
Abstract
Objective
The aim of this paper is to describe characteristics associated with maltreatment types in children referred to the child protection team at the University Children’s Hospital Zürich. Since 2003, the child protection team has registered data on each case in a standardized form.
Methods
To examine differences in gender, age, nationality, and socioeconomic status by type of maltreatment, regression analyses were conducted for the 1,484 cases that were referred from 2003 to 2006.
Results
The most common types of referred maltreatment were sexual (38%) and physical maltreatment (31%) with mean ages of 8.4 and 7 years, respectively. Compared to physical maltreatment, where gender distribution was equal, there was a higher risk for girls to become victims of sexual maltreatment. Younger children were at higher risk for neglect (mean age 5 years). Low socioeconomic status increased the risk for physical as compared to sexual maltreatment. However, whether the child was of Swiss or of foreign nationality was not associated with an increased risk for any type of maltreatment when controlling for socioeconomic status.
Conclusion
As this study is one of a few to analyze characteristics in child maltreatment referred to a hospital child protection team, further research is needed. To improve international comparability, thorough documentation of the cases is encouraged.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Fifty years ago, the first multidisciplinary child protection teams (CPTs) were introduced in the USA [4]. The first clinical child protection team in Switzerland was formed at University Children’s Hospital Zürich in 1969. Today, team approaches to the diagnosis and treatment of child maltreatment are common: in Switzerland, 20 out of 36 children’s hospitals or departments have a CPT. The teams bring together professionals with different backgrounds—in the case of Zürich, three pediatricians, a pediatric surgeon, a child psychiatrist, a child psychologist, two social workers, and two pediatric nurses. Each case is evaluated by a representative subgroup of the team. Besides hospital CPTs and other voluntary institutions confronted with maltreated and neglected children (e.g., child and adolescent psychiatric services, social services), Swiss legislation provides “tutelary authorities” with the power to ordain protection measures in favor of children [12, 36]. In most cases, these authorities confine a general and unspecified mandate to a professional in a general social service or a child protection agency appointing him/her as assistant or, in more severe cases, tutor. As many European states, Switzerland knows no mandatory reporting legislation for most professionals working with children or adolescents [22].
Although CPTs have been established for quite a while in different places and states, only few articles are published that report data of CPT cases in hospitals [3, 13, 15, 16, 20, 21, 26–28, 33, 35], and just two of them are from Europe [8, 34]. The available data differ in various aspects, making it difficult to compare or generalize. First, CPTs differ considerably in their definitions of maltreatment [15, 20, 26, 33], and, second, they often focus on specific types of maltreatment, mainly sexual [13, 16, 21, 27] or physical [8], sometimes combined with a focus on specific age groups [28]. Finally, comparability of data is complicated by the fact that some studies focus on interventions, diagnoses, or perpetrators [3, 15, 34, 35] and describe only few comparable demographics of their sample. Therefore, the findings to date are more or less exploratory.
Not surprisingly, the most prominent type of maltreatment reported to CPTs at hospitals in different parts of the world are violations of child’s physical well-being [14, 20, 25, 26, 33, 34], although definitions of this category differ from narrow to wide. No clear picture can be drawn regarding the distribution of gender and age within maltreatment subtypes except for sexual maltreatment, where more girls are reported than boys [16, 20, 26]. Whereas older studies published mean ages in early childhood [14, 15, 26], more recent publications [3, 20] displayed mean ages around 7 years. This may reflect the changes since the first description of the battered child syndrome [17] to today’s conceptions of child abuse and neglect affecting children at all ages. Findings with regard to cultural variables remain even more obscure. As the ethnic groups in US studies [14, 15, 20, 26] were not matched to types of maltreatment, it remains unclear whether one of the ethnic groups was overrepresented in any of the maltreatment types. In any case, the ethnic situation in USA hospitals hardly compares to the ethnic composition of the hospital population of a Western European country like Switzerland. All the same, it seems important to account for different cultural backgrounds, as 22% of Swiss population is of foreign nationality, which is a considerably higher percentage than in the majority of European countries [5]. Further support for consideration of cultural factors comes from the only other CPT study in Switzerland: Ferrier et al. [8] found that foreigners were overrepresented in their sample of physically maltreated children in Geneva. Researchers in the field of child maltreatment and neglect have pointed out that cultural background should not be examined without considering social class [10, 19]. Garbarino and Ebata [10] report that ethnic differences in child sexual abuse are very small when group socioeconomic resources are considered and controlled. CPT data on socioeconomic resources are very rare; only Paluszny et al. [26] indicate that increased unemployment is to be associated with physical maltreatment.
Aims
The aim of this study was twofold: first, we assessed the characteristics of a large CPT sample at a Swiss University Children’s Hospital in association with types of maltreatment. Second, we examined the role of sociodemographic variables (gender, age, nationality, socioeconomic status) in predicting maltreatment types. Based on the previous findings presented above, we postulated two hypotheses. First, we expect more girls than boys to be sexually maltreated. Second, we assume that foreign nationals will be overrepresented in the physical maltreatment sample.
Materials and methods
Sample
Since 2003, the CPT at University Children’s Hospital Zürich has been capturing important features of every referred child in a standardized form. From 2003 to 2006, a total of 1,484 children and adolescents were referred to the CPT, with an annual range varying between 350 patients in 2005 and 385 patients in 2004. Reports of child maltreatment and neglect reach the CPT through different channels: besides hospital inpatients (18%) and outpatients (28%), around half of the cases (54%) originated through external reports (telephone calls) from the victims themselves, affected relatives, teachers, or institutions confronted with child maltreatment and neglect (e.g., child and adolescent psychiatric services, school psychologists, social services).
Measures
The CPT applies a definition of child maltreatment based on the widely accepted guidelines from a Swiss governmental expert group [2]. Therein, child maltreatment is defined as a nonaccidental, conscious or unconscious, and physical or psychological impairment through persons (parents, caregivers, or third), institutions, or social structures that lead to injuries, developmental impairment, or death. Subtypes were categorized as physical, sexual, or psychological maltreatment, neglect, or Munchausen syndrome by proxy (MSBP; Table 1). The certainty of maltreatment was differentiated into substantiated, suspicious, or unlikely [19]. Relying on criteria defined in the standard work by Monteleone and Brodeur [24], the maltreatment of a child was deemed to be substantiated if physical or psychological symptoms were most likely explained by it or if the child disclosed the maltreatment towards medical professionals. If physical or psychological symptoms were explicable through known illnesses or accidents, the maltreatment was judged to be unlikely. A maltreatment that could neither be substantiated nor dismissed was judged to be suspicious. If multiple types of maltreatment had been suspected, the case was categorized as the substantiated maltreatment type. If several categories had been substantiated, physical or sexual maltreatment were labeled instead of psychological maltreatment or neglect. Where the family environment was deemed risky but maltreatment had not (yet) occurred, the situation was referred to as “risk of maltreatment.” This label is useful in clinical practice, as it earmarks cases where preventive measures are needed. However, the “risk of maltreatment” situations cannot be qualified as a further maltreatment category because they represent an earlier stage. They were therefore excluded from further analyses. The labeling of the type as well as the certainty of maltreatment was obtained through consensus in CPT meetings.
Analyses of the victims’ sociodemographic characteristics included gender, age, nationality, and socioeconomic status. Nationality was dichotomized, with the child categorized as either Swiss or foreign national. As no direct data on prosperity were available, the proportion of the population in the child’s neighborhood receiving public assistance was used to estimate the socioeconomic level of the child’s family [9]. This further analysis was conducted for a subsample of children residing in the city of Zürich, of whom 238 could be matched, via registered addresses, to one of the city’s 12 districts [30, 31]. In the years 2003 to 2006, the city districts had averages of people receiving assistance between 1.6% and 10.9% with a total city average of 6.25%. As the rate of persons receiving public assistance is an imprecise estimate of the family’s socioeconomic level, only families residing in the two city districts with the lowest rates were labeled as of upper socioeconomic status (9%), and families residing in the two districts with the highest rates were labeled as of lower socioeconomic status (20%). This leaves the majority of the city districts—and with them the majority of the subsample (71%)—in the middle socioeconomic range.
The separate analysis of the CPT patients in the city of Zürich has to take into account a significantly different distribution as compared to the rest of the CPT population: the subsample contains a higher ratio of (hospital) internal patients (59%) than in the remaining areas (39%; χ 2(3) = 29.84; p < 0.001). This arises from the exclusion of 120 externally referred where the victims lived in the city of Zürich but for whom no address was on register. With no addresses, their socioeconomic status could not be approximated via the rate of persons receiving assistance in the neighborhood.
Statistical analyses
Distributions of categorical variables in maltreatment types were analyzed using chi-squared tests and differences in age means by maltreatment type using analysis of variance (ANOVA). To predict the probability of maltreatment types out of multiple variables, multinomial logistic regression analyses were conducted. In a first step, gender and age were analyzed as independent variables in the whole sample. For the city of Zürich subsample, child’s nationality and socioeconomic status were introduced as further independent variables. Regarding the prominent role of physical maltreatment in hospital settings [14, 20, 25, 26, 33, 34], it is set as base outcome for the regressions, and other categories are compared to it. To take differences between the categories of certainty and the reporting channels into account, these variables are included as controls in the statistical analyses. To this purpose, the latter variable was dichotomized into internal and external reports.
Differences between sample and subsample were analyzed using t tests for age means; chi-squared test was used for the comparison of the distributions of categorical variables. All statistical analyses were conducted using the software Stata 10 [29].
Results
Sample characteristics
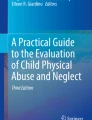
In 568 children and adolescents (38%) referred to the CPT at the University Children’s Hospital Zürich, sexual maltreatment was suspected. Physical maltreatment was suspected in 459 patients (31%). Together, these categories account for 69% of the CPT caseload. The remaining patients were referred due to suspected psychological maltreatment (n = 215) or neglect (n = 110) or because the child’s situation was deemed as risk of maltreatment (n = 126). MSBP was rarely suspected (n = 6), and it was substantiated in only two cases. It is also obvious from Fig. 1 that the maltreatment types differed respectably in their substantiation rate: sexual maltreatment often remained suspicious (46%)—meaning that, whereas the allegation of maltreatment could not be substantiated, there was reason to suspect that the child had been sexually maltreated—in contrast to psychological maltreatment with only 21% suspicious cases. Few of the referrals were judged unlikely except for physical maltreatment referrals, where the rate was somewhat higher (16% unlikely). Because they were judged to be unlikely and because some of the subgroups contained fewer than five cases, the unlikely maltreatments were excluded from further analyses which associated demographic variables with maltreatment subtype.

Substantiation rate for the different types of maltreatment (N = 1,358)
Most of the psychologically or sexually maltreated children reached the CPT through external referrals (67% or 59%, respectively). The rate of external referrals was lower in neglect (45%) and physical maltreatment (44%).
Sociodemographic variables predicting maltreatment types
Some sample characteristics were introduced as predictors in multinomial logistic regressions to analyze the strength of their connection with specific types of maltreatment. For these further analyses, the sample was reduced: first, the cases with unlikely maltreatment and risk of maltreatment were excluded. Second, as statistical analyses of small groups are susceptible to biases, the six MSBP cases were excluded as well. This left a total of 1,257 maltreated children and adolescents in the sample. For these patients, the genders are quite equally distributed between the maltreatment types, except for sexual maltreatment, where victims are female in 76% of the cases (Table 2). As compared to physical maltreatment, girls are much more likely to be sexually maltreated than boys (Table 3). As sexual maltreatment is the most frequent type of maltreatment seen by the CPT, the high rate of female victims is the reason for the higher total of girls (62%) in the sample. While children were referred at all ages, mean age of the maltreated children ranges from 5 years in neglected to 8.4 years in sexually maltreated children. Compared to the mean age of 7 years in physically maltreated children, younger children are at significantly higher risk of being neglected, and older children are at a significantly higher risk of being sexually maltreated (Table 3).
The connection between nationality, socioeconomic status, and maltreatment type was examined in a subsample of children residing in the city of Zürich. The rate of children originating from foreign nations varies from 38% in physical maltreatment to 27% in sexual maltreatment and neglect (Table 2). The chi-squared test indicates that the differences in this distribution are not statistically significant. However, socioeconomic status is unevenly distributed among the different maltreatment types (Table 2). Lower socioeconomic status is more common in physical maltreatment (33%) and neglect (36%) than in psychological (16%) and sexual maltreatment (13%). Here, the multinomial logistic regression shows a higher risk for children with lower socioeconomic status to become victims of physical than sexual maltreatment (Table 4). Rates of families with upper socioeconomic status differ from 4% in physical to 14% in psychological maltreatment. With a cell count of fewer than five cases in physical maltreatment and neglect, there were insufficient cases in these categories for statistical analysis.
Mean ages do not differ between the whole sample and the city of Zürich subsample in nondirectional t tests (neglect: t = 0.07, p = 0.947; psychological maltreatment: t = 0.31, p = 0.754; physical maltreatment: t = −1.51, p = 0.131; sexual maltreatment: t = −0.40, p = 0.690). And also in the subsample, there is a higher risk for younger children to become victims of neglect as compared to physical maltreatment (Table 4). However, with more variables introduced in the multinomial logistic regression of this subsample, there is no longer an age-bound risk of sexual maltreatment as compared to physical maltreatment. As the chi-squared test indicates (χ 2(1) = 1.92; p = 0.17), gender distribution in the subsample does not differ from the main sample. The higher risk of girls to become victims of sexual as compared to physical maltreatment also holds true in the subsample (Table 4).
Discussion
This study analyzed the characteristics of a large sample of maltreated children that were referred from 2003 to 2006 to a child protection team at one of the university children’s hospitals in Switzerland. Physical and sexual maltreatments were by far the most common types. Sexually maltreated children were mainly externally referred to the CPT via telephone calls, and only about half of the referrals could be substantiated. On the other hand, physical maltreatments were mainly referred when suspected in inpatients or outpatients and had a higher substantiation rate than the sexual maltreatment referrals.
As other studies suggest [14, 34], physical maltreatment is a common phenomenon referred to the CPT at University Children’s Hospital Zürich. However, this CPT handles even more sexually maltreated children and adolescents. Unlike other hospitals’ CPT [3, 8, 13, 15, 16, 20, 21, 27, 28, 33, 34], the CPT at University Children’s Hospital Zürich also takes in external referrals, and these often concern sexual maltreatment. This may also be due to the fact that the CPT at the University Children’s Hospital Zürich is an established institution dealing with sexual maltreatment. It is well known among authorities who often ask the CPT for support and refer children and adolescents. Almost half of the referrals for sexual maltreatment remain suspicious. In fact, assessment of sexual maltreatment is difficult, as it is seldom possible to substantiate it by concrete evidence like bruises in physical maltreatment or bad hygiene in neglect [38]. On the other hand, the highest rate of unlikely maltreatments is found in physical maltreatment. According to the signal detection paradigm, an elevated rate of false alarms indicates a liberal criterion in differentiating between the “signal” and the distracting “noise” [6]. Physical maltreatment is probably quite readily detected, leading to more false alarms but—in turn—also to fewer undetected cases.
Sample characteristics differ in their respective strength as predictors of different maltreatment types. Compared to the physical maltreatment, girls are at a significantly higher risk to be victims of sexual maltreatment, and young children are at a significantly higher risk for neglect. Contrary to previous studies, no specific risk was connected to nationality. On the other hand, there was a specific risk associated with socioeconomic status: compared to sexual maltreatment, lower socioeconomic status children are at a higher risk to be physically maltreated.
Apart from the surplus of girls as victims of sexual maltreatment, gender distribution for the different maltreatment types is more or less even. This finding is supported elsewhere [16, 20]. Except for the true difference in gender of sexually maltreated children, Watkins and Bentovim [37] point out some more reasons that may account for fewer boys being reported, such as boys being more reluctant to disclose the maltreatment because they fear being disbelieved or being labeled as homosexual. Results regarding the age of the referred children are ambiguous. Analyzed together with gender in the whole sample, sexually maltreated children are on average significantly older than physically maltreated. There is often no physical sign of sexual maltreatment [11], so there have to be other, mainly verbal, hints that child sexual maltreatment occurred. Developmental factors, particularly cognitive limitations, may inhibit disclosure in young children [11], which may partly account for the age difference. However, the difference is no longer significant, if age and gender are analyzed together with nationality and socioeconomic status in a subsample. This mixed evidence qualifies the explanation mentioned above. Both in the main sample and the subsample, for younger children, there is a higher risk to be neglected as compared to physically maltreated. As neglect is the most understudied and consequently the least understood type of maltreatment [7, 23], this result is difficult to interpret. We suspect that the types of neglect encountered in hospitals are more common in younger children and neglect types in older children are presented elsewhere.
In the city of Zürich subsample, the ratio of foreign nationals in physical maltreatment is somewhat higher than in neglect or sexual maltreatment and also somewhat higher than the ratio of foreign nationals in the population of the city of Zürich [31]. This agrees with the findings of Ferrier et al. [8] in Geneva. However, there is no significant difference between the ratios of foreign nationals by maltreatment type when socioeconomic status is accounted for. This reinforces the finding by Garbarino and Ebata [10] that ethnic differences in child sexual abuse are very small, when group socioeconomic resources are considered and controlled. On the other hand, socioeconomic resources differ between the maltreatment types: physically maltreated children are more often of lower socioeconomic status than sexually maltreated children, reinforcing Paluszny et al. [26]. Possibly, physical maltreatment is partially a helpless but damaging reaction associated with impaired environmental resources, whereas sexual maltreatment is based on factors other than a lack of environmental resources.
However, results concerning socioeconomic status should be interpreted cautiously, as the use of rate of persons receiving public assistance is merely an estimate for this variable. In addition, differences between the urban setting of the city of Zürich and the remaining areas minimize generalization. Apart from the weaknesses of the socioeconomic status variable, there are other limitations that should be taken into account. First, only one type of maltreatment per child was categorized, although the co-occurrence of multiple types is common [1]. Second, the presented variables represent only a small choice of the factors that are possibly connected with the risk of different maltreatment types. Other potentially correlated variables, such as the child being handicapped [32] or adopted, were not analyzed, as they have not been registered systematically. Third, the categories of “unlikely” and “risk of maltreatment” have been excluded although there remains a possibility that some children excluded were actually maltreated—a fact research concerned with child maltreatment will always be confronted with. Finally, the labeling of the child protection case (type of maltreatment, certainty) has been reached through consensus in the CPT and has not been validated externally.
Conclusions
Future research is needed to clarify the role of age, nationality, and socioeconomic status and to identify further case characteristics varying between the types of maltreatment. In future studies, special attention should be given to socioeconomic status by not just approximating it but by collecting it properly. As there are still a lot of different taxonomies of child maltreatment and neglect in hospitals, effort should be put into revising them for better comparability. This includes the definitional issue of the “risk of maltreatment” situations. The risk factors leading to the label should be collected, too. If these risk factors are also assessed in cases where maltreatment has occurred, future research should be able to learn about the potential damage of a respective risk factor. These aims necessarily rely on thorough documentation of the CPT cases. We encourage other CPTs to use standardized forms and to support efforts to introduce comparable categories in the areas of maltreatment types, sociodemographics, perpetrators, and interventions.
References
Arata CM, Langhinrichsen-Rohling J, Bowers D et al (2007) Differential correlates of multi-type maltreatment among urban youth. Child Abuse Negl 31(4):393–415
Arbeitsgruppe Kindesmisshandlung (1992) Kindesmisshandlungen in der Schweiz. Eidgenössische Drucksachen- und Materialzentrale, Bern
Benbenishty R, Chen W (2003) Decision making by the child protection team of a medical center. Health Soc Work 28(4):284–292
Bross DC, Ballo N, Korfmacher J (2000) Client evaluation of a consultation team on crimes against children. Child Abuse Negl 24(1):71–84
Bundesamt für Statistik (2006) Ausländerinnen und Ausländer in der Schweiz. Bundesamt für Statistik, Neuchâtel
Dopke CA, Lundahl BW, Dunsterville E et al (2003) Interpretations of child compliance in individuals at high- and low-risk for child physical abuse. Child Abuse Negl 27(3):285–302
Dubowitz H (2007) Understanding and addressing the “neglect of neglect:” digging into the molehill. Child Abuse Negl 31(6):603–606
Ferrier PE, Schaller M, Girardet I (1985) Abused children admitted to a pediatric in-patient service in Switzerland: a ten-year experience and follow-up evaluation. Child Abuse Negl 9(3):373–381
Freisthler B, Merritt DH, LaScala EA (2006) Understanding the ecology of child maltreatment: a review of the literature and directions for future research. Child Maltreat 11(3):263–280
Garbarino J, Ebata A (1983) The significance of ethnic and cultural differences in child maltreatment. J Marriage Fam 45(4):773–783
Goodman-Brown TB, Edelstein RS, Goodman GS et al (2003) Why children tell: a model of children's disclosure of sexual abuse. Child Abuse Negl 27(5):525–540
Häfeli C (2005) Wegleitung für vormundschaftliche Organe, 4th edn. kdmz, Zürich
Hall A (1988) The development of a multi-disciplinary approach to the assessment and management of child sexual abuse in an inner city Health District. Health Trends 20(2):39–43
Hampton RL, Newberger EH (1985) Child abuse incidence and reporting by hospitals: significance of severity, class, and race. Am J Public Health 75(1):56–60
Hochstadt NJ, Harwicke NJ (1985) How effective is the multidisciplinary approach? A follow-up study. Child Abuse Negl 9(3):365–372
Jones DA, Trudinger P, Crawford M (2004) Intelligence and achievement of children referred following sexual abuse. J Paediatr Child Health 40(8):455–460
Kempe CH, Silverman FN, Steele BF et al (1962) The battered-child syndrome. JAMA 181:17–24
Kruttschnitt C, McLeod J, Dornfeld M (1994) The economic environment of child abuse. Soc Probl 41(2):299–315
Leeb RT, Paulozzi L, Melanson C et al (2008) Child maltreatment surveillance: uniform definitions for public health and recommended data elements, version 1.0. Centers for Disease Control and Prevention, National Center for Injury Prevention and Control, Atlanta
Levy HB, Markovic J, Chaudhry U et al (1995) Reabuse rates in a sample of children followed for 5 years after discharge from a child abuse inpatient assessment program. Child Abuse Negl 19(11):1363–1377
Lynch DL, Stern AE, Oates RK et al (1993) Who participates in child sexual abuse research? J Child Psychol Psychiatry 34(6):935–944
Mathews B, Kenny MC (2008) Mandatory reporting legislation in the United States, Canada, and Australia: a cross-jurisdictional review of key features, differences, and issues. Child Maltreat 13(1):50–63
McSherry D (2007) Understanding and addressing the “neglect of neglect”: why are we making a mole-hill out of a mountain? Child Abuse Negl 31(6):607–614
Monteleone JA, Brodeur AE (1998) Child maltreatment: a clinical guide and reference. Whaley, St. Louis
Oral R, Can D, Kaplan S et al (2001) Child abuse in Turkey: an experience in overcoming denial and a description of 50 cases. Child Abuse Negl 25(2):279–290
Paluszny MJ, Cullen BJ, Funk J et al (1989) Child abuse disposition: concurrences and differences between a hospital team, child protection agency and the court. Child Psychiatry Hum Dev 20(1):25–38
Roane TH (1992) Male victims of sexual abuse: a case review within a child protective team. Child Welfare 71(3):231–239
Skellern CY, Wood DO, Murphy A et al (2000) Non-accidental fractures in infants: risk of further abuse. J Paediatr Child Health 36(6):590–592
StataCorp (2007) Stata statistical software: release 10. StataCorp LP, College Station
Statistik Stadt Zürich (2006) Statistisches Jahrbuch der Stadt Zürich 2005/2006. Statistik Stadt Zürich, Zürich
Statistik Stadt Zürich (2008) Statistisches Jahrbuch der Stadt Zürich 2008. Statistik Stadt Zürich, Zürich
Sullivan PM, Knutson JF (2000) Maltreatment and disabilities: a population-based epidemiological study. Child Abuse Negl 24(10):1257–1273
Thomas DE, Leventhal JM, Friedlaender E (2001) Referrals to a hospital-based child abuse committee: a comparison of the 1960s and 1990s. Child Abuse Negl 25(2):203–213
Thun-Hohenstein L (2006) Interdisciplinary child protection team work in a hospital setting. Eur J Pediatr 165(6):402–407
Vitulano LA, Lewis M, Doran LD et al (1986) Treatment recommendation, implementation, and follow-up in child abuse. Am J Orthopsychiatr 56(3):478–480
Voll P, Jud A, Mey E et al (2008) Zivilrechtlicher Kindesschutz: Akteure, Prozesse, Strukturen. Interact, Luzern
Watkins B, Bentovim A (1992) The sexual abuse of male children and adolescents: a review of current research. J Child Psychol Psychiatry 33(1):197–248
Weber MW (1997) The assessment of child abuse: a primary function of child protective services. In: Helfer ME, Kempe RS, Krugman RS (eds) The battered child. University of Chicago Press, Chicago, pp 120–149
Acknowledgments
This study was funded by the “Perspectives” foundation of Swiss Life, Zürich, and the Olga Mayenfisch Foundation, Zürich. The authors have no financial relationship with the organizations that sponsored the research.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Jud, A., Lips, U. & Landolt, M.A. Characteristics associated with maltreatment types in children referred to a hospital protection team. Eur J Pediatr 169, 173–180 (2010). https://doi.org/10.1007/s00431-009-1001-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00431-009-1001-5