
Abstract
Despite its incidence, there are still few reports in literature relating to tinnitus in children. Almost all data were collected by means of questionnaires or in a limited population of children. In order to collect data in a homogeneous way and directly from the patients, the protocol of study proposed by Savastano has been applied to 1,100 children. The results showed tinnitus as present in 374 children but only 6.5% of the cases complained spontaneously about it. In all, 76.4% of the children demonstrated normal hearing, whereas 64.5% reported being bothered by their tinnitus. Tinnitus measurements were obtained and are reproducible in all patients older than 8 years of age. The loudness level was <10 dB in 48.6% of cases, which was higher than 10 dB in 51.4%. As for the frequency distribution, in most cases it appears to be between 0 and 1,000 Hz. There is a correspondence between the loudness level and masking level. A total inhibition of <60 s for most children with lower loudness was obtained. The present study demonstrates that the application in the infancy of a specific protocol of study allows the presence of tinnitus to be discovered, giving specific and detailed information about it so as to minimize its damage to be obtained. Moreover, for the first time, data regarding the measurement of tinnitus in childhood has been gathered.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Tinnitus in childhood, despite its incidence, has been a neglected problem which has begun to receive more consideration over the last decades [1, 4, 5, 11]. There are still few reports in literature relating to tinnitus in children and in most cases the data are collected through questionnaires. Tinnitus is a relatively common symptom in childhood, but children rarely complain spontaneously of it; when they are able to describe it, openly or when questioned, their complaints are often minimized or not taken seriously by adults [2].
The discrepancy between the high incidence of tinnitus and low rate of spontaneous complaint in children may be explained by the fact that they consider tinnitus to be a normal event, as it has usually been present for a long period of time. A second explanation for this discrepancy lies in the fact that the child may not distinguish between the presence of tinnitus and its medical significance. Another explanation could be that children are more easily distracted by their external environment than adults and so, while playing or doing various things, they may forget about their tinnitus [12].
Even if a child does not mention the existence of tinnitus, nevertheless, it may cause difficulties in concentration and bring about behavioural problems such as irritation, nervousness, deterioration in the lingual capacity, learning and writing difficulties. The presence of tinnitus has also been reported in children with normal hearing function even if comparative studies have found tinnitus to be more common in those with a mild to moderately severe (PTA up to 70 dB) hearing deficit [5].
Most of the data referred to in literature have been obtained from the results of questionnaires or limited to age ranges [4, 5] or limited to subjects with otological and/or hearing pathology [1, 8, 12]. Not until now have the tinnitus subjective characteristics and measurements in childhood been described in young consecutive patients.
Considering that tinnitus in children exists and may provoke serious consequences, a protocol of study in order to identify and analyze the symptom was proposed in 2002 by Savastano [11]. The following steps are considered: (1) an accurate medical history regarding in particular previous otological problems and/or head injuries; (2) an investigation into the presence of tinnitus that specifically concerns tinnitus; (3) an otological examination in order to exclude ear pathologies; (4) an audiological examination for a complete study of the symptoms.
The present study refers to the results obtained from the application of this protocol to a wide population of children who attended, not only for a specific otological problem, the ENT Department of Padua University.
Materials and methods
The present study considered 1,100 consecutive children. Only children aged 6 years and over were included, since below this age, consistent answers could not be obtained. Mean age was 11.9 (min 6, max 16; Fig. 1), 368 were female and 732 were male. Subjects with severe neurological and/or psychiatric disturbances were excluded. All children underwent the tinnitus protocol of study for children proposed by Savastano in 2002.

Percentage distribution of age of children with tinnitus
After the personal data and the general and otological medical history, the following steps were performed: (1) tinnitus subjective investigation pertaining to presence of noise in the ear, ability to describe it; and (2) a subjective description, which includes a general description (similar noise), laterality (right, left, bilateral, in the head), pitch description and level description. The level description is then broken down into the duration, including intermittent (most of the time/some of the time) or continuous. Additionally there is the annoyance degree (always annoyed/seldom annoyed, very annoyed/little annoyed); and the severity of tinnitus in regards to causing worry (not at all/slightly/sometimes/more severely).
After these subjective data were collected, the following tests were performed: (1) pure tone audiometry, which gives information about the hearing function of the child; (2) tympanometry, which indicates the possible presence of middle ear pathologies, which are quite frequent in childhood, and confirms the audiometric threshold; (3) tinnitus measurements, including tinnitus loudness and spectral composition, masking effectiveness and residual inhibition. The pitch of the tinnitus is determined by a matching procedure and the difference between the threshold and the sensation level is considered to be the tinnitus loudness. On the basis of the loudness level, the children were divided into 2 groups: group I presenting a level <10 dB; and group II with a >10-dB level. An eventual correspondence between a subjective judgement expressed for the intensity and tinnitus measurement value for the loudness, divided into low (<10 dB ), medium (between 10 and 15 dB) and high (>15 dB), was considered. Furthermore, both the masking level and the residual inhibition were compared to the loudness values.
The masking was performed with a wide frequency band noise in the ear affected by tinnitus; its value consists of the difference between the threshold level of the masking sound and the threshold necessary to mask tinnitus completely. Masking levels were divided into 0–30 dB, 31–60 dB and >60 dB. Residual inhibition was measured by presenting the masking signal for 1 min and observing, once the stimulus was suspended, the period of time for which tinnitus was inhibited. Three classes of residual inhibition were considered: partial (tinnitus still present), total (tinnitus completely disappeared) <60 s and >60 s.
The degree of hearing loss, when present, of each child was classified according to Mills and Cherry (mean threshold 1–4 Hz: 20–40 dB mild; 40–60 dB moderate; 60–80 dB severe; >100 dB profound)[8]. The chi-square test was applied to evaluate the statistical significance.
Results
Tinnitus resulted as being present in 374 children (34% of cases), 249 boys, 125 girls, with a mean age of 11.9. Only 71 children (6.5%) complained spontaneously of tinnitus, while the symptom in the remaining 303 subjects (27.5%) was detected when they were specifically questioned according to the protocol utilized. The great number of children that did not complain spontaneously is statistically significant compared to the number of children that complained spontaneously (χ2=1382.3;p<0.0001). In 31.6%, pre-existent middle-ear pathology was reported, while in 14% otological flogosis was present at the moment of observation. In all, 76.4 % of the children (286 cases) demonstrated normal hearing (χ2=20;p <0.001) while in 23.6% of cases (88 children), a hearing loss was detected, which was mild in 74 cases (2 sensorineural: 1, 2 and 4 KHz; 72 conductive: low-medium frequencies), moderate in 11 cases (1 sensorineural: all frequencies; 10 conductive: low frequencies), severe in 3 cases (all sensorineural: for all frequencies). Tympanometry was normal in 221 children (59%) and abnormal (middle ear negative pressure) in 55 subjects (14.7%) without significant statistical difference compared to children without tinnitus (p >0.05). Tympanometry was not performed in 98 children which were unable to cooperate. In 8% of the cases, there was a clinical history of meningitis, in 10% of cases there was a past history of ventilation tube insertion, in 25% a head injury and in 9% of cases a noise trauma (noisy toys, air-bag deployment, explosion trauma, headphones).
As far as the specific characteristics of tinnitus are concerned, 241 children (64.5%) reported being bothered by their tinnitus: always in 45 cases, seldom in 82 cases, little in 121 cases, very in 66 cases. In 26.4% (99 cases) the symptom did not bother them, while 34 children (9.1 %) did not respond. As to whether children were worried about their noise: not at all in 198 cases (53%); slightly in 44 cases (12%), sometimes in 114 cases (30%), more severely in 18 cases (5%). Tinnitus was reported as bilateral in 156 cases (41.8%), unilateral in 141 cases (37.7%: 16.3 % left, 21.1% right), in the head in 69 cases (18.4%), and undefined laterality in 8 cases (2.1 %). It was described as intermittent in 12.8% of cases (47 children) and continuous in the remaining cases (327 children). The intermittent type was referred to as being present most of the time in 70% of the children (33 cases), and some of the time in the remaining cases. The pitch described was low in 197 children (52.6%), high in 162 children (43.3%), undefined in 146 cases (39% ). A more detailed description of the noises heard in regards to their tinnitus is shown in Table 1. The level of the tinnitus was reported as being loud in 130 subjects (34.7%) and low in 243 cases (64.9%).
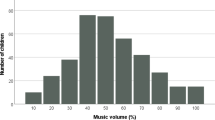
Tinnitus measurements were obtained and reproducible in all patients older than 8 years (341 cases). Below this age, the tinnitus tests showed non-reproducible results. In Fig. 2, a detailed summary of the loudness percentage distribution as pertains to intervals of 3 dB from 0 to 15 dB and values >15 dB is depicted. Figure 3 shows the frequency distribution. The kind of perception of tinnitus (low, medium and high) for children presenting with a loudness of <10 dB, between 10 and 15 dB and >15 dB respectively, is reported in Fig. 4. Figure 5 shows the masking level in patients presenting with a loudness <10 dB or >10 dB.The values of the residual inhibition in the two groups of subjects are reported in Fig. 6.

Percentage distribution as for tinnitus loudness levels expressed in dB

Percentage distribution as for tinnitus frequencies ranges expressed in Hz

Comparison between tinnitus intensity denounced by the patient and loudness values obtained by tinnitus measurement

Percentage distribution of masking levels, expressed in dB, concerning the two groups of patients differentiated as for loudness

Percentage distribution regarding residual inhibition duration, expressed in seconds
Discussion
The data obtained in this study show that a considerable number of children report tinnitus and confirm, in agreement with all authors, that children with tinnitus rarely complain spontaneously of it, but are able to describe it when questioned. The total percentage of children with tinnitus rises from 6.5% (tinnitus reported spontaneously), to 34% when children are specifically questioned.
Most children, more than 50%, have normal hearing; in those with hearing impairment, no particular type or severity of hearing loss has been found. Analogous results by Martin and Snashall are reported. Tinnitus without hearing loss has been described in 31 children studied by Rosanowski while Aust and Holgers found a prevalence of tinnitus in subjects with normal hearing between 6 and 36% and much higher, between 23 and 64%, in subjects with hearing loss [1, 4, 5, 10].
A past history of middle-ear pathology in our population of children was reported in 31.6% of cases and did not seem to be a significant factor in the genesis of children’s tinnitus as reported by Viani, Martin and Snashall, and Mills et al. As to the incidence of tinnitus, they found no statistical difference between the group of children with no history of middle-ear disease and the group of children who had middle-ear disease [5, 7, 12]. All children were able to give a description of their noises which showed a wide range, similar to other studies in adults [6, 11]. The most common description being “ringing” and “buzzing”.
Only in a few cases is tinnitus described as intermittent, while in most cases it is referred to as continuous. There is a correspondence between the percentage of children with normal hearing and tinnitus described as continuous and the percentage of children with hearing loss and tinnitus reported as intermittent. This finding supports previous studies in which intermittent tinnitus was usually associated with a hearing loss and constant tinnitus was usually associated with normal hearing [3, 5, 9, 12].
In contrast with the data reported by Mills and Cherry and by Mills at al. and in agreement with those reported by Martin and Snashall, only a low percentage of children with tinnitus reported that it does not bother them. Nevertheless, the majority of our children report that the symptom does not worry them [5, 7, 8]. The subjective judgement concerning one’s own tinnitus intensity rated low for over half of the cases.
Matched loudness values showed a rather homogeneous distribution for levels between 0 and 12 dB and for those over 12 dB, even if the highest percentage wass found to be between 4 and 6 dB for low intensity levels. Contrary to the data obtained by Savastano in an adult population, in children there is a correspondence between the judgement of their own tinnitus intensity and the loudness values reported. As a matter of fact, in most cases, the children with a loudness higher than 10 dB report a high intensity and those with lower loudness report a low intensity [11]. High frequencies resulting from the pitch match procedure were, as in adults, those between 0 and 1,000 Hz and, in lower percentage, those between 1,000 and 3,000 Hz and those at 8,000 Hz.
There is a correspondence between the loudness level and masking level. In most children with loudness <10 dB, the necessary masking level is limited to between 0 and 30 dB, while in most subjects of the second group (>10 dB), the masking level must be between 30 and 60 dB. In only a few cases was higher masking intensity required. A total residual inhibition over 60 s in a low percentage of cases was obtained both in the first and second group. A total inhibition <60 s or a partial inhibition in an analogous percentage for the second group was reached, while a total inhibition <60 s for the majority of children with lower loudness was obtained.
Conclusion
Tinnitus is not an uncommon symptom in the pediatric population and, despite its incidence, it is still an unrecognized problem, particularly in normal hearing children. Children rarely spontaneously complain of tinnitus but they report it and are able to describe it when they are directly asked about the symptom. Even if there is a lack of complaint, the fact that a clear description is always available indicates that tinnitus is a real entity in children.
The present study demonstrates that the application in infancy of a specific protocol of study provides the possibility of discovering the presence of tinnitus and obtaining specific and detailed information about it so as to minimize its damage. Moreover, for the first time, data regarding tinnitus measurement in childhood has been gathered. The complete protocol of study proposed by Savastano seems to be applicable in children above 8 years of age because, below this age, tinnitus measurements showed non-reproducible data.
References
Aust G (2002) Tinnitus in childhood. Int Tinnitus J 8:20–26
Baguley DM, Mc Ferran DJ (1999) Tinnitus in childhood. Int J Pediatr Otorhinolaryngol 49:99–105
Graham JM (1981) Paediatric tinnitus. J Laryngol Otol 95 Suppl 4:117–120
Holgers KM (2003) Tinnitus in 7-year-old children. Eur J Pediatr 162:276–278
Martin K, Snashall S (1994) Children presenting with tinnitus: a retrospective study. Br J Audiol 28:111–115
Meikle M, Walsh T (1984) Characteristics of tinnitus and related observations in over 1800 tinnitus patients. J laryngol Otol Suppl 9:17–21
Mills RP, Cherry JR (1984) Subjective tinnitus in children with otological disorders. Int J Pediatr Otorhinolaryngol 7:21–27
Mills RP, Albert DM, Brain CE (1986) Tinnitus in childhood. Clin Otolaryngol Allied Sci 11:431–434
Nodar RH (1984) Pediatric tinnitus. J Laryngol Otol 98 Suppl 9:234–235
Rosanowski F, Hoppe U, Proschel U, Eysholdt U (1997) Chronic tinnitus in children and adolescents. HNO 45:927–932
Savastano M (2002) A protocol of study for tinnitus in childhood. Int Pediatr Otorhinolaryngology 64:23–27
Viani LG (1989) Tinnitus in children with hearing loss. J Laryngol Otol 103:1142–1145
Acknowledgements
I would like to thank the consultants of ENT and pediatric medical offices of Cesena for allowing us to include their patients in this study. Dr. Carla Mucignat and Dr.Aram Megighian are thanked for the statistical analysis.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Savastano, M. Characteristics of tinnitus in childhood. Eur J Pediatr 166, 797–801 (2007). https://doi.org/10.1007/s00431-006-0320-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00431-006-0320-z