
Abstract
Physical fitness in childhood is considered a marker of current and future health. For this reason, there is a need for a simple but reliable test to assess the different components of physical fitness even at school during physical education lessons. However, standard values are required to correctly interpret the results of such tests. Hence, this study aimed to generate sex- and age-specific normative percentile values for health-related physical fitness in Italian children. To this aim, 30,472 children aged 6–11 years from the Friuli Venezia-Giulia region (Italy) were examined. The fitness test battery included the Léger test (cardiorespiratory), the shuttle test (agility), standing long jumps, frontal throws of a basketball (lower and upper limb strength), the sit-and-reach test (flexibility), and the standing balance test. Sex- and age-percentile curves were determined using the General Additive Model for Location Scale and Shape (GAMLSS).
Conclusion: The reference standards are provided as 1st, 3rd, 10th, 25th, 50th, 75th, 90th, 97th, and 99th percentiles in the form of both tables and charts and are roughly comparable with those of other European children.
What is Known: • Physical fitness in childhood is considered a marker of current and future health; • Several tests have been developed to assess physical fitness in children; • There are general European reference standards for a series of tests of the main fitness components for children. | |
What is New: • The present study provides specific reference standards for a series of tests that are indicative of the main fitness components and easily applied in children, particularly those in the Italian population; • Standing balance test and basketball frontal throw test references in a wide sample of children; • The performance of children in the present study was roughly comparable to that of other European children. |
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Physical fitness in childhood involves several health-related components, such as cardiorespiratory and muscular endurance, muscular strength, speed-agility, flexibility, and balance [1]. These components are considered markers of current and future health [2]. Some studies have shown that a low level of cardiorespiratory fitness is associated with cardiovascular diseases, some types of cancer, increased adiposity, and obesity [2]. Muscle strength is inversely related to cardiovascular diseases and metabolic risk factors [2] independent of cardiovascular fitness [3], and both upper and lower body muscle strength levels are considered important [4]. Additionally, muscle strength levels and speed-agility capacities are positively related to bone health and self-esteem [2]. Finally, even though there is only weak evidence indicating that flexibility and balance in childhood are correlated with health [5], the American College of Sports Medicine (ACSM) still includes exercise aimed at improving flexibility and balance in its guidelines for preventing worsening of physical fitness in adults [1] and elderly individuals. Since childhood physical fitness is important for public health [6], several tests have been developed to assess its components in a simple but reliable way. The Léger test is often used to evaluate cardiorespiratory fitness [7], and standing long jump and frontal throws of a basketball are considered reliable indices of lower [8] and upper [9] limb muscle fitness. In addition, the shuttle (10 × 5 m) [10], sit and reach [11], and standing balance [12] tests are considered reliable methods for evaluating speed-agility, flexibility, and balance, respectively. Sex- and age-specific reference values help identify children with a low level of fitness and promote healthy behaviours thereby preventing future health risks.
Although there are some reference values from different regions of the world [13], there is a scarcity of reference values for Italian children [13]. Even though reference from Europe already exist [14], there may be wide differences among countries or even within a single country [15]. Hence, this study aimed to generate sex- and age-specific normative percentile values for health-related physical fitness in Italian children aged between 6 and 11 years. Furthermore, this study aimed to provide a battery of tests by selecting the simplest tests to be performed.
Subjects and methods
A sample of 30,472 Italian schoolchildren (6–11 years old) involved in the “MOVIMENTO in 3S: promozione della Salute nelle Scuole attraverso lo Sport” (MOVIMENTO in 3S project: promoting Health in Schools through Sport) project was considered in the present study [6]. The project was a cross-sectional study; children were enrolled from different public schools in the Friuli Venezia-Giulia Region (Italy) between 2016 and 2018. One hundred thirty-seven of the 387 schools in the region joined the project and about 95% of the students of these schools participated in the measurements. The total number of primary schoolchildren in the Friuli Venezia Giulia region was about 60,000.
The experimental protocol was approved by the University of Udine Ethics Committee on Human Research for Medical Science. All the Children attending primary school were considered eligible for the study excluding those with any issues that prevented them from attending physical education classes. The procedures and purposes of the project were carefully explained to each child and his or her parents. Children gave verbal consent to participate and parents gave written informed consent. Thereafter, physical fitness tests were performed at the beginning and of each school year during school hours by a previously trained researcher to collect the data accurately and consistently.
Physical fitness
A battery of 6 tests was chosen to obtain a complete report of children’s physical fitness [16]. Priority was given to the use of tests that were easy to perform without the use of any special tools. The 6 tests were administered to the children on 6 different days during their class hours.
Cardiorespiratory fitness
Cardiorespiratory fitness was evaluated by a single repetition of the Léger test [16], which has been also validated in children [17, 18]. For the test, children were required to run back and forth continuously between two cones placed 20 m apart. A pre-recorded audio signal started to beep at pre-set intervals. The children had to follow the rhythm imposed by the beeps and the starting speed was selected at 8.5 km h−1. The children had to be in correspondence with the cone at each beep. Every minute the speed was increased by 0.5 km h−1 reducing the time between two consecutive beeps.
When the children being tested did not reach the final point in time or when the children stopped by fatigue, the last stage completed was recorded as their final score.
Speed-agility
Whole body speed-agility was evaluated by a shuttle test (10 × 5 m) [19,20,21,22], which has been validated in children [10]. Two lines have been depicted on the floor 5 m apart. At the “go!” signal, children had to run as fast as possible to the opposite line, cross it with both feet, run back across the starting line, and repeat the task for 10 shuttles (50 m), without brakes, in the shortest possible time. The best time of two trials was then taken into consideration.
Muscular power of the lower limbs
Lower limb explosive power was evaluated by means of a long jump test [12, 14, 19,20,21,22,23,24,25,26], which has been validated, by several authors, also in children [8, 16, 21]. Children were asked to jump for distance from a standing start. They were instructed to bend their knees with their arms in front of them, parallel to the ground, then to swing both arms and jump as far as possible, trying to land on their feet. The best trial between 3 tests was recorded.
Muscular power of the upper limbs
Upper limb power was evaluated by a frontal throw of a basketball (0.5 kg) [9]. The validity and reliability of this test has been previously confirmed [24]. Children were instructed to throw the basketball while sitting on the ground with their legs spread apart and with their back against the wall in order to use only upper limb’s muscles. The ball was thrown with two hands maintaining back contact with the wall. The distance of the throws was considered between the wall and the first point of contact of the ball on the ground. The best of three throws was recorded in centimetres.
Flexibility
Hip and low back flexibility was evaluated by the sit-and-reach test [12, 19,20,21,22, 24,25,26], which has been previously validated [11]. Children were asked to sit on the floor with legs stretched forward and knee locked and pressed against the floor. Shoes were removed and soles of the feet were placed flat against a box. Children stretched as far as possible along the measuring line and held that position for 1 to 2 s while the distance was measured. The level of the feet was considered to be 15 cm [27] in order to make all the values positive.
Static balance
The standing balance test evaluates balance capacity in children [12, 27], and it is considered valid and reliable [17, 18]. Children were asked to remove their shoes and to keep their balance on their preferred leg. The free leg had to be flexed at the knee, and the foot had to be held by the hand against the buttock of the same side while the contralateral hand remained fixed at the level of the hip. The test started after 1 min of practice. Time in seconds was considered the score of the test. The test was considered concluded either after 30 s, when the children moved their supporting foot, or when they lost contact between the heel of the non-supporting leg and the buttocks.
Statistical analysis
Statistical analyses were performed using the GAMLSS (General Additive Model for Location Scale and Shape) package 5.1-4 [28] of the statistical software R version 3.6.3. All physical fitness results were expressed as the mean and standard deviation (SD). To perform the analysis, the collected data were first screened for incorrect inclusions. The percentile curves for the fitness variables were stratified by sex and calculated as a function of age using the GAMLSS method. The percentile curves for the 1st, 3rd, 10th, 25th, 50th, 75th, 90th, 97th, and 99th percentiles were calculated based on the model that showed the best goodness of fit.
Results
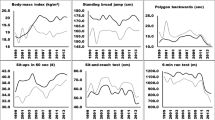
The initial selected sample (n: 30472) was screened for any incorrect inclusions and 41 children were deleted from the original database due to temporary physical issues preventing them from performing the tests. Then, 30,431 children were considered in the present study. Tables 1 and 2 and Figs. 1, 2, and 3 display the age- and sex-specific percentiles (P1, P3, P10, P25, P50, P75, P90, P97, and P99) for the different fitness tests in 30,431 Italian schoolchildren (6–11 years old). In the Léger test, boys performed better (P < 0.05) than girls, and older children performed better (P < 0.05) than younger children (Fig. 1a, b); in the speed-agility shuttle test, girls and boys had similar values, and older children performed worse (P < 0.05) than younger children (Fig. 1c, d). In the standing long jump test (Fig. 2a, b) and frontal throw test (Fig. 2 c, d), boys performed better (P < 0.05) than girls, and older children performed better (P < 0.05) than younger. In the sit-and-reach test, girls performed better (P < 0.05) than boys (Fig. 3a, b). In addition, girls’ performance decreased with age from P1 to P50, while it increased with age from P75 to P99; however, boys’ performance decreased with age from P1 to P99. Finally, in the standing balance test, boys and girls had similar values (Fig. 3c, d); moreover, in both sexes, the increment with age was maximal around P50 and tended to be lower when approaching both P99 and P1.

Percentile curves of the physical fitness (Léger test: a, b; speed-agility shuttle test: c, d), stratified by sex (girls: a, c; boys: b, d) and class of age (6–11 years old)

Percentile curves of the physical fitness (standing long jump test: a, b; frontal throw test: c, d), stratified by sex (girls: a, c; boys: b, d) and class of age (6–11 years old)

Percentile curves of the physical fitness (sit and reach test: a, b; standing balance test: c, d), stratified by sex (girls: a, c; boys: b, d) and class of age (6–11 years old)
Discussion
The present study provides age and sex reference standards for a series of tests indicative of the main fitness components that are easily applied in schoolchildren. The values for the percentiles presented are noteworthy because they come from a fairly wide sample of 30,431 children, and they could be very useful for educators. Moreover, they can be used to compare the fitness status of Italian children to that of European children and children worldwide. Finally, these reference standards can serve as a good reference for monitoring the decline in physical fitness state that is occurring in children around the world [29,30,31,32].
Because the relationship between cardiorespiratory fitness and health issues in children is well documented [2, 7, 33,34,35], the Léger test is often used to assess this important component at school [36]. The Léger test [17], also called the 20-m shuttle running test (20-mSRT), is one of the most widely used tests for evaluating cardiorespiratory fitness due to its validity and reliability and the ability to test a large number of children at the same time [37]. It can be scored by using the number of stages completed (as in the present study), the number of laps completed, or the speed reached at the last stage and allows us to estimate the maximal oxygen uptake [17, 38]. The values obtained in the present study were roughly comparable to those obtained previously in Spanish children [20, 39] and those in Tomkinson’s study [22], particularly for girls. Even though the study by Tomkinson included children and adolescents aged 9–17 years old from 30 European countries, it is not possible to compare values for the younger children. Moreover, our data from children aged >9 years were comparable to those from Australian children [40]. The review by Olds et al. [13], which included 37 countries from around the world, showed that Italian children were among the worst performers on the Léger test, whereas northern European countries were the best performers. However, the reference standards provided by the present study appear to be roughly in line with those of other European countries. Hence, the situation of the Italian children considered in the present study does not seem to be so compromised when compared with the situation of those from other European countries.
Speed-agility is strongly related to health as well, in particular to bone mineral density and bone mass accumulation later in life [2, 3, 5, 35]. There are a wide variety of tests aimed at evaluating speed-agility, often based on running patterns and changes in direction. The shuttle test is one of them [19,20,21,22], and it has been previously used several times to assess speed-agility in children and adolescents [19,20,21,22, 34]. Overall, the studies confirm that girls tend to have higher values than boys and that younger children have better performance than older children, not only in children the same age as those in our study [20] but also in adolescents until 17 years old [21, 22, 34]. Furthermore, our values appear to be in line with or slightly higher than those observed in Spanish children [20].
Muscular strength/fitness is one of the most studied fitness components in relation to health [2,3,4,5, 35]. In particular, the standing long jump is considered a general index of muscular fitness [4]. Our results were similar to those found in Spanish children of the same age [20] and European children aged 6 to 9 years old [14] but lower than those found in Polish [21] and Australian children older than 9 years old. However, in all these studies, as in ours, boys and older children had higher outcomes than girls and younger children, respectively [14, 20, 21, 40]. In terms of muscle fitness, upper body muscle fitness is considered an important predictor of heath in children [4]. One of the most commonly used tests to assess this component was the handgrip test [4, 14, 20, 21, 41]. However, in our opinion, it is very important to provide an easy-to-perform test that does not require special tools to evaluate upper body muscle fitness. In light of this, the basketball frontal throw test was developed [42]. Our results were slightly higher than those observed in Australian children and adolescents older than 9 years old [40]. In addition, to the best of our knowledge, this is the first study that has provided reference values for the basketball frontal throw test in a wide sample of children.
The flexibility standard reference values provided by the present study are in line with those for Spanish children [20]; moreover, older boys and girls showed less flexibility levels than younger boys, while girls were more flexible than boys. The reference values from Dobosz [21] showed that Polish boys performed better than Italian boys. Finally, the review by Catley and Tomkinson [40] shows higher values in Australian children than in the children in our study, but it is not clear if the differences were due to different methods of assessment.
To our knowledge, the present study was the first to provide a standing balance test reference in children. This may help promote the use of this test in assessing balance, since it has been proven to be reliable to evaluate balance capacity in children [12, 18]. Nevertheless, although our results on balance were not directly comparable with others, the trends whereby older individuals performed better than younger individuals [14, 21, 34] and girls performed better than boys [14, 34] were confirmed by other studies.
For a practical application of these data, educators, coaches, and all other people involved in children physical activity may consider these reference values of fitness status: very poor (X < P10); poor (P10 ≤ X < P25); medium (P25 ≤ X < P75); good (P75 ≤ X < P90); and very good (X < P90). The lowest percentiles, for example, 10th percentile, can represent a “warning signal” for further tests and investigations. Miguel-Etayo and colleagues [14] suggest that a fitness level below P5 is potentially pathological and cardiorespiratory and muscular fitness is particularly associated with health status [2]. Moreover, children with values below P25 may be introduced to training programmes to improve their fitness. On the other hand, children with values above the highest percentiles may be advised for further athletic developments.
A further aspect to be considered is the secular trend in children’s physical fitness; it seems that in many countries around the world, physical fitness has been worsening over the years [29,30,31,32, 38]. The study by Tomkinson et al. [38], which used the Léger test to assess cardiorespiratory fitness in 11 mainly developed countries around the world between 1980 and 2000, showed a marked decline in performance in both sexes, especially in older compared to younger individuals. In this light, the data provided by the present study may be useful for monitoring this phenomenon. Many factors can influence physical fitness, such as sex, age, children’s body mass index, and the amount of physical activity, and these factors are independently related to each other [43]. Indeed, the study by Zaqout et al. [33], in accordance with our data, showed that boys had better cardiorespiratory fitness and upper- and lower-limb strength than girls, while girls had better balance and flexibility. Furthermore, increased body mass index (BMI) was related to lower cardiorespiratory fitness, flexibility and lower limb strength, balance, and increased upper limb strength as previously reported [6], while higher physical activity was connected to the improvement of all components of physical fitness except balance [43]. Children’s BMI is also positively associated with their mother’s obesity, but, luckily, CRF and muscular strength mitigate this relationship [44]. Therefore, physical fitness and physical activity are important, and the role of the school may be crucial, on the one hand, to identify children with low physical fitness levels and, on the other hand, to encourage children to be active. However, physical activity programmes should aim to improve not only cardiorespiratory fitness but also muscular fitness and speed-agility [2]. For this reason, physical activity is recommended in the form of both structured and unstructured activity in children; in particular, aerobic exercise is recommended daily, while activity focused on muscle and bone strengthening should be prescribed at least 3 days per week [45]. Recent findings [46] suggest that also active videogaming may be beneficial.
Two of the main strengths of the present study are the large number of children involved and the fact that all tests are easy to perform at school without specific tools. Furthermore, to the best of our knowledge, this is the first study to provide reference values of the standing balance test in children. On the other hand, the two main limitations are (1) the design of the study is cross-sectional while it would be preferable to obtain data from a longitudinal study on growing children and (2) the children included in the sample come from a single region of Italy.
In conclusion, our results provide reference standards for a complete series of tests that are indicative of the main components of physical fitness and applicable to children aged between 6 and 11 years. It is important to note that the tests included in this work are easy to perform without any specific tools.
Furthermore, the performance of children in the present study was roughly comparable to that of other European children, and our data could be useful for monitoring the secular trend of physical fitness in children, which has been decreasing over the years.
Data availability
N/A
Abbreviations
- 20-mSRT:
-
Léger test, also called 20-m shuttle running test
- Pn:
-
n percentile
- GAMLSS:
-
General Additive Model for Location Scale and Shape method
References
Garber CE, Blissmer B, Deschenes MR, Franklin BA, Lamonte MJ, Lee IM, Nieman DC, Swain DP (2011) Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise. Med Sci Sports Exerc 43:1334–1359. https://doi.org/10.1249/MSS.0b013e318213fefb
Ortega FB, Ruiz JR, Castillo MJ, Sjostrom M (2008) Physical fitness in childhood and adolescence: a powerful marker of health. Int J Obes 32:1–11. https://doi.org/10.1038/sj.ijo.0803774
Smith JJ, Eather N, Morgan PJ, Plotnikoff RC, Faigenbaum AD, Lubans DR (2014) The health benefits of muscular fitness for children and adolescents: a systematic review and meta-analysis. Sports Med 44:1209–1223. https://doi.org/10.1007/s40279-014-0196-4
Castro-Piñero J, Laurson KR, Artero EG, Ortega FB, Labayen I, Ruperez AI, Zaqout M, Manios Y, Vanhelst J, Marcos A, Polito A, Gonzalez-Gross M, Widhalm K, Moreno LA, Gutierrez A, Ruiz JR (2019) Muscle strength field-based tests to identify European adolescents at risk of metabolic syndrome: the HELENA study. J Sci Med Sport 22:929–934. https://doi.org/10.1016/j.jsams.2019.04.008
Ruiz JR, Castro-Pinero J, Artero EG, Ortega FB, Sjostrom M, Suni J, Castillo MJ (2009) Predictive validity of health-related fitness in youth: a systematic review. Br J Sports Med 43:909–923. https://doi.org/10.1136/bjsm.2008.056499
Fiori F, Bravo G, Parpinel M, Messina G, Malavolta R, Lazzer S (2020) Relationship between body mass index and physical fitness in Italian prepubertal schoolchildren. PLoS One 15:e0233362. https://doi.org/10.1371/journal.pone.0233362
Raghuveer G, Hartz J, Lubans DR, Takken T, Wiltz JL, Mietus-Snyder M, Perak AM, Baker-Smith C, Pietris N, Edwards NM, On behalf of the American Heart Association Young Hearts Athero, Hypertension and Obesity in the Young Committee of the Council on Lifelong Congenital Heart Disease and Heart Health in the Young (2020) Cardiorespiratory fitness in youth: an important marker of health: a scientific statement from the American Heart Association. Circulation 142:e101–e118. https://doi.org/10.1161/CIR.0000000000000866
Fernandez-Santos JR, Ruiz JR, Cohen DD, Gonzalez-Montesinos JL, Castro-Piñero J (2015) Reliability and validity of tests to assess lower-body muscular power in children. J Strength Cond Res 29:2277–2285. https://doi.org/10.1519/JSC.0000000000000864
Gallotta MC, Marchetti R, Baldari C, Guidetti L, Pesce C (2009) Linking coordinative and fitness training in physical education settings. Scand J Med Sci Sports 19:412–418. https://doi.org/10.1111/j.1600-0838.2008.00796.x
Fjørtoft I, Pedersen AV, Sigmundsson H, Vereijken B (2011) Measuring physical fitness in children who are 5 to 12 years old with a test battery that is functional and easy to administer. Phys Ther 91:1087–1095. https://doi.org/10.2522/ptj.20090350
Muyor JM, Zemková E, Štefániková G, Kotyra M (2014) Concurrent validity of clinical tests for measuring hamstring flexibility in school age children. Int J Sports Med 35:664–669. https://doi.org/10.1055/s-0033-1353217
Ceschia A, Giacomini S, Santarossa S, Rugo M, Salvadego D, da Ponte A, Driussi C, Mihaleje M, Poser S, Lazzer S (2016) Deleterious effects of obesity on physical fitness in pre-pubertal children. Eur J Sport Sci 16:271–278. https://doi.org/10.1080/17461391.2015.1030454
Olds T, Tomkinson G, Léger L, Cazorla G (2006) Worldwide variation in the performance of children and adolescents: an analysis of 109 studies of the 20-m shuttle run test in 37 countries. J Sports Sci 24:1025–1038. https://doi.org/10.1080/02640410500432193
De Miguel-Etayo P, Gracia-Marco L, Ortega FB et al (2014) Physical fitness reference standards in European children: the IDEFICS study. Int J Obes 38(Suppl 2):S57–S66. https://doi.org/10.1038/ijo.2014.136
Chillón P, Ortega FB, Ferrando JA, Casajus JA (2011) Physical fitness in rural and urban children and adolescents from Spain. J Sci Med Sport 14:417–423. https://doi.org/10.1016/j.jsams.2011.04.004
CDS (1993) Eurofit. European test of physical fitness, 2nd edn. Council of Europe, Strasburg
Léger LA, Mercier D, Gadoury C, Lambert J (1988) The multistage 20 metre shuttle run test for aerobic fitness. J Sports Sci 6:93–101. https://doi.org/10.1080/02640418808729800
Artero EG, Espaa-Romero V, Castro-Piero J et al (2011) Reliability of field-based fitness tests in youth. Int J Sports Med 32:159–169. https://doi.org/10.1055/s-0030-1268488
Tokmakidis SP, Kasambalis A, Christodoulos AD (2006) Fitness levels of Greek primary schoolchildren in relationship to overweight and obesity. Eur J Pediatr 165:867–874. https://doi.org/10.1007/s00431-006-0176-2
Gulías-González R, Sánchez-López M, Olivas-Bravo Á, Solera-Martínez M, Martínez-Vizcaíno V (2014) Physical fitness in Spanish schoolchildren aged 6-12 years: reference values of the battery EUROFIT and associated cardiovascular risk. J Sch Health 84:625–635. https://doi.org/10.1111/josh.12192
Dobosz J, Mayorga-Vega D, Viciana J (2015) Percentile values of physical fitness levels among Polish children aged 7 to 19 years--a population-based study. Cent Eur J Public Health 23:340–351. https://doi.org/10.21101/cejph.a4153
Tomkinson GR, Carver KD, Atkinson F, Daniell ND, Lewis LK, Fitzgerald JS, Lang JJ, Ortega FB (2018) European normative values for physical fitness in children and adolescents aged 9–17 years: results from 2 779 165 Eurofit performances representing 30 countries. Br J Sports Med 52:1445–1456. https://doi.org/10.1136/bjsports-2017-098253
Ruiz JR, Castro-Pinero J, Espana-Romero V, Artero EG, Ortega FB, Cuenca MM, Jimenez-Pavon D, Chillon P, Girela-Rejon MJ, Mora J, Gutierrez A, Suni J, Sjostrom M, Castillo MJ (2011) Field-based fitness assessment in young people: the ALPHA health-related fitness test battery for children and adolescents. Br J Sports Med 45:518–524. https://doi.org/10.1136/bjsm.2010.075341
Sacchetti R, Ceciliani A, Garulli A, Masotti A, Poletti G, Beltrami P, Leoni E (2012) Physical fitness of primary school children in relation to overweight prevalence and physical activity habits. J Sports Sci 30:633–640. https://doi.org/10.1080/02640414.2012.661070
Armstrong MEG, Lambert MI, Lambert EV (2017) Relationships between different nutritional anthropometric statuses and health-related fitness of South African primary school children. Ann Hum Biol 44:208–213. https://doi.org/10.1080/03014460.2016.1224386
Gontarev S, Kalac R, Velickovska L, Stojmanovska D, Misovski A, Milenkovski J (2018) Health-related physical fitness of normal, stunted and overweight children aged 6-14 years in Macedonia. Nutr Hosp 35:1208–1214. https://doi.org/10.20960/nh.1794
Morrow JR, Zhu W, Franks DB et al (2009) 1958–2008: 50 years of youth fitness tests in the United States. Res Q Exerc Sport 80:1–11. https://doi.org/10.1080/02701367.2009.10599524
Stasinopoulos DM, Rigby RA (2007) Generalized Additive Models for Location Scale and Shape (GAMLSS) in R. J Stat Soft 23. https://doi.org/10.18637/jss.v023.i07
Tomkinson GR, Olds TS (2007) Secular changes in aerobic fitness test performance of Australasian children and adolescents. Med Sport Sci 50:168–182. https://doi.org/10.1159/000101361
Runhaar J, Collard DCM, Singh AS, Kemper HCG, van Mechelen W, Chinapaw M (2010) Motor fitness in Dutch youth: differences over a 26-year period (1980–2006). J Sci Med Sport 13:323–328. https://doi.org/10.1016/j.jsams.2009.04.006
Dyrstad SM, Berg T, Tjelta LI (2012) Secular trends in aerobic fitness performance in a cohort of Norwegian adolescents: secular trend in aerobic fitness performance. Scand J Med Sci Sports 22:822–827. https://doi.org/10.1111/j.1600-0838.2011.01315.x
Hardy LL, Barnett L, Espinel P, Okely AD (2013) Thirteen-year trends in child and adolescent fundamental movement skills: 1997–2010. Med Sci Sports Exerc 45:1965–1970. https://doi.org/10.1249/MSS.0b013e318295a9fc
Zaqout M, Michels N, Bammann K et al (2016) Influence of physical fitness on cardio-metabolic risk factors in European children. The IDEFICS study. Int J Obes 40:1119–1125. https://doi.org/10.1038/ijo.2016.22
Venckunas T, Mieziene B, Emeljanovas A (2018) Aerobic capacity is related to multiple other aspects of physical fitness: a study in a large sample of Lithuanian schoolchildren. Front Physiol 9:1797. https://doi.org/10.3389/fphys.2018.01797
Evaristo S, Moreira C, Lopes L, Oliveira A, Abreu S, Agostinis-Sobrinho C, Oliveira-Santos J, Póvoas S, Santos R, Mota J (2019) Muscular fitness and cardiorespiratory fitness are associated with health-related quality of life: results from LabMed physical activity study. J Exerc Sci Fit 17:55–61. https://doi.org/10.1016/j.jesf.2019.01.002
Lang JJ, Tomkinson GR, Janssen I et al (2018) Making a case for cardiorespiratory fitness surveillance among children and youth. Exerc Sport Sci Rev 46:66–75. https://doi.org/10.1249/JES.0000000000000138
Ruiz JR, Ortega FB, Gutierrez A, Meusel D, Sjöström M, Castillo MJ (2006) Health-related fitness assessment in childhood and adolescence: a European approach based on the AVENA, EYHS and HELENA studies. J Public Health 14:269–277. https://doi.org/10.1007/s10389-006-0059-z
Tomkinson GR, Léger LA, Olds TS, Cazorla G (2003) Secular trends in the performance of children and adolescents (1980-2000): an analysis of 55 studies of the 20m shuttle run test in 11 countries. Sports Med 33:285–300. https://doi.org/10.2165/00007256-200333040-00003
Castro-Piñeiro J (2011) Percentile values for aerobic performance running/walking field tests in children aged 6 to 17 years; influence of weight status. Nutr Hosp 162–168. https://doi.org/10.3305/nh.2011.26.3.4597
Catley MJ, Tomkinson GR (2013) Normative health-related fitness values for children: analysis of 85347 test results on 9–17-year-old Australians since 1985. Br J Sports Med 47:98–108. https://doi.org/10.1136/bjsports-2011-090218
Cadenas-Sanchez C, Intemann T, Labayen I, Peinado AB, Vidal-Conti J, Sanchis-Moysi J, Moliner-Urdiales D, Rodriguez Perez MA, Cañete Garcia-Prieto J, Fernández-Santos JR, Martinez-Tellez B, Vicente-Rodríguez G, Löf M, Ruiz JR, Ortega FB (2019) Physical fitness reference standards for preschool children: the PREFIT project. J Sci Med Sport 22:430–437. https://doi.org/10.1016/j.jsams.2018.09.227
Fernandez-Santos JR, Ruiz JR, Gonzalez-Montesinos JL, Castro-Piñero J (2016) Reliability and validity of field-based tests to assess upper-body muscular strength in children aged 6-12 years. Pediatr Exerc Sci 28:331–340. https://doi.org/10.1123/pes.2014-0196
Zaqout M, Vyncke K, Moreno LA, de Miguel-Etayo P, Lauria F, Molnar D, Lissner L, Hunsberger M, Veidebaum T, Tornaritis M, Reisch LA, Bammann K, Sprengeler O, Ahrens W, Michels N (2016) Determinant factors of physical fitness in European children. Int J Public Health 61:573–582. https://doi.org/10.1007/s00038-016-0811-2
Brand C, Fochesatto CF, Dias AF, Gaya AR, de Lucena Martins CM, Renner JDP, Reuter CP, Kelishadi R (2020) Child’s body mass index and mother’s obesity: the moderating role of physical fitness. Eur J Pediatr. https://doi.org/10.1007/s00431-020-03810-5
Bushman BA (2014) Kids and physical activity - who, what, why, and how. 18:6
Coknaz D, Mirzeoglu AD, Atasoy HI, Alkoy S, Coknaz H, Goral K (2019) A digital movement in the world of inactive children: favourable outcomes of playing active video games in a pilot randomized trial. Eur J Pediatr 178:1567–1576. https://doi.org/10.1007/s00431-019-03457-x
Acknowledgements
We are grateful to the children who participated in this study, their parents, teachers, and the directors of the Schools and the Institution for their cooperation. We thank the Sports Sciences PhD students at the School of Sport Sciences of the University of Udine (Italy), for their qualified assistance during the study. We thank the Friuli Venezia Giulia Regional Health Department, Public Education Department and Sport Department, Friuli Venezia Giulia Regional Italian Olympic Committee, Friuli Venezia Giulia Regional Italian Paralympic Committee, for their support during the study.
Author information
Authors and Affiliations
Contributions
SL conceived the overall study, all the authors contributed to design the research and to make the measurements. GB analysed the data. FV wrote the manuscript with the help of FF and GB. SL, MP, GM, RM revised the manuscript. All the authors read and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This article does not contain any studies with human participants or animals performed by any of the authors. The experimental protocol was approved by the University of Udine Ethics Committee on Human Research for Medical Science. Before the study began, the purpose and objectives were carefully explained to each child and his or her parents. Children gave their verbal consent, and written informed consent was obtained from their parents.
Consent for publication
Patients signed informed consent regarding publishing their data
Conflict of interest
The authors declare no conflict of interest.
Code availability
N/A
Additional information
Communicated by Gregorio Paolo Milani
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Vaccari, F., Fiori, F., Bravo, G. et al. Physical fitness reference standards in Italian children. Eur J Pediatr 180, 1789–1798 (2021). https://doi.org/10.1007/s00431-021-03946-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00431-021-03946-y