
Abstract
Some studies of infants with acute respiratory distress have demonstrated that neurally adjusted ventilator assist (NAVA) had better short-term results compared to non-triggered or other triggered models. We determined if very prematurely born infants with evolving or established bronchopulmonary dysplasia (BPD) had a lower oxygenation index (OI) on NAVA compared to assist control ventilation (ACV). Infants were studied for 1 h each on each mode. At the end of each hour, blood gas analysis was performed and the OI calculated. The inspired oxygen concentration (FiO2), the peak inflation (PIP) and mean airway pressures (MAP) and compliance were averaged from the last 5 min on each mode. Nine infants, median gestational age of 25 (range 22–27) weeks, were studied at a median postnatal age of 20 (range 8–84) days. The mean OI after 1 h on NAVA was 7.9 compared to 11.1 on ACV (p = 0.0007). The FiO2 (0.36 versus 0.45, p = 0.007), PIP (16.7 versus 20.1 cm H2O, p = 0.017) and MAP (9.2 versus 10.5 cm H2O, p = 0.004) were lower on NAVA. Compliance was higher on NAVA (0.62 versus 0.50 ml/cmH2O/kg, p = 0.005).
Conclusion: NAVA compared to ACV improved oxygenation in prematurely born infants with evolving or established BPD.
What is Known: • Neurally assist ventilator adjust (NAVA) uses the electrical activity of the diaphragm to servo control the applied pressure. • In infants with acute RDS, use of NAVA was associated with lower peak inflation pressures and higher tidal volumes. |
What is New: • This study uniquely reports infants with evolving or established BPD, and their results were compared on 1 h each of NAVA and assist controlled ventilation. • On NAVA, infants had superior (lower) oxygen indices, lower inspired oxygen concentrations and peak and mean airway pressures and higher compliance. |
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Whilst the survival of babies born very prematurely has improved, many will develop bronchopulmonary dysplasia (BPD) and chronic respiratory morbidity. New modes of ventilation have been developed with the aim of reducing lung injury and improving respiratory outcomes. One such mode is neurally adjusted ventilatory assist (NAVA). NAVA uses the electrical activity of the diaphragm (Edi), captured by a specialised nasogastric tube with an array of electrodes (the Edi catheter), to servo control the applied ventilator pressure. The Edi is used both to trigger each inflation and also to determine the level of support proportional to the infant’s neural drive to breathe throughout each inflation [11]. Inflations are off-cycled when the Edi falls by a prespecified amount. The clinician sets the NAVA level or gain factor by which the Edi signal at each point in time is “translated” into airway pressure provided. The change in electrical activity of the diaphragm that triggers inflation is earlier in the respiratory cycle than the change in flow which is used in other trigger modes; hence, the trigger delay is shorter on NAVA [4]. Edi may be a more accurate method to detect the infant’s inspiratory efforts and hence, there would be less ineffective or wasted effort and auto or double triggering.
In infants with acute respiratory distress, in randomised and non-randomised crossover studies, NAVA has been shown to have superior results compared to non-triggered and other triggered modes, but only with regard to pressure levels and lung function. Studies have not addressed clinically important outcomes such as the length of intubation or mortality. In a randomised crossover study of 4-h periods comparing synchronised intermittent mandatory ventilation (SIMV) with pressure support, NAVA was shown to have a lower peak airway pressure in preterm infants born between 24 and 36 weeks [8]. In a non-randomised study, five premature infants with a mean gestational age of 26 weeks were studied at a median postnatal age of 7 days [13]. They were ventilated for consecutive 4-h periods on NAVA followed by pressure controlled ventilation, and the sequence was repeated three times. The peak inflation pressure (PIP) was lower and the tidal volumes and compliance were higher on NAVA [13]. A non-randomised, crossover study of two 12h periods of pressure-regulated volume control ventilation followed by NAVA was performed on 19 infants with a median gestational age of 31.8 weeks. NAVA resulted in lower peak inspiratory pressures and the tidal volumes of the infants were lower on NAVA [9]. In addition, on NAVA, the asynchrony index was lower and there were no neural apnoeas. [9].
Infants with evolving or established bronchopulmonary dysplasia (BPD) have a high resistance of the respiratory system which means flow triggering can be challenging. During NAVA, flow triggering is not used [4]. Previous studies have assessed infants with acute respiratory distress who have very different lung function to those with evolving or established BPD. Hence, it cannot be assumed that similar results from those with acute respiratory distress would be achieved in those with established or evolving BPD. Hence, the aim of our study was to uniquely test the hypothesis that NAVA compared to assist control ventilation (ACV) would result in a lower OI in infants with evolving or established BPD.
Methods
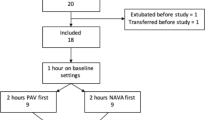
The study was undertaken at King’s College Hospital NHS Foundation Trust between December 2015 and June 2016. Infants were eligible for this randomised, crossover study if they were born at less than 32 weeks of gestation and remained ventilated at 1 week of age on assist control ventilation (ACV). Eligible infants were identified on a daily basis by a researcher by discussion with the clinical team. A local audit of 100 consecutive infants born at less than 32 weeks of gestation had demonstrated 95% of those who remained ventilator dependent at 1 week of age developed BPD, that is oxygen dependency beyond 28 days. Those with major congenital abnormalities (that is requiring surgical correction) or receiving neuromuscular blockade were excluded. All infants were clinically stable with assessed. The study was approved by the West Midlands - Solihull Research Ethics Committee. Written, informed parental consent was obtained.
Infants at King’s College Hospital NHS Foundation Trust are routinely supported by the SLE 5000 (software versions 4.3; SLE Ltd., South Croydon, UK). All infants were ventilated with Coles shouldered endotracheal tubes which have been shown to have minimal or no leaks [7]. Volume targeting was not used. On entry into the study, the infants were transferred from ACV on the SLE 5000 to ACV (named ‘Pressure Control’ on the Servo-n ventilator, Maquet Critical Care, Solna, Sweden). The same ventilator settings and backup rate were used. In particular, the positive end expiratory pressure (PEEP) was kept at 4–5 cm H2O as had been used prior to the study and the inflation time was set, as previously, at 0.36 to 0.4 s. The apnoea time was set to 2 s and the upper pressure limit at least 5 cm H2O higher than the baseline settings, but did not exceed 30 cm H2O. A six French Edi catheter was inserted and correct positioning confirmed as per the instructions of the manufacturer using the Edi catheter positioning guide function on the ventilator (Magnet Servo-n User Manual Version 1.1). The guide function displays the retrocardiac echocardiograph. Correct positioning was when the P waves and QRS complexes were visible in the uppermost leads and then decreased in size until the P waves disappeared in the lowest lead. Coloured highlighting of the central two leads appeared once the catheter was in the correct place. Once correct positioning was confirmed, the catheter was securely attached to the infant’s face using an adhesive dressing. After 1 h of stabilisation on the Servo-n ventilator using the settings described above, blood gas analysis was performed. Infants were then randomised to receive either ACV or NAVA first for 1 h and then to receive the alternative mode for a subsequent hour. The order in which the infants received the two modes was randomised between each baby using a sequential opaque sealed envelope system. Before the infant was changed to NAVA mode, the NAVA level was adjusted so that the displayed pressure waveform on NAVA closely matched the actual pressure waveform on the baseline settings, aiming for the peak Edi to be between 5 and 15 μV as per the recommendations of the manufacturer. The baseline ventilator settings were used to determine the backup settings to be used on NAVA in the absence of an Edi signal.
The initial ventilator settings were noted, and the number and duration of desaturations (defined as oxygen saturation less than 88%) were noted on each ventilator mode. The FiO2 was adjusted with the aim of maintaining oxygen saturations between 92 and 96%. At the end of each hour, capillary blood gas analysis was performed and the oxygenation index (OI) calculated as the inspired oxygen concentration (FiO2) x mean airway pressure (MAP) × 100/pO2. The FiO2, the PIP, MAP, tidal volume and respiratory system compliance (calculated from the tidal volume divided by the PIP) were recorded from the ventilator displays and averaged from the last 5 min of each 1-h period. The data were down-loaded into excel via a USB stick.
Sample size
The planned sample size was 18 infants, as this would allow detection of a difference in oxygenation index between the two modes of one standard deviation, with 80% power and 5% significance. An interim analysis was planned to take place half way through, i.e. after nine patients, as our studies with proportional assist ventilation (PAV), a ventilation mode which also provides tailored support throughout the infant’s inspiratory cycle, demonstrated the OI on PAV was better in all patients than on ACV [2, 12]. In order to preserve the type I error at 5%, the interim analysis was conducted at 0.01 with the final analysis conducted using 0.04. This gave an overall type 1 error rate (significance level) of 5% [(1–0.01) × (1–0.04) = 0.95 = 1–0.05]. If the interim analysis showed p < 0.01, then the trial was to stop and the final analyses conducted using the nine patients treated to that point.
Analysis
The results were positively skewed and, therefore, log-transformed for analysis so that a paired t test could be used. Using that method, the results including the mean and confidence intervals are on the ratio scale [3]. Results were back-transformed to give geometric means for each mode of ventilation. The ratio of geometric means and the corresponding 95% confidence intervals for the ratio are presented. The ratio of the geometric means can be interpreted as the percentage difference between a result on NAVA compared to on ACV. The desaturation data were discrete and analysed using the Wilcoxon signed-rank test. Data were analysed using Stata v 14.
Results
At the interim analysis, the comparison of the OI on NAVA versus ACV was statistically significant using the modified cut-off for significance described above. The OI was lower on NAVA for all infants (Table 1). Hence, the clinical and statistics team agreed that the trial be stopped at that point and the data analysed.
Nine infants had been assessed, seven males and two females. Their median gestational age was 25 (range 22–27) weeks and median birthweight 750 (range 545–830) grammes. The infants were studied at a median postnatal age of 20 (range 8–84) days. All had received at least one dose of antenatal steroids and postnatal surfactant and were on caffeine at the time of the study. Only one infant was receiving sedation and this was at the same dose throughout the study. Five of the infants were studied first on NAVA and four on ACV. There was no suggestion that the size of difference in OI was greater with order (i.e. with either ACV then NAVA or NAVA then ACV). Neither was there any suggestion that the order (by chance) was related to the size of value, i.e. no suggestion that all those with a high starting OI received the modalities in the same order (p = 0.66).
The ratio of the geometric means for the OI, the primary outcome, was 0.72 (NAVA/ACV), showing that the mean OI was 28% lower on NAVA compared to ACV with corresponding 95% CIs from 62 to 83% (Table 1). Infants who had the highest OIs on ACV tended to have a larger reduction in OI when studied on NAVA (Table 1). The mean PIP (p = 0.017) and mean MAP (p = 0.004) were significantly lower on NAVA, as was the mean FiO2 (p = 0.007). The mean compliance (p = 0.005) and oxygen saturation (p = 0.016) were significantly higher on NAVA. The means for the tidal volume, respiratory rate and peak Edi and the number of desaturations were not significantly different between the two modes (Table 2).
Discussion
We have demonstrated that in infants born very prematurely and with evolving or established BPD, NAVA compared to ACV resulted in a significantly lower oxygenation index. This was associated with significantly lower PIPs and MAPs, likely reflecting that during NAVA the applied pressure is servo-controlled throughout each inflation. On ACV, although inflation is triggered by the beginning of the infant’s inspiratory effort, the start of inflation may have been delayed as a flow trigger was used. Furthermore, after the inflation is triggered during ACV, neither the inflation pressure nor time is tailored to the infant’s inspiratory efforts. The higher compliance on NAVA compared to ACV reflects the lower PIPs with similar tidal volumes. A higher compliance on NAVA has been previously reported in neonatal and paediatric patients [1, 5, 6]. Our results suggest that infants with the highest OIs, i.e. the most severe lung disease, had the greatest reduction in OI during NAVA. This may reflect, as above, the shorter trigger delay on NAVA which means more of the infant’s breath is pressure supported.
There are strengths and some limitations to our study. As the same ventilator was used for each mode, the significant differences demonstrated are due to the differences in the modes, rather than differences in the ventilator performance. Although infants were only studied for an hour on each mode, we have demonstrated significant differences between the two modes. The infants included had a wide range of severity of respiratory disease as suggested by their PIP and FiO2, yet we saw a positive effect of NAVA in all infants. The infants had also had a wide range of postnatal ages, but we have shown in an audit of 100 consecutive prematurely born infants, 95% of those who remained ventilator dependent at 1 week developed BPD. Thus, we feel our results demonstrate that compared to ACV, NAVA use was associated with superior results in infants with evolving or established BPD. We used capillary blood samples to calculate the OIs. We used this method at the end of each of the two periods in all infants, thus the use of capillary blood sampling did not bias our results. The infants were all clinically stable when assessed and none were seriously ill, had shock, hypotension or peripheral vasoconstriction at the time of assessment [10]. Thus, we feel it was appropriate to calculate the OIs from the capillary blood samples. Only one infant was receiving sedation and this was at the same dose throughout the study, so this did not influence the results. We used a crossover design as this removes the variability between patients by looking at effects within them. As we have demonstrated no order effect, the design gives more precision. We stopped the trial at the planned interim analysis as in all infants the OI was lower on NAVA. We did not demonstrate a significant difference in the peak Edi between the two modes, although there was a trend for it to be lower on NAVA. This may have been due to insufficient redistribution of work from the patient to the ventilator, as the NAVA level was only adjusted so that the estimated pressure waveform closely matched the pressure waveform on the baseline settings.
We have previously demonstrated that proportional assist ventilation (PAV), when compared to ACV, resulted in improved oxygenation [2, 12] and a reduced work of breathing [2] in infants with evolving or established bronchopulmonary dysplasia. Both PAV and NAVA provide support in proportion to the respiratory effort throughout each breath. Our results suggest that such modes are superior to ACV. As yet, there are no randomised controlled trials with long-term outcomes assessing either NAVA or PAV and therefore, any potential long term benefit remains unknown.
In conclusion, we have demonstrated in a randomised crossover study that NAVA, compared to ACV, resulted in improved (lower) oxygenation index and this was associated with lower peak and mean airway pressures.
Abbreviations
- ACV:
-
Assist control ventilation
- BPD:
-
Bronchopulmonary dysplasia
- Edi:
-
Electrical activity of the diaphragm
- FiO2 :
-
Inspired oxygen concentration
- MAP:
-
Mean airway pressures
- NAVA:
-
Neurally assist ventilator adjust
- OI:
-
Oxygenation index
- PEEP:
-
Positive end expiratory pressure
- PIP:
-
Peak inflation pressure
- RDS:
-
Respiratory distress syndrome
References
Beck J, Reilly M, Grasselli G, Mirabella L, Slutsky AS, Dunn MS, Sinderby C (2009) Patient-ventilator interaction during neurally adjusted ventilatory assist in low birth weight infants. Pediatr Res 65:663–668
Bhat P, Patel D-S, Hannam S, Rafferty GF, Peacock JL, Milner AD, Greenough A (2015) Crossover study of proportional assist versus assist control ventilation. Arch Dis Child Fetal Neonatal Ed 100:F35–F38
Bland JM, Altman DG (1996) Statistics notes. Logarithms BMJ 312:700
Bordessoule A, Emeriaud G, Morneau S, Jouvet P, Beck J (2012) Neurally adjusted ventilatory assist improves patient–ventilator interaction in infants as compared with conventional ventilation. Pediatr Res 72:194–202
Breatnach C, Conlon NP, Stack M, Healy M, O’Hare BP (2010) A prospective crossover comparison of neurally adjusted ventilatory assist and pressure-support ventilation in a pediatric and neonatal intensive care unit population. Pediatr Crit Care Med 11:7–11
de la Oliva P, Schüffelmann C, Gómez-Zamora A, Villar J, Kacmarek RM (2012) Asynchrony, neural drive, ventilatory variability and COMFORT: NAVA versus pressure support in pediatric patients. A non-randomized cross-over trial. Intensive Care Med 38:838–846
Hird M, Greenough A, Gamsu HR (1990) Gas trapping during high frequency positive pressure ventilation using conventional ventilators. Early Hum Dev 22:51–56
Lee J, Kim H-S, Sohn JA, Lee JA, Choi CW, Kim EK, Kim BI, Choi JH (2012) Randomized crossover study of neurally adjusted ventilatory assist in preterm infants. J Pediatr 161:808–813
Longhini F, Ferrero F, De Luca D, Cosi G, Alemani M, Colombo D, Cammarota G, Berni P, Conti G, Bona G, Della Corte F, Navalesi P (2015) Neurally adjusted ventilatory assist in preterm neonates with acute respiratory failure. Neonatology 107:60–67
McLain BI, Evans J, Dear PR (1988) Comparison of capillary and arterial blood gas measurements in neonates. Arch Dis Child 63:743–747
Navalesi P, Longhini F (2015) Neurally adjusted ventilatory assist. Curr Opin Crit Care 21:58–64
Shetty S, Bhat P, Hickey A, Peacock JL, Milner AD, Greenough A (2016) Proportional assist versus assist control ventilation in premature infants. Eur J Pediatr 175:57–61
Stein H, Alosh H, Ethington P, White DB (2013) Prospective crossover comparison between NAVA and pressure control ventilation in premature neonates less than 1500 grams. J Perinatol 33:452–456
Authors’ contributions
Professor Greenough and Dr. Ali designed the study and approved the final manuscript as submitted. Dr. Shetty and Dr. Hunt collected the data and approved the final manuscript as submitted. Professor Peacock designed the statistical analysis and analysed the data and approved the final manuscript as submitted. All authors were involved in the preparation of the manuscript and approved the final manuscript as submitted.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Funding
Dr. Hunt is supported by a grant from the Charles Wolfson Charitable Trust. Dr. Shetty was supported by funding from King’s College Hospital NHS Foundation Trust in recognition of Professor Greenough’s NIHR Senior Investigator Award. The research was supported by the National Institute for Health Research (NIHR) Biomedical Research Centre based at Guy’s and St Thomas’ NHS Foundation Trust and King’s College London. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health.
Conflict of interest
AG has held grants from various ventilator manufacturers and has received honoraria for giving lectures and advising various ventilator manufacturers. The Servo-n ventilator was loaned to us by Marquet Critical Care, Solna, Sweden. They were not involved in the study design, data collection, data analysis or production of the manuscript.
Informed consent
Infants whose parents gave informed written consent were recruited.
Additional information
Communicated by Patrick Van Reempts
Rights and permissions
About this article

Cite this article
Shetty, S., Hunt, K., Peacock, J. et al. Crossover study of assist control ventilation and neurally adjusted ventilatory assist. Eur J Pediatr 176, 509–513 (2017). https://doi.org/10.1007/s00431-017-2866-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00431-017-2866-3