human nm23 gene, nm 23-H3b. Chin J Cancer Res 6:18–23
Jin F, Xiang YB, Gao YT (1998) Cancer survival in Shanghai, People’s Republic of China. In: Sankaranaryanan R, Black RJ, Parkin DM (eds) Cancer survival in developing countries. IARC Scientific Publication No. 145. IARC, Lyon, pp. 37–50
Jinno K, Tanimizu M, Hyodo I, Nishikawa Y, Hosokawa Y, Doi T, Endo H, Yamashita T, Okada Y (1998a) Circulating vascular endothelial growth factor (VEGF) is a possible tumor marker for metastasis in human hepatocellular carcinoma. J Gastroenterol 33:376–382
Jinno K, Tanimizu M, Hyodo I, Nishikawa Y, Hosokawa Y, Endo H, Doi T, Mandai K, Ishitsuka H (1998b) Circulating platelet-derived endothelial cell growth factor increases in hepatocellular carcinoma patients. Cancer 82:1260–1267
Kim J, Kim SH, Lee SU, Ha GH, Kang DG, Ha NY, Ahn JS, Cho HY, Kang SJ, Lee YJ, Hong SC, Ha WS, Bae JM, Lee CW, Kim JW (2002) Proteome analysis of human liver tumor tissue by two-dimensional gel electrophoresis and matrixassisted laser desorption/ionization-mass spectrometry for identification of disease-related proteins. Electrophoresis 23:4142–4156
Kitay-Cohen Y, Amiel A, Ashur Y, Fejgin MD, Herishanu Y, Afanasyev F, Bomstein Y, Lishner M (2001) Analysis of chromosomal aberrations in large hepatocellular carcinomas by comparative genomic hybridization. Cancer Genet Cytogenet 131:60–64
Kobayashi T, Kubota K, Takayama T, Makuuchi M (2001) Telomerase activity as a predictive marker for recurrence of hepatocellular carcinoma after hepatectomy. Am J Surg 181:284–288
Kubo S, Nishiguchi S, Hirohashi K, Tanaka H, Shuto T, Kinoshita H (2002) Randomized clinical trial of long-term outcome after resection of hepatitis C virus-related hepatocellular carcinoma by postoperative interferon therapy. Br J Surg 89:418–422
Kusano N, Okita K, Shirahashi H, Harada T, Shiraishi K, Oga A, Kawauchi S, Furuya T, Sasaki K (2002) Chromosomal imbalances detected by comparative genomic hybridization are associated with outcome of patients with hepatocellular carcinoma. Cancer 94:746–751
Lau WY, Leung TW, Ho SK, Chan M, Machin D, Lau J, Chan AT, Yeo W, Mok TS, Yu SC, Leung NW, Johnson PJ (1999) Adjuvant intra-arterial iodine-131-labelled lipiodol for resectable hepatocellular carcinoma: a prospective randomised trial. Lancet 353:797–801
Li XM, Tang ZY, Zhou G, Liu YK, Ye SL (1998a) Significance of vascular endothelial growth factor mRNA expression in invasion and metastasis of hepatocellular carcinoma. J Exp Clin Cancer Res 17:13–17
Li XM, Tang ZY, Xue Q, Liu YK, Ye SL, Zhang XR, Zhao ZH (1998b) Suramin inhibits growth and metastasis of human hepatocellular cacinoma in nude mice. Zhonghua Shiyan Waike Zazhi (Chin J Exp Surg) 15:3–4 (Chin)
Li XM, Tang ZY, Chen FG (1998c) Gene transfer of dominant-negative flk-1 mutant inhibits angiogenesis, growth and metastases of human hepatocellular carcinoma in nude mice. Zhongguo Zhongliu Shengwu Zhiliao Zazhi (Chin J Cancer Biother) 5:160–162 (Chin)
Li XM, Sun HC, Tang ZY, Zhou J (1999a) Cytostatic calcium influx inhibitor carboxyamido- triazole inhibited angiogenesis induced by human hepatocellular carcinoma. Zhonghua Shiyan Waike Zazhi (Chin J Exp Surg) 16:489–490 (Chin)
Li XM, Tang ZY, Qin LX, Zhou J, Sun HC (1999b) Serum vascular endothelial growth factor is a predictor of invasion and metastasis in hepatocellula rcarcinoma. J Exp Clin Cancer Res 18:511–517
Li Y, Tang ZY, Ye SL, Liu YK, Chen J, Xue Q, Chen J, Gao DM, Bao WH (2001) Establishment of cell clones with different metastatic potential from the metastatic hepatocellular carcinoma cell line MHCC97. World J Gastroenterol 7:630–636
Li Y, Tang ZY, Ye SL, Liu BB, Liu YK, Chen J, Xue Q (2003) Establishment of a hepatocellular carcinoma cell line with unique metastatic characteristics through in vivo selection and screening for metastasis-related genes through cDNA microarray. J Cancer Res Clin Oncol 129:43–51
Liang XH, Loncarevic IF, Tang ZY, Yu YQ, Zentgraf H, Schroder CH (1991) Resection of hepatocellular carcinoma: Oligocentric origin of recurrent and multinodular tumours. J Gastroenterol Hepatol 6:77–80
Liao Y, Tang ZY, Ye SL, Liu KD, Sun FX, Huang Z (2000) Modulation of apoptosis, tumorigenesity and metastatic potential with antisense H-ras oligodeoxynucleotides in a high metastatic tumor model of hepatoma: LCI-D20. Hepatogastroenterology 47:365–370
Liu H, Ye SL, Yang J, Tang ZY, Liu YK, Qin LX, Qiu SJ, Sun RX (2002) The microcell mediated transfer of human chromosome 8 into highly metastatic rat liver cancer cell line C5F. World J Gastroenterol 9:449–453
Liu H, Ye SL, Li WC, LiY, Liu YK, Qin LX, Qiu SJ, Sun RX, Chen J, Tang ZY (2003) Quantitative analysis of expression of TEY1 gene in liver cancer cells with different metastatic potential. Ai Zheng (Chin J Cancer) 22:561–565 (Chin)
Liu YK, Li Y, Ma XM, Chen J, Xue Q, Gao DM, Zhang Y, Ye SL, Tang ZY (2002) Regulation of liver cancer related gene and alpha fetal protein expression by cell differentiation agent II. Zhongguo Zhongliu 11:169–172 (Chin)
Mou DC, Cai SL, Peng JR, Wang Y, Chen HS, Pang XW, Leng XS, Chen WF (2002) Evaluation of MAGE-1 and MAGE-3 as tumour-specific markers to detect blood dissemination of hepatocellular carcinoma cells. Br J Cancer 86:110–116
Muller A, Homey B, Soto H, Ge N, Catron D, Buchanan ME, McClanahan T, Murphy E, Yuan W, Wagner SN, Barrera JL, Mohar A, Verastegui E, Zlotnik A (2001) Involvement of chemokine receptors in breast cancer metastasis. Nature 410:50–56
Muto Y, Moriwaki H, Ninomiya M, Adachi S, Saito A, Takasaki KT, Tanaka T, Tsurumi K, Okuno M, Tomita E, Nakamura T, Kojima T (1996) Prevention of second primary tumors by an acyclic retinoid, polyprenoic acid, in patients with hepatocellular carcinoma. Hepatoma Prevention Study Group. N Engl J Med 334:1561–1567
Muto Y, Moriwaki H, Saito A (1999) Prevention of second primary tumors by an acyclic retinoid in patients with hepatocellular carcinoma. N Engl J Med 340:1046–1047
Niu Q, Tang ZY, Ma ZC, Qin LX, Zhang LH (2000a) Serum vascular endothelial growth factor is a potential biomarker of metastatic recurrence after curative resection of hepatocellular carcinoma. World J Gastroenterol 6:565–568
Niu Q, Tang ZY, Chen L, Ma ZC, Qin LX, Zhang LH (2000b) Basic fibroblast growth factor is a potential predictive marker of metastatic recurrence after resection of hepatocellular carcinoma. Zhonghua Waike Zazhi (Chin J Surg) 38:637–639 (Chin)
Niu Q, Tang ZY, Ma ZC, Qin LX, Bao WH, Zhang LH (2001) Relationship between serum matrix metalloproteinase-2 and metastasis and recurrence following radical hepatic resection in hepatocellular carcinoma. Zhonghua Ganzangbing Zazhi (Chin J Hepatol) 9:56–58 (Chin)
Okochi O, Hibi K, Uemura T, Inoue S, Takeda S, Kaneko T, Nakao A (2002) Detection of mitochondrial DNA alterations in the serum of hepatocellular carcinoma patients. Clin Cancer Res 8:2875–2878
Ono T, Yamanoi A, Nazmy El Assal O, Kohno H, Nagasue N (2001) Adjuvant chemotherapy after resection of hepatocellular carcinoma causes deterioration of long-term prognosis in cirrhotic patients: meta-analysis of three randomized controlled trials. Cancer 91:2378–2385
Pan H-W, Ou Y-H, Peng S-Y, Liu S-H, Lai P-L, Lee P-H, Sheu J-C, Chen C-L, Hsu H-C (2003) Overexpression of osteopontin is associated with intrahepatic metastasis, early recurrence, and poorer prognosis of surgically resected hepatocellular carcinoma. Cancer 98:119–127
Parasole R, Izzo F, Perrone F, Pignata S, Galati MG, Leonardi E, Castiglione F, Orlando R, Castello G, Esposito G, Gallo C, Daniele B (2001) Prognostic value of serum biological markers in patients with hepatocellular carcinoma. Clin Cancer Res 7:3504–3509
Parkin DM, Bray F, Ferlay J, Pisani P (2001) Estimsating the world cancer burden: globocan 2000. Int J Cancer 94:153–156
Poon RT, Ng IO, Lau C, Zhu LX, Yu WC, Lo CM, Fan ST, Wong J (2001a) Serum vascular endothelial growth factor predicts venous invasion in hepatocellular carcinoma: a prospective study. Ann Surg 233:227–235
Poon RT, Ng IO, Lau C, Yu WC, Fan ST, Wong J (2001b) Correlation of serum basic fibroblast growth factor levels with clinicopathologic features and postoperative recurrence in hepatocellular carcinoma. Am J Surg 182:298–304
Qin LX, Tang ZY, Liu KD, Ye SL, Zhou G (1995) p53 mutations may be related to tumor invasiveness of human hepatocellular carcinoma in China. Oncol Rep 2:1175–1179
Qin LX, Tang ZY, Liu KD, Ye SL, He B, Zhang Y, Zhou G (1996) Alterations of CDKN2 (P16/MTS1) exon 2 in human hepatocellular carcinoma. Oncol Rep 3:405–408
Qin LX, Tang ZY, Sham JST, Ma ZC, Ye SL, Zhou XD, Wu ZQ, Trent JM, Guan XY (1999) The association of chromosome 8p deletion and tumor metastasis in human hepatocellular carcinoma. Cancer Res 59:5662–5665
Qin LX, Tang ZY, Ye SL, Liu YK, Ma ZC, Zhou XD, Wu ZQ, Lin ZY, Sun FX, Tian J, Guan X-Y, Pack SD, Zhuang ZP (2001) Chromosome 8p deletion is associate with metastasis of human hepatocellular carcinoma when high and low metastatic models are compared. J Cancer Res Clin Oncol 127:482–488
Qin LX, Tang ZY, Ma ZC, Wu ZQ, Zhou XD, Ye QH, Yuan J, Huang LW, Jia HL, Sun HC, Wang L (2002a) P53 immunohistochemical scoring: an independent prognostic marker for patients after hepatocellular carcinoma resection. World J Gastroenterol 8:459–463
Qin LX, Tang ZY (2002b) The prognostic molecular markers in hepatocellular carcinoma. World J Gastroenterol 8:385–392
Qiu SJ, Ye SL, Wu ZQ, Tang ZY, Liu YK (1998) The expression of the mdm2 gene may be related to the aberration of the p53 gene in human hepatocellular carcinoma. J Cancer Res Clin Oncol 124:253–258
Saffroy R, Lelong JC, Azoulay D, Salvucci M, Reynes M, Bismuth H, Debuire B, Lemoine A (1999) Clinical significance of circulating anti-p53 antibodies in European patients with hepatocellular carcinoma. Br J Cancer 79:604–610
Schwartz JD, Schwartz M, Mandeli J, Sung M (2002) Neoadjuvant and adjuvant therapy for resectable hepatocellular carcinoma: review of the randomised clinical trials. Lancet Oncol 3:593–603
Seki S, Kitada T, Kawada N, Sakaguchi H, Kadoya H, Nakatani K, Satake K, Kuroki T (1999) Establishment and characteristics of human hepatocellular carcinoma cells with metastasis to lymph nodes. Hepatogastroenterology 46:2812–2817
Seow TK, Liang RC, Leow CK, Chung MC (2001) Hepatocellular carcinoma: from bedside to proteomics. Proteomics 1:1249–1263
Shao DM, Wang QH, Chen C, Shen ZH, Yao M, Zhou XD, Tang ZY, Gu JX (1999) N-Actylglucosaminyltransferase V activity in metastatic models of human hepatocellular carcinoma in nude mice. J Exp Clin Cancer Res 18:331–335
Steeg PS (2003) Angiogenesis inhibitors: motivator of metastasis? Nature Med 9:822–823
Sun FX, Tang ZY, Liu KD, Ye SL, Xue Q, Gao DM, Ma ZC (1996) Establishment of a metastatic model of human hepatocellular carcinoma in nude mice via orthotopic implantation of histologically intact tissues. Int J Cancer 66:239–243
Sun HC, Tang ZY, Zhou G, Li XM (1998) Kai-1 gene expression in hepatocellular carcinoma and its relationship with intrahepatic metastases. J Exp Clin Cancer Res 17:307–311
Sun HC, Li XM, Xue Q, Chen J, Gao DM, Tang ZY (1999a) Study of angiogenesis induced by metastatic and non-metastatic liver cancer by corneal micropocket model in nude mice. World J Gastroenterol 5:116–118
Sun HC, Zhang M, Tang ZY, Li XM, Wang L, Gao DM, Xue Q, Chen J (1999b) Inhibition of growth of LCI D20 hepatocellular carcinoma by Endostatin. Zhonghua Shiyan Waike Zazhi (Chin J Exp Surg) 116:491–492 (Chin)
Sun HC, Tang ZY, Li XM, Zhou YN, Sun BR, Ma ZC (1999c) Microvessel density of hepatocellular carcinoma: its relationship with prognosis. J Cancer Res Clin Oncol, 125:419–426
Sun HC, Tang ZY (2003) Preventive treatments for recurrence after curative resection of hepatocellular carcinoma—a literature review of randomized control trials. World J Gastroenterol 9:635–640
Sun JJ, Zhou XD, Liu YK, Tang ZY, Feng JX, Zhou G, Xue Q, Chen J (1999) Invasion and metastasis of liver cancer: expression of intercellular adhesion molecule 1. J Cancer Res Clin Oncol 125:28–34
Sun JJ, Zhou XD, Liu YK, Tang ZY, Sun RX, Zhao Y, Uemura T (2000) Inhibitory effects of syntheticβpeptide on invasion and metastasis of liver cancer. J Cancer Res Clin Oncol 126:595–600
Takayama T, Sekine T, Makuuchi M, Yamasaki S, Kosuge T, Yamamoto J, Shimada K, Sakamoto M, Hirohashi S, Ohashi Y, Kakizoe T (2000) Adoptive immunotherapy to lower postsurgical recurrence rates of hepatocellular carcinoma: a randomised trial. Lancet 356:802–807
Tang ZY (1989) Small hepatocellular carcinoma. In: Tang ZY, Wu MC, Xia SS (eds) Primary liver cancer. Berlin, Springer, pp. 191–203
Tang ZY (2003) Thirty years’ studies on surgery and related basic research of hepatocellular carcinoma. Ann Coll Surg HK 7:11–17
Tang ZY, Ma ZC (1989) Establishment of transplantable human hepatocellular carcinoma in nude mice and their use in studies of tumor markers and radioimmunodetection. In: Tang ZY Wu MC, Xia SS (eds) Primary liver cancer. Berlin, Springer, pp. 172–179
Tang ZY, Yu YQ, Zhou XD (1984) An important approach to prolonging survival further after radical resection of AFP positive hepatocellular carcinoma. J Exp Clin Cancer Res 3:359–366
Tang ZY, Qin LX, Wang XM, Zhou G, Liao Y, Weng Y, Jiang XP, Lin ZY, Liu KD, Ye SL (1998) Alterations of oncogenes, tumor suppressor genes and growth factors in hepatocellular carcinoma: with relation to tumor size and invasiveness. Chin Med J 111:313–318
Tang ZY, Zhou XD, Lin ZY, Yang BH, Ma ZC, Ye SL, Wu ZQ, Fan J, Liu YK, Liu KD, Qin LX, Tian J, Sun HC, He B, Xia JL, Qiu SJ, Zhou J (1999) Surgical treatment of hepatocellular carcinoma and related basic research with special reference to recurrence and metastasis. Chin Med J 112:887–891
Tian J, Tang ZY, Ye SL, Liu YK, Lin ZY, Chen J, Xue Q (1999) New human hepatocellular carcinoma (HCC) cell line with highly metastatic potential (MHCC97) and its expression of the factors associated with metastasis. Br J Cancer 81:814–821
van de Vijver MJ, He YD, van’t Veer LJ, Dai H, Hart AAM, Voskuil DW, Schreiber GJ, Peterse JL, Roberts C, Marton M, Parrish M, Atsma D, Witteveen A, Glas A, Delahaye L, van der Velde T, Bartelink H, Rodenhuis S, Rutgers ET, Friend SH, Bernards AR (2002) A gene-expression signature as a predictor of survival in breast cancer. N Engl J Med 347:1999–2009
Wang G, Zhao Y, Liu X, Wang L, Wu C, Zhang W, Liu W, Zhang P, Cong W, Zhu Y, Zhang L, Chen S, Wan D, Zhao X, Huang W, Gu J (2001) Allelic loss and gain, but not genomic instability, as the major somatic mutation in primary hepatocellular carcinoma. Genes Chromosomes Cancer 31:221–227
Wang L, Tang ZY, Qin LX, Wu XF, Sun HC, Xue Q, Ye SL (2000a) High-dose and long-term therapy with interferon-alfa inhibits tumor growth and recurrence in nude mice bearing human hepatocellular carcinoma xenografts with high metastatic potential. Hepatology 32:43–48
Wang L, Tang ZY, Xue Q, Sun HC, Chen J, Zhang XR, Zhao ZH, Gao DM, Liu YK, Ye SL (2000b) Effect of interferon-α and all-trans retinoic acid on recurrence and metastasis of hepatocellular carcinoma. Zhonghua Shiyan Waike Zazhi (Chin J Exp Surg) 17:421–423 (Chin)
Wang XM, Tang ZY, Xue Q, Hong XY, Bao WH, Zou HQ (1995) Transforming growth factor α induces proliferation and expression of epidermal growth factor receptor in hepatocellular carcinoma cells. J Exp Clin Cancer Res 14:179–184
Witzigmann H, Geissler F, Benedix F, Thiery J, Uhlmann D, Tannapfel A, Wittekind C, Hauss J (2002) Prospective evaluation of circulating hepatocytes by alpha-fetoprotein messenger RNA in patients with hepatocellular carcinoma. Surgery 131:34–43
Wong CM, Lee JM, Lau TC, Fan ST, Ng IO (2002) Clinicopathological significance of loss of heterozygosity on chromosome 13q in hepatocellular carcinoma. Clin Cancer Res 8:2266–2272
Wong IH, Lau WY, Leung T, Yeo W, Johnson PJ (1999) Hematogenous dissemination of hepatocytes and tumor cells after surgical resection of hepatocellular carcinoma: a quantitative analysis. Clin Cancer Res 5:4021–4027
Wu XF, Fan J, Lin ZY, Wu ZQ, Lu JZ, Zhou J, Tang ZY (2003) Quantitative analysis of AFP m RNA in portal, hepatic and peripheral venous blood of patients with HCC during liver surgery and its clinical significance. Zhonghua Gandan Waike Zazhi (Chin J Hepatobiliary Surg) 9:338–341 (Chin)
Xia JL, Yang BH, Tang ZY, Sun FX, Xue Q, Gao DM (1997) Inhibitory effect of the angiogenesis inhibitor TNP-470 on tumor growth and metastasis in nude mice bearing human hepatocellular carcinoma. J Cancer Res Clin Oncol 123:383–387
Xu XR, Huang J, Xu ZG, Qian BZ, Zhu ZD, Yan Q, Cai T, Zhang X, Xiao HS, Qu J, Liu F, Huang QH, Cheng ZH, Li NG, Du JJ, Hu W, Shen KT, Lu G, Fu G, Zhong M, Xu SH, Gu WY, Huang W, Zhao XT, Hu GX, Gu JR, Chen Z, Han ZG (2001) Insight into hepatocellular carcinogenesis at transcriptome level by comparing gene expression profiles of hepatocellular carcinoma with those of corresponding noncancerous liver. Proc Natl Acad Sci USA 98:15089–15094
Yang J, Qin LX, Ye SL, Liu YK, Li Y, Gao DM, Chen J, Tang ZY (2003) The abnormalities of chromosome 8 in two hepatocellular carcinoma cell lines with the same genetic background and different metastatic potential. J Cancer Res Clin Oncol 129:303–308
Yao M, Zhou XD, Zha XL, Shi DR, Fu J, He JY, Lu HF, Tang ZY (1997) Expression of the integrin α5 subunit and its mediated cell adhesion in hepatocellular carcinoma. J Cancer Res Clin Oncol 123:435–440
Yao M, Zhou DP, Jiang SM, Wang QH, Zhou XD, Tang ZY, Gu JX (1998a) Elevated activity of N-acetylglucosaminyltransferase V in human hepatocellular carcinoma. J Cancer Res Clin Oncol 124:27–30
Yao M, Zhou XD, Liu YK, Tang ZY (1998b) Expression of E-cadherin in hepatocellular carcinoma with high invasiveness. Zhonghua Xiaohua Zazhi (Chin J Digest) 18:31–33 (Chin)
Ye QH, Qin LX, Forgues M, He P, Kim JW, Peng AC, Simon R, Li Y, Robles AI, Chen YD, Ma ZC, Wu ZQ, Ye SL, Liu YK, Tang ZY, Wang XW (2003) Predicting hepatitis B virus-positive metastatic hepatocellular carcinomas using gene expression profiling and supervised machine learning. Nature Med 9:416–423
Ye YJ, Yu YQ, Tang ZY, Wan DF, Lu JZ, He LP (1998) Construction of nm23-H1 cDNA clone and the relationship between its mRNA expression and metastasis in hepatocellular carcinoma. Zhonghua Shiyan Waike Zazhi (Chin J Exp Surg) 15:17–18 (Chin)
Zhang LH, Qin LX, Ma ZC, Ye SL, Liu YK, Ye QH, Wu X, Huang W, Tang ZY (2003) Allelic imbalance regions on chromosomes 8p, 17p and 19p related to metastasis of hepatocellular carcinoma: comparison between matched primary and metastatic lesions in 22 patients by genomic microsatellite analysis. J Cancer Res Clin Oncol 129:279–286
Zhao X, Li J, He Y, Lan F, Fu L, Guo J, Zhao R, Ye Y, He M, Chong W, Chen J, Zhang L, Yang N, Xu B, Wu M, Wan D, Gu J (2001) A novel growth suppressor gene on chromosome 17p13.3 with a high frequency of mutation in human hepatocellular carcinoma. Cancer Res 61:7383–7387
Zhao X, He M, Wan D, Ye Y, He Y, Han L, Guo M, Huang Y, Qin W, Wang MW, Chong W, Chen J, Zhang L, Yang N, Xu B, Wu M, Zuo L, Gu J (2003) The minimum LOH region defined on chromosome 17p13.3 in human hepatocellular carcinoma with gene content analysis. Cancer Lett 190:221–232
Zheng Q, Tang ZY, Xue Q (1998a) Changes of PAI-1 and biological behaviour of human hepatocellular carcinoma in metastatic model of nude mice. Zhonghua Waike Zazhi (Chin J Surg) 36:687–689 (Chin)
Zheng Q, Tang ZY, Xue Q (1998b) Role of heparin on tumor growth and metastasis in model of human hepatocellular carcinoma in nude mice. Zhonghua Ganzangbing Zazhi (Chin J Hepatol) 6:151–152 (Chin)
Zheng Q, Tang ZY, Wu ZQ (1999) Changes of PAI-1 in plasma and tumor extract of patients with hepatocellular carcinoma. Zhonghua Xiaohua Zazhi (Chin J Digest) 19:16–18 (Chin)
Zheng Q, Tang ZY, Xue Q, Shi DR, Song HY, Tang HB (2000) Invasion and metastasis of hepatocellular carcinoma in relation to urokinase-type plasminogen activator, its receptor and inhibitor. J Cancer Res Clin Oncol 126:641–646
Zheng XY, Lin ZY, Tang ZY, Liu YK, Feng XL, Zhuang W (1998) The abundance of NM23-H1 mRNA is related with in situ microenvironment and intrahepatic metastasis in hepatocellular carcinoma. J Exp Clin Cancer Res 17:337–341
Zhou J, Tang ZY, Fan J, Wu ZQ, Li XM, Liu YK, Liu F, Sun HC, Ye SL (2000a) Expression of platelet-derived endothelial cell growth factor and vascular endothelial growth factor in hepatocellular carcinoma and portal vein tumor thrombus. J Cancer Res Clin Oncol 126:57–61
Zhou J, Tang ZY, Fan J, Wu ZQ, Ji Y, Wang L, Bao WH, Qiu SJ (2000b) Study on inhibition of the growth and metastasis of LCID20 hepatocellular carcinoma by capecitabine. Zhonghua Shiyan Waike Zazhi (Chin J Exp Surg) 17:403–405 (Chin)
Zhou J, Tang ZY, Fan J, Wu ZQ, Ji Y, Ye SL (2001) The potential of plasma thrombomodulin as a biomarker of portal vein tumor thrombus in hepatocellular carcinoma. J Cancer Res Clin Oncol 127:559–564
Acknowledgments
We thank Fan-Xian Sun, Jian Tian, Qiong Xue, and Jie Chen for the establishment of metastatic models; Qi Zheng, Xiao-Ming Li, Qi Niu, and Xiao-Feng Wu for studies of metastatic predictors; Ming Yao and Lian-Hai Zhang for studies on metastasis-related genes and chromosomes; Yong Liao and Jing-Jing Sun for experimental interventions. These studies were supported in part by the State Key Basic Research Program of China (G1998051211), Key Laboratory of Carcinogenesis and Cancer Invasion (Fudan University), Ministry of Education, and the Fund for Leading Specialty of Shanghai Metropolitan Bureau of Health 983001.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Tang, ZY., Ye, SL., Liu, YK. et al. A decade’s studies on metastasis of hepatocellular carcinoma. J Cancer Res Clin Oncol 130, 187–196 (2004). https://doi.org/10.1007/s00432-003-0511-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00432-003-0511-1