
Abstract
Although traditionally considered sterile, human milk is currently recognized as an alive ecosystem that harbors not only bacteria, but also viruses, fungi and yeasts, and minor genera, collectively known as the human milk microbiome (HMM). The seeding of HMM is a complex phenomenon whose dynamics are still a matter of research. Many factors contribute to its determination, both maternal, neonatal, environmental, and related to human milk itself. The transmission of microorganisms to the infant through breastfeeding may impact its present and future health, mainly shaping the GI tract microbiome and immune system. The existence and persistence of HMM as a conserved feature among different species may also have an evolutionary meaning, which will become apparent only in evolutionary times.
Conclusion: The complexities of HMM warrant further research in order to deepen our knowledge on its origin, determinants, and impact on infants’ health. The practical and translational implications of research on HMM (e.g., reconstitution of donor human milk through inoculation of infant’s own mother milk, modulation of HMM through maternal dietary supplementation) should not be overlooked.
What is Known: • Human milk harbors a wide variety of microorganisms, ranging from bacteria to viruses, fungi and yeasts, and minor genera. • Human milk microbiome is shaped over time by many factors: maternal, neonatal, environmental, and related to human milk itself. • The transmission of microorganisms through breastfeeding may impact the infant’s present and future health. | |
What is New: • We provide an overview on human milk microbiome, hopefully encouraging physicians to consider it among the other better-known breastfeeding benefits. • Further studies, with standardized and rigorous study designs to enhance accuracy and reproducibility of the results, are needed to deepen our knowledge of the human milk microbiota and its role in newborn and infant’s health. |
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Human milk (HM) was traditionally thought to be sterile. However, the presence of bacteria in HM was never fully excluded. The first studies conducted between the end of the 19th and the beginning of the 20th century [1,2,3] focused on the potentially harmful nature of the bacteriological content of HM, failing to consider it, as it now is, as a precious resource. Still, in the late 60s, the presence of bacteria in HM was considered a consequence of low levels of personal and environmental hygiene [4].
Later on, in 2003, interest in the microbiology of HM resurfaced with a new perspective. Based on the detection of allegedly endogenous lactic acid bacteria from HM of eight healthy mothers, it was suggested that HM could be considered a symbiotic food, harboring safe bacteria with a potential role in the prevention of neonatal infectious diseases [5].
Over time, the development of culture-independent techniques (e.g., quantitative polymerase chain reaction and next-generation sequencing—NGS), in addition to the already well established culture-dependent ones, has progressively allowed for the characterization of the composition, diversity, and variability of HM microflora in greater detail, albeit with some limitations [6].
Today, HM is considered “mother nature’s prototypical probiotic food” [7]. Growing research on this subject has led to a deeper understanding of the matter, discovering that HM is an alive universe populated by bacteria, viruses, fungi and yeasts that cooperate for the present and future health of the infant. This complex host-associated microbial community constitutes the HM microbiome (HMM).
The aim of this review is to provide an overview of what is currently known on HMM origin, composition, determinants, and role, eventually suggesting possible future directions for researchers who want to further explore this field.
Origin of HMM
The seeding of HMM is a complex and dynamic process, still not completely understood to date. Multiple, non-mutually exclusive, sources of HMM have been suggested (Table 1). It is still up for debate whether the mammary gland hosts a resident microbiome (i.e., the mucosal interface model) or it is simply a bystander subjected to a constant influx of microbes from exogenous sources (i.e., the constant influx model). This latter model is supported by the current lack of evidence of bacterial adhesion to the mammary epithelium outside of a mastitis setting, and of bacterial reproduction within the mammary tissue. Conversely, the mucosal interface model is supported by evidence of a pre-lactation mammary gland microbiome [8]. However, the fact that nonlactating mammary gland microbiome differs from HMM does not allow to exclude the constant influx model [9].
Composition
Although historically the knowledge of HMM was only limited to bacterial species [15], recent evidence highlighted that HM contains a wide variety of microorganisms, including viruses, fungi and yeasts, and new genera (Table 2).
Bacteriome
The implementation of the new NGS techniques, such as metataxonomics (16SrRNA gene sequencing) and metagenomics (shot-gun sequencing), has allowed for the detection of several new bacterial species, including many anaerobes, adding up to a total of more than 1300 different species [12, 16, 17, 22,23,24,25,26,27].
However, when trying to determine what constitutes the HM bacteriome, inter-individual variability, and geographic location of the study, methods used for HM collection, storage, and analysis must be taken into consideration. Hence, the definition, and the existence itself, of a “core” HM bacteriome is still a matter of debate [28].
Using genomic analysis, different studies have detected a wide variety of soil and water-related microorganisms, such as Bradyrhizobium, Pseudomonas, and Stenotrophomonas [8, 12, 16, 22, 26, 29]. However, these results must be critically interpreted, as such microorganisms could also be contained in molecular biology reagents, solutions, and kits, and their relative amounts could be amplified by DNA techniques, thus contributing to mistaken interpretations [22, 30,31,32]. Furthermore, differentiating between live or dead microorganisms is critical. Therefore, appropriate techniques should be selected to limit possible biases [33].
Virome
Most (95%, [18]) of the HM virome is made of bacteriophages, with eukaryotic viruses and other viral particles constituting a lesser proportion.
HM virome has distinctive features that differentiate it from other viromes (e.g., adult stool, urine, saliva, and cerebrospinal fluid viromes) [34, 35]. Conversely, a significant number of shared viruses have been identified between HM and infant stool from mother-infant pairs, supporting their vertical inheritance through breastfeeding [34, 36]. Interestingly, it has been noted [34] that the virome of infant stool bears a closer resemblance to HM than to adult stool.
Mycobiome and other -omes
Fungi are an important component of the human microbiome [37]. However, their presence in HM is a relatively recent discovery [20]. Although considering geographical variability, the existence of a core mycobiome has been hypothesized, thus suggesting that their transmission through HM is a conserved feature.
Other microorganisms, until recently neglected, contribute to the HMM. In particular, current research has been focusing on Archaea. The presence of archaeal DNA has been demonstrated in 8/10 HM samples analyzed, none of which belonging to women with mastitis, thus suggesting a protective role [17]. Conversely, other authors did not identify archaeal DNA in the HM samples analyzed [38].
Determinants Of HMM
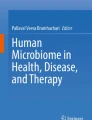
The complex HM ecosystem appears to be shaped over time by many factors: maternal, neonatal, environmental, and related to HM itself (Fig. 1). The extremely dynamic nature of HMM composition may account for the often-contradictory data reported in the Literature. Furthermore, it should be noted that many factors that have been implicated in the determination of HMM are closely intertwined.

Overview of the main determinants of HMM (see text for explanation)
Maternal determinants
Some authors [26, 39,40,41] demonstrated that, compared to women who underwent a C-section, vaginally delivered women’s HM samples showed higher bacterial diversity and richness, with higher levels of Bifidobacterium and Lactobacillus spp. However, other studies did not confirm such results [42, 43]. A potential influence of the mode of delivery on the virome and mycobiome of HM has been hypothesized as well [44, 45].
A decrease in the abundance of Lactobacillus, Bifidobacterium, Staphylococcus, and Eubacterium spp. in HM samples from mothers who received peri-natal antibiotics has been reported [8, 46, 47]. Maternal chemotherapy during lactation has also been associated with a reduction in HM bacterial diversity [48].
Maternal diet impacts HMM composition (allegedly more so during pregnancy than during lactation [49,50,51]). High-fiber and high-fat food dietary regimens [49] as well as vitamin intake (vitamin C and complex B vitamins) [51] have been shown to alter HMM composition. Furthermore, both pre-pregnancy BMI and weight gain during gestation are reflected in differential abundances of bacterial strains (mainly Streptococcus, Staphylococcus, and Bifidobacterium) in HM [40, 52,53,54].
Compared to healthy women, mothers with celiac disease have lower levels of Bacteroides spp. and Bifidobacterium spp. in their milk [55]. Likewise, mastitis determines modifications in bacterial load and microbial diversity in HMM, which subside once clinical symptoms disappear [56,57,58].
Maternal post-natal psychosocial distress (defined as symptoms of anxiety, stress, or depression during the postnatal period) has been linked to lower HM bacterial diversity at 3 months post-delivery, with a progressive decrease in the relative abundance of Staphylococci and a parallel increase of some minority genera (Lactobacillus, Acinetobacter, and Flavobacterium) in mothers with low psychosocial distress [59].
Neonatal determinants
Lower counts of Enterococcus spp. and higher counts of Bifidobacterium spp. have been detected in HM samples from mothers who delivered at term compared to preterm mothers [39]. Conversely, other authors [42] did not detect any difference in microbial profiles based on length of gestation, postulating a fail-safe mechanism that allows the mother to be “ready” to pass along her bacterial imprint regardless of gestational age at birth, as part of an evolutionary pressure directed towards the baby’s benefit. Variations in HM virome and mycobiome composition according to gestational age and birth weight have been recently demonstrated [44, 45].
Effect of newborn gender on HMM composition has been hypothesized [60], based on the detection of more Streptococci and less Staphylococci in HM from mothers of male infants compared to mothers of female infants. However, such differences have not been confirmed by other studies [42, 61].
Environmental determinants
The analysis of HM samples collected from selected populations in Europe, Africa, and Asia, suggested that HMM composition is related to the geographical study location [62]. Furthermore, a high variability in HM metabolites across study sites, and an association between variations in HM metabolome and specific features of HMM, have been documented [63]. However, a novel analysis of HM samples from Ethiopia, The Gambia, Ghana, Kenya, the USA, Peru, Spain, and Sweden, demonstrated that, while HM bacterial communities varied geographically, they consistently contained the core genera Staphylococcus and Streptococcus [64]. Such results have been confirmed by a recent systematic review [65], which included twelve studies that used culture-independent methods to identify bacteria at genus level in HM from healthy women. Notably, it has been speculated that at least part of the geographical variability in HMM composition might be related to differences in the setting and procedure of HM collection, storage, and analysis [66]. As for collection methods, it has been observed [61] that HM from mothers who use breast pumps have higher microbial load and lower abundance of cultivable staphylococci compared to HM samples collected manually. Conversely, other authors found no difference in ɑ-diversity between samples collected by manual expression or by pumping with a single-use sterile device [67].
The analysis of HMM from women living in the same Indian region but with different lifestyles (traditional vs. western-like), revealed that HM samples from “rural women” had higher diversity and greater abundance of sub-dominant bacterial lineages than those from “urban women” [68].
A study conducted in the Central Africa Republic within a small-scale society suggested that seasonality may influence the relative abundance of specific taxa in HMM, although it may be difficult to determine whether the variation in composition depends on differences in seasonal environmental exposure and/or seasonal variation in diet [69]. The same study [69] explored the relationship between mother-infant social network size, and HMM composition and diversity, showing how HM from mothers with larger networks, and infants with more caregivers, had higher microbial evenness (but not microbial richness) than HM from mothers whose infants had fewer caregivers.
HM determinants
Cabrera-Rubio et al. [26] were the first to describe the changes HMM undergoes over time, from colostrum to transitional and mature milk. These authors reported a progressively increased abundance of typical oral inhabitants (e.g., Veillonella, Leptotrichia, and Prevotella spp.) in transition and mature HM, and higher counts of Bifidobacterium at later stages of lactation. Other authors [39] later reported a greater influence of lactation stage on Bifidobacterium and Enterococcus spp. counts, which showed a progressive increase in their concentration from colostrum to mature HM, as did Lactobacillus and Staphylococcus spp. Different patterns over time have been described. Analyzing HM samples collected at 3 time points over a 4-week interval, a set of 9 “core operational taxonomic units” was identified [16]. However, in some samples, HM bacterial communities were rather consistent over time, whereas, in others, the relative abundance of the bacterial genera shifted over time [16]. Some authors [60] observed a relative stability of HMM over time, with only small changes in some minority genera, while others [43] did not observe any effect of lactation stage on HMM composition. Regarding the virome, it was recently documented [44] that, although bacteriophages are predominant in both transient and mature HM samples, transient HM has a greater abundance of Podoviridae and Myoviridae, whereas in mature HM Podoviridae decreases, and Siphoviridae becomes the most abundant family. As for mycobiome, a recent study [45] analyzed samples of HM from different stages of lactation and found that, in transient HM samples, Saccharomyces cerevisiae and Aspergillus glaucus were the most abundant species, while Penicillium rubens and Aspergillus glaucus were predominant in mature HM samples.
It has been speculated that other HM components, such as HM oligosaccharides (HMOs—prebiotics), milk fatty acids, hormones, immune cells, and antibodies, could modulate the composition of HMM [70, 71]. In particular, HMOs may promote the growth of Staphylococcus spp. in the lactating mammary gland [72].
Donor human milk and HMM
When mother’s own milk is not available or insufficient, donor HM (DHM) is the second-best alternative [73,74,75]. However, pasteurization, needed to guarantee the necessary microbiological safety standards, inevitably inactivates several of HM nutritional and biological properties [76], including HMM. As a matter of fact, pasteurization eliminates most milk bacteria (except the spore-forming Bacillus species [77,78,79]). Nevertheless, viability of HMM is no longer considered essential. Indeed, the probiotic effect of beneficial microbes in HM has been hypothesized to rely on the ability of the host’s cells to recognize specific bacterial components or products, thus activating the immune system. These “non-viable (more often heat-inactivated) microbial cells (intact or broken) or crude cell extracts (i.e., nucleic acids, cell-wall components)” are known as para-probiotics or ghost probiotics [80].
Role and benefits of HMM
HMM seeds the infant GI tract with pioneering bacteria, thus contributing to the establishment of both the infant oral and gut microbiota [81, 82]. However, not all the bacteria present in HM are found in the infant gut, but, rather, only a select few seem to colonize the newborn [42]. Nonetheless, it has been hypothesized that transient exposure could be just as effective as persistent colonization [83, 84]. Moreover, bacteria in HM may upregulate protective factors such as antibodies, immune cells, lactoferrin, and beta-defensins that would then be passed on to the neonate through breastfeeding [42]. The HM virome, especially bacteriophages, likely contributes to the gut ecology of the infant, as well [18].
Early microbial exposure is essential to provide antigenic stimuli that promote the intestinal immune system maturation by encouraging a shift from the predominant intrauterine T helper (TH) 2 cell immune milieu to a TH1/TH2 balanced response, and triggering regulatory T cell differentiation [85].
Through modifications of the infant gut microbiota and by means of the gut-brain axis, HMM may also influence the development of a more convenient behavioral phenotype of the offspring, as hypothesized for other HM bioactives [86]. Indeed, in early infancy, HM may promote the colonization of a specific microbiota that influences offspring biobehavioral regulation. A milk-oriented infant gut microbiota may produce a less energetically costly behavioral phenotype in order to more optimally allocate maternal energetic investment [86].
An association between breastfeeding and upper respiratory microbiota composition at 6 weeks was reported, with breastfed infants showing a significantly different microbial composition than formula-fed ones [87]. Interestingly, such association seems to disappear at 6 months of age (when weaning typically begins) [87, 88].
Finally, it has been hypothesized that HMM may benefit the mother too, protecting her against infections such as mastitis [42].
Potential evolutionary significance of HMM
Breastfeeding represents a valuable route of maternal microbial transmission both in humans and other animals (i.e., rhesus monkeys, cows, sheep, goats) [89,90,91,92]. Since the transmission of HMM appears to be a conserved feature among different species, a possible evolutionary purpose can be hypothesized.
Maternal microbial transmission provides offspring with important microbes early in life, rather than leaving their acquisition to chance during later stages of development. By shaping the offspring’s own microbiome, such microbes may determine evolutionary advantages in the recipient [11, 93, 94]. Consequently, within a broader evolutionary context, HMM transmission could be seen as at least partially capable of shaping the microbiome of the whole species over evolutionary time, since microbes that promote host fitness will increase their odds of reaching the next generation.
Future directions
Despite the progress made in the last decades, many unanswered questions still remain. However, the lack of internationally recognized “best practices” in HMM analysis (e.g., HM collection, storage, processing, DNA extraction, and sequencing) often limits comparison among studies. Therefore, standardized and rigorous study designs are needed to promote accuracy and reproducibility of the results.
Many topics addressed in the present review represent interesting fields to explore. Firstly, the sources and pathways of HMM seeding should be further examined, possibly through experimental studies on animal models. Moreover, interactions between mother, infant, and environment should be better investigated, thus uncovering hidden mechanisms of coregulation between different microbiomes. Additionally, all the members of the microbial community of HM should be equally considered. So far, bacteria have been the most studied microorganisms. Progressively, attention has shifted to viruses (although with a strong bias towards DNA viruses), fungi, and yeasts. The next frontier will be to explore the archaeome and to deepen our knowledge of the potential infant health implications of the “minor” components of HMM. Finally, the functional significance of HMM and its impact on infants’ GI tract microbiome, immune system, and later health would benefit from appropriate experimental, possibly longitudinal, studies.
The practical and translational implications of research on HMM should also be considered. For example, studies on the reconstitution of DHM through inoculation of definite amounts of infant’s own mother milk aimed at restoring the live HMM, as described by Cacho et al. [95], should be incentivized. Likewise, the possible role of maternal dietary supplementation with pre- or postbiotics aimed at modulating HMM should be clarified, as well as the more suitable timing for such supplementation (e.g., during pregnancy and/or during lactation).
Conclusions
Although traditionally considered sterile, it is now clear that HM harbors a wide variety of microorganisms, ranging from bacteria to viruses, fungi and yeasts, and minor genera. The transmission of such microorganisms to the infant may help determine its present and future health, mainly shaping the neonatal GI tract microbiome and immune system. The complexities of the HM ecosystem warrant further research to deepen our knowledge on HMM origin, determinants, and implications for infants’ health.
Abbreviations
- BMI:
-
Body mass index
- DHM:
-
Donor human milk
- GI:
-
Gastro-intestinal
- HM:
-
Human milk
- HMM:
-
Human milk microbiome
- HMOs:
-
Human milk oligosaccharides
- NGS:
-
Next-generation sequencing
References
Ringel UD, Keimgehalt D (1893) Frauenmilch. Münchener med. Wochenschrift. Nr. 27. Ref. Centralblatt, für Bakteriologie. Bd. XIV. S. 429
Holt EL, Howland J (1922) The diseases of infancy and childhood
Dudgeon LS, Jewesbury RC (1924) The bacteriology of human milk. J Hyg (Lond) 23:64–76. https://doi.org/10.1017/s0022172400008470
Wyatt RG (1967) Mata LJ (1969) Bacteria in colostrum and milk of Guatemalan Indian women. J Trop Pediatr 15:159–162. https://doi.org/10.1093/tropej/15.4.159
Martín R, Langa S, Reviriego C et al (2003) Human milk is a source of lactic acid bacteria for the infant gut. J Pediatr 143:754–758. https://doi.org/10.1016/j.jpeds.2003.09.028
LeMay-Nedjelski L, Copeland J, Wang PW et al (2018) Methods and strategies to examine the human breastmilk microbiome. Methods Mol Biol 1849:63–86. https://doi.org/10.1007/978-1-4939-8728-3_5
McGuire MK, McGuire MA (2015) Human milk: mother nature’s prototypical probiotic food? Adv Nutr 6:112–123. https://doi.org/10.3945/an.114.007435
Urbaniak C, Cummins J, Brackstone M et al (2014) Microbiota of human breast tissue. Appl Environ Microbiol 80:3007–3014. https://doi.org/10.1128/AEM.00242-14
Stinson LF, Sindi ASM, Cheema AS et al (2021) The human milk microbiome: who, what, when, where, why, and how? Nutr Rev 79:529–543. https://doi.org/10.1093/nutrit/nuaa029
Biagi E, Aceti A, Quercia S et al (2018) Microbial community dynamics in mother’s milk and infant’s mouth and gut in moderately preterm infants. Front Microbiol 9:2512. https://doi.org/10.3389/fmicb.2018.02512
Fernández L, Langa S, Martín V et al (2013) The human milk microbiota: origin and potential roles in health and disease. Pharmacol Res 69:1–10. https://doi.org/10.1016/j.phrs.2012.09.001
Jost T, Lacroix C, Braegger CP et al (2014) Vertical mother-neonate transfer of maternal gut bacteria via breastfeeding. Environ Microbiol 16:2891–2904. https://doi.org/10.1111/1462-2920.12238
Boix-Amorós A, Collado MC, Mira A (2016) Relationship between milk microbiota, bacterial load, macronutrients, and human cells during lactation. Front Microbiol 7:492. https://doi.org/10.3389/fmicb.2016.00492
Rodríguez JM (2014) The origin of human milk bacteria: is there a bacterial entero-mammary pathway during late pregnancy and lactation? Adv Nutr 5:779–784. https://doi.org/10.3945/an.114.007229
Eidelman AI, Szilagyi G (1979) Patterns of bacterial colonization of human milk. Obstet Gynecol 53:550–552
Hunt KM, Foster JA, Forney LJ et al (2011) Characterization of the diversity and temporal stability of bacterial communities in human milk. PLoS One 6:e21313. https://doi.org/10.1371/journal.pone.0021313
Jiménez E, de Andrés J, Manrique M et al (2015) Metagenomic analysis of milk of healthy and mastitis-suffering women. J Hum Lact 31:406–415. https://doi.org/10.1177/0890334415585078
Mohandas S, Pannaraj PS (2020) Beyond the bacterial microbiome: virome of human milk and effects on the developing infant. Nestle Nutr Inst Workshop Ser 94:86–93. https://doi.org/10.1159/000504997
Boix-Amorós A, Puente-Sánchez F, du Toit E et al (2019) Mycobiome profiles in breast milk from healthy women depend on mode of delivery, geographic location, and interaction with bacteria. Appl Environ Microbiol 85:e02994-e3018. https://doi.org/10.1128/AEM.02994-18
Boix-Amorós A, Martinez-Costa C, Querol A et al (2017) Multiple approaches detect the presence of fungi in human breastmilk samples from healthy mothers. Sci Rep 7:13016. https://doi.org/10.1038/s41598-017-13270-x
Togo AH, Grine G, Khelaifia S et al (2019) Culture of methanogenic archaea from human colostrum and milk. Sci Rep 9:18653. https://doi.org/10.1038/s41598-019-54759-x
Fernández L, Pannaraj PS, Rautava S, Rodríguez JM (2020) The microbiota of the human mammary ecosystem. Front Cell Infect Microbiol 10:586667. https://doi.org/10.3389/fcimb.2020.586667
Fouhy F, Ross RP, Fitzgerald GF et al (2012) Composition of the early intestinal microbiota: knowledge, knowledge gaps and the use of high-throughput sequencing to address these gaps. Gut Microbes 3:203–220. https://doi.org/10.4161/gmic.20169
Togo A, Dufour J-C, Lagier J-C et al (2019) Repertoire of human breast and milk microbiota: a systematic review. Future Microbiol 14:623–641. https://doi.org/10.2217/fmb-2018-0317
Jost T, Lacroix C, Braegger C, Chassard C (2013) Assessment of bacterial diversity in breast milk using culture-dependent and culture-independent approaches. Br J Nutr 110:1253–1262. https://doi.org/10.1017/S0007114513000597
Cabrera-Rubio R, Collado MC, Laitinen K et al (2012) The human milk microbiome changes over lactation and is shaped by maternal weight and mode of delivery. Am J Clin Nutr 96:544–551. https://doi.org/10.3945/ajcn.112.037382
Zimmermann P, Curtis N (2020) Breast milk microbiota: a review of the factors that influence composition. J Infect 81:17–47. https://doi.org/10.1016/j.jinf.2020.01.023
Ojo-Okunola A, Nicol M, du Toit E (2018) Human breast milk bacteriome in health and disease. Nutrients 10:E1643. https://doi.org/10.3390/nu10111643
Li S-W, Watanabe K, Hsu C-C et al (2017) Bacterial composition and diversity in breast milk samples from mothers living in Taiwan and Mainland China. Front Microbiol 8:965. https://doi.org/10.3389/fmicb.2017.00965
Mühl H, Kochem A-J, Disqué C, Sakka SG (2010) Activity and DNA contamination of commercial polymerase chain reaction reagents for the universal 16S rDNA real-time polymerase chain reaction detection of bacterial pathogens in blood. Diagn Microbiol Infect Dis 66:41–49. https://doi.org/10.1016/j.diagmicrobio.2008.07.011
Salter SJ, Cox MJ, Turek EM et al (2014) Reagent and laboratory contamination can critically impact sequence-based microbiome analyses. BMC Biol 12:87. https://doi.org/10.1186/s12915-014-0087-z
Laurence M, Hatzis C, Brash DE (2014) Common contaminants in next-generation sequencing that hinder discovery of low-abundance microbes. PLoS One 9:e97876. https://doi.org/10.1371/journal.pone.0097876
Emerson JB, Adams RI, Román CMB et al (2017) Schrödinger’s microbes: tools for distinguishing the living from the dead in microbial ecosystems. Microbiome 5:86. https://doi.org/10.1186/s40168-017-0285-3
Pannaraj PS, Ly M, Cerini C et al (2018) Shared and distinct features of human milk and infant stool viromes. Front Microbiol 9:1162. https://doi.org/10.3389/fmicb.2018.01162
Ghose C, Ly M, Schwanemann LK et al (2019) The virome of cerebrospinal fluid: viruses where we once thought there were none. Front Microbiol 10:2061. https://doi.org/10.3389/fmicb.2019.02061
Duranti S, Lugli GA, Mancabelli L et al (2017) Maternal inheritance of bifidobacterial communities and bifidophages in infants through vertical transmission. Microbiome 5:66. https://doi.org/10.1186/s40168-017-0282-6
Cui L, Morris A, Ghedin E (2013) The human mycobiome in health and disease. Genome Med 5:63. https://doi.org/10.1186/gm467
Asnicar F, Manara S, Zolfo M et al (2017) Studying vertical microbiome transmission from mothers to infants by strain-level metagenomic profiling. mSystems 2:e00164–16. https://doi.org/10.1128/mSystems.00164-16
Khodayar-Pardo P, Mira-Pascual L, Collado MC, Martínez-Costa C (2014) Impact of lactation stage, gestational age and mode of delivery on breast milk microbiota. J Perinatol 34:599–605. https://doi.org/10.1038/jp.2014.47
Cabrera-Rubio R, Mira-Pascual L, Mira A, Collado MC (2016) Impact of mode of delivery on the milk microbiota composition of healthy women. J Dev Orig Health Dis 7:54–60. https://doi.org/10.1017/S2040174415001397
Hoashi M, Meche L, Mahal LK et al (2016) Human milk bacterial and glycosylation patterns differ by delivery mode. Reprod Sci 23:902–907. https://doi.org/10.1177/1933719115623645
Urbaniak C, Angelini M, Gloor GB, Reid G (2016) Human milk microbiota profiles in relation to birthing method, gestation and infant gender. Microbiome 4:1. https://doi.org/10.1186/s40168-015-0145-y
Sakwinska O, Moine D, Delley M et al (2016) Microbiota in breast milk of Chinese lactating mothers. PLoS One 11:e0160856. https://doi.org/10.1371/journal.pone.0160856
Dinleyici M, Pérez-Brocal V, Arslanoglu S et al (2021) Human milk virome analysis: changing pattern regarding mode of delivery, birth weight, and lactational stage. Nutrients 13:1779. https://doi.org/10.3390/nu13061779
Dinleyici M, Pérez-Brocal V, Arslanoglu S et al (2020) Human milk mycobiota composition: relationship with gestational age, delivery mode, and birth weight. Benef Microbes 11:151–162. https://doi.org/10.3920/BM2019.0158
Soto A, Martín V, Jiménez E et al (2014) Lactobacilli and bifidobacteria in human breast milk: influence of antibiotherapy and other host and clinical factors. J Pediatr Gastroenterol Nutr 59:78–88. https://doi.org/10.1097/MPG.0000000000000347
Witt A, Mason MJ, Burgess K et al (2014) A case control study of bacterial species and colony count in milk of breastfeeding women with chronic pain. Breastfeed Med 9:29–34. https://doi.org/10.1089/bfm.2013.0012
Urbaniak C, McMillan A, Angelini M et al (2014) Effect of chemotherapy on the microbiota and metabolome of human milk, a case report. Microbiome 2:24. https://doi.org/10.1186/2049-2618-2-24
LeMay-Nedjelski L, Asbury MR, Butcher J et al (2021) Maternal diet and infant feeding practices are associated with variation in the human milk microbiota at 3 months postpartum in a cohort of women with high rates of gestational glucose intolerance. J Nutr 151:320–329. https://doi.org/10.1093/jn/nxaa248
Cortes-Macías E, Selma-Royo M, García-Mantrana I et al (2021) Maternal diet shapes the breast milk microbiota composition and diversity: impact of mode of delivery and antibiotic exposure. J Nutr 151:330–340. https://doi.org/10.1093/jn/nxaa310
Padilha M, Danneskiold-Samsøe NB, Brejnrod A et al (2019) The human milk microbiota is modulated by maternal diet. Microorganisms 7:E502. https://doi.org/10.3390/microorganisms7110502
Lundgren SN, Madan JC, Karagas MR et al (2019) Microbial communities in human milk relate to measures of maternal weight. Front Microbiol 10:2886. https://doi.org/10.3389/fmicb.2019.02886
Davé V, Street K, Francis S et al (2016) Bacterial microbiome of breast milk and child saliva from low-income Mexican-American women and children. Pediatr Res 79:846–854. https://doi.org/10.1038/pr.2016.9
Collado MC, Laitinen K, Salminen S, Isolauri E (2012) Maternal weight and excessive weight gain during pregnancy modify the immunomodulatory potential of breast milk. Pediatr Res 72:77–85. https://doi.org/10.1038/pr.2012.42
Olivares M, Albrecht S, De Palma G et al (2015) Human milk composition differs in healthy mothers and mothers with celiac disease. Eur J Nutr 54:119–128. https://doi.org/10.1007/s00394-014-0692-1
Boix-Amorós A, Hernández-Aguilar MT, Artacho A et al (2020) Human milk microbiota in sub-acute lactational mastitis induces inflammation and undergoes changes in composition, diversity and load. Sci Rep 10:1–14. https://doi.org/10.1038/s41598-020-74719-0
Mediano P, Fernández L, Jiménez E et al (2017) Microbial diversity in milk of women with mastitis: potential role of coagulase-negative Staphylococci, Viridans group Streptococci, and Corynebacteria. J Hum Lact 33:309–318. https://doi.org/10.1177/0890334417692968
Patel SH, Vaidya YH, Patel RJ et al (2017) Culture independent assessment of human milk microbial community in lactational mastitis. Sci Rep 7:7804. https://doi.org/10.1038/s41598-017-08451-7
Browne PD, Aparicio M, Alba C et al (2019) Human milk microbiome and maternal postnatal psychosocial distress. Front Microbiol 10:2333. https://doi.org/10.3389/fmicb.2019.02333
Williams JE, Carrothers JM, Lackey KA et al (2017) Human milk microbial community structure is relatively stable and related to variations in macronutrient and micronutrient intakes in healthy lactating women. J Nutr 147:1739–1748. https://doi.org/10.3945/jn.117.248864
Treven P, Mahnič A, Rupnik M et al (2019) Evaluation of human milk microbiota by 16S rRNA gene next-generation sequencing (NGS) and cultivation/MALDI-TOF mass spectrometry identification. Front Microbiol 10:2612. https://doi.org/10.3389/fmicb.2019.02612
Kumar H, du Toit E, Kulkarni A et al (2016) Distinct patterns in human milk microbiota and fatty acid profiles across specific geographic locations. Front Microbiol 7:1619. https://doi.org/10.3389/fmicb.2016.01619
Gomez-Gallego C, Garcia-Mantrana I, Salminen S, Collado MC (2016) The human milk microbiome and factors influencing its composition and activity. Semin Fetal Neonatal Med 21:400–405. https://doi.org/10.1016/j.siny.2016.05.003
Lackey KA, Williams JE, Meehan CL et al (2019) What’s normal? Microbiomes in human milk and infant feces are related to each other but vary geographically: the INSPIRE study. Front Nutr 6:45. https://doi.org/10.3389/fnut.2019.00045
Fitzstevens JL, Smith KC, Hagadorn JI et al (2017) Systematic review of the human milk microbiota. Nutr Clin Pract 32:354–364. https://doi.org/10.1177/0884533616670150
Beghetti I, Biagi E, Martini S et al (2019) Human milk’s hidden gift: implications of the milk microbiome for preterm infants’ health. Nutrients 11:E2944. https://doi.org/10.3390/nu11122944
Rodríguez-Cruz M, Alba C, Aparicio M et al (2020) Effect of sample collection (manual expression vs. pumping) and skimming on the microbial profile of human milk using culture techniques and metataxonomic analysis. Microorganisms 8:E1278. https://doi.org/10.3390/microorganisms8091278
Vaidya YH, Patel SH, Patel RJ et al (2017) Human milk microbiome in urban and rural populations of India. Meta Gene 13:13–22. https://doi.org/10.1016/j.mgene.2017.04.001
Meehan CL, Lackey KA, Hagen EH et al (2018) Social networks, cooperative breeding, and the human milk microbiome. Am J Hum Biol 30:e23131. https://doi.org/10.1002/ajhb.23131
Gómez-Gallego C, Morales JM, Monleón D et al (2018) Human breast milk NMR metabolomic profile across specific geographical locations and its association with the milk microbiota. Nutrients 10:E1355. https://doi.org/10.3390/nu10101355
Moossavi S, Atakora F, Miliku K et al (2019) Integrated analysis of human milk microbiota with oligosaccharides and fatty acids in the CHILD cohort. Front Nutr 6:58. https://doi.org/10.3389/fnut.2019.00058
Hunt KM, Preuss J, Nissan C et al (2012) Human milk oligosaccharides promote the growth of staphylococci. Appl Environ Microbiol 78:4763–4770. https://doi.org/10.1128/AEM.00477-12
Section on Breastfeeding (2012) Breastfeeding and the use of human milk. Pediatrics 129:e827-841. https://doi.org/10.1542/peds.2011-3552
Italian Association of Human Milk Banks Associazione Italiana Banche del Latte Umano Donato (AIBLUD: www.aiblud.org), Arslanoglu S, Bertino E et al (2010) Guidelines for the establishment and operation of a donor human milk bank. J Matern Fetal Neonatal Med 23(Suppl 2):1–20. https://doi.org/10.3109/14767058.2010.512414
Agostoni C, Buonocore G, Carnielli VP et al (2010) Enteral nutrient supply for preterm infants: commentary from the European Society of Paediatric Gastroenterology, Hepatology and Nutrition Committee on Nutrition. J Pediatr Gastroenterol Nutr 50:85–91. https://doi.org/10.1097/MPG.0b013e3181adaee0
Peila C, Moro GE, Bertino E et al (2016) The effect of holder pasteurization on nutrients and biologically-active components in donor human milk: a review. Nutrients 8:E477. https://doi.org/10.3390/nu8080477
Landers S, Updegrove K (2010) Bacteriological screening of donor human milk before and after Holder pasteurization. Breastfeed Med 5:117–121. https://doi.org/10.1089/bfm.2009.0032
Capriati T, Goffredo BM, Argentieri M et al (2019) A modified holder pasteurization method for donor human milk: preliminary data. Nutrients 11:E1139. https://doi.org/10.3390/nu11051139
Escuder-Vieco D, Espinosa-Martos I, Rodríguez JM et al (2018) High-temperature short-time pasteurization system for donor milk in a human milk bank setting. Front Microbiol 9:926. https://doi.org/10.3389/fmicb.2018.00926
Deshpande G, Athalye-Jape G, Patole S (2018) Para-probiotics for preterm neonates-the next frontier. Nutrients 10:E871. https://doi.org/10.3390/nu10070871
Rautava S (2016) Early microbial contact, the breast milk microbiome and child health. J Dev Orig Health Dis 7:5–14. https://doi.org/10.1017/S2040174415001233
Milani C, Duranti S, Bottacini F et al (2017) The first microbial colonizers of the human gut: composition, activities, and health implications of the infant gut microbiota. Microbiol Mol Biol Rev 81:e00036-e117. https://doi.org/10.1128/MMBR.00036-17
Hapfelmeier S, Lawson MAE, Slack E et al (2010) Reversible microbial colonization of germ-free mice reveals the dynamics of IgA immune responses. Science 328:1705–1709. https://doi.org/10.1126/science.1188454
Gan XT, Ettinger G, Huang CX et al (2014) Probiotic administration attenuates myocardial hypertrophy and heart failure after myocardial infarction in the rat. Circ Heart Fail 7:491–499. https://doi.org/10.1161/CIRCHEARTFAILURE.113.000978
Gensollen T, Iyer SS, Kasper DL, Blumberg RS (2016) How colonization by microbiota in early life shapes the immune system. Science 352:539–544. https://doi.org/10.1126/science.aad9378
Allen-Blevins CR, Sela DA, Hinde K (2015) Milk bioactives may manipulate microbes to mediate parent-offspring conflict. Evol Med Public Health 2015:106–121. https://doi.org/10.1093/emph/eov007
Biesbroek G, Bosch AATM, Wang X et al (2014) The impact of breastfeeding on nasopharyngeal microbial communities in infants. Am J Respir Crit Care Med 190:298–308. https://doi.org/10.1164/rccm.201401-0073OC
Biesbroek G, Tsivtsivadze E, Sanders EAM et al (2014) Early respiratory microbiota composition determines bacterial succession patterns and respiratory health in children. Am J Respir Crit Care Med 190:1283–1292. https://doi.org/10.1164/rccm.201407-1240OC
Funkhouser LJ, Bordenstein SR (2013) Mom knows best: the universality of maternal microbial transmission. PLoS Biol 11:e1001631. https://doi.org/10.1371/journal.pbio.1001631
Jin L, Hinde K, Tao L (2011) Species diversity and relative abundance of lactic acid bacteria in the milk of rhesus monkeys (Macaca mulatta). J Med Primatol 40:52–58. https://doi.org/10.1111/j.1600-0684.2010.00450.x
O’Sullivan A, He X, McNiven EMS et al (2013) Metabolomic phenotyping validates the infant rhesus monkey as a model of human infant metabolism. J Pediatr Gastroenterol Nutr 56:355–363. https://doi.org/10.1097/MPG.0b013e31827e1f07
Quigley L, O’Sullivan O, Stanton C et al (2013) The complex microbiota of raw milk. FEMS Microbiol Rev 37:664–698. https://doi.org/10.1111/1574-6976.12030
Díaz-Ropero MP, Martín R, Sierra S et al (2007) Two Lactobacillus strains, isolated from breast milk, differently modulate the immune response. J Appl Microbiol 102:337–343. https://doi.org/10.1111/j.1365-2672.2006.03102.x
Maldonado J, Cañabate F, Sempere L et al (2012) Human milk probiotic Lactobacillus fermentum CECT5716 reduces the incidence of gastrointestinal and upper respiratory tract infections in infants. J Pediatr Gastroenterol Nutr 54:55–61. https://doi.org/10.1097/MPG.0b013e3182333f18
Cacho NT, Harrison NA, Parker LA et al (2017) Personalization of the microbiota of donor human milk with mother’s own milk. Front Microbiol 8:1470. https://doi.org/10.3389/fmicb.2017.01470
Author information
Authors and Affiliations
Contributions
AC, JC, GS, and MLG contributed to the conception and design of the manuscript. AC, JC, and GS wrote the first draft of the manuscript. DM, LC, FM, and MLG critically reviewed and revised the manuscript. All authors approved the final version of the manuscript as submitted.
Corresponding author
Ethics declarations
Ethics approval
Not applicable.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Communicated by Gregorio Paolo Milani.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Consales, A., Cerasani, J., Sorrentino, G. et al. The hidden universe of human milk microbiome: origin, composition, determinants, role, and future perspectives. Eur J Pediatr 181, 1811–1820 (2022). https://doi.org/10.1007/s00431-022-04383-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00431-022-04383-1