
Abstract
Kaposiform haemangioendothelioma (KHE) is a rare, locally aggressive vascular spindle cell proliferation, with resemblance to Kaposi’s sarcoma. This tumour usually occurs in skin and retroperitoneum of infants and young children and is often complicated by the Kasabach–Merritt phenomenon (KMP). A 3-year-old boy presented with a right submandibular swelling due to lymphadenopathies, a violaceous skin lesion at the left commissure of the lips and an ill-defined lesion in the right thyroid lobe. There were some signs of KMP. Histological examination revealed a typical infiltrative multilobular spindle cell proliferation with slit-like vascular spaces in these three localisations. Immunohistochemical stains showed positivity for CD34 and CD31 and many alpha-smooth muscle actin-positive spindle cells around the vascular spaces. There was no Herpes virus type 8 expression. The presented case is unique in two ways. First, thyroid involvement of KHE has never been described in the literature until now. Secondly, and most remarkably, the multifocal presentation in three anatomically distinct and separated localisations is extremely unusual.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Kaposiform haemangioendothelioma (KHE) is defined as a locally aggressive vascular neoplasm, characterised by a predominantly Kaposi sarcoma-like fascicular spindle cell growth pattern [17]. The tumour usually occurs in the skin [3, 7, 8, 11, 18, 20] and retroperitoneum [1, 9, 11, 16, 20] of infants and young children, but some adult cases have been described [5, 10]. KHE is often complicated by Kasabach–Merritt phenomenon (KMP), a condition of severe thrombocytopenia and consumptive coagulopathy [1–3, 6, 7, 11, 14, 16, 18–20]. Some cases of KHE are associated with lymphangiomatosis [7, 20]. Unlike juvenile haemangioma, KHE shows no tendency for spontaneous regression [7, 8]. Regional lymph node metastasis is rare, but distant metastasis has not been reported yet [7]. Mortality is mostly due to KMP with life-threatening haemorrhage [7, 14]. We recently encountered a case of KHE with a multifocal presentation and infiltration into the thyroid gland, a hitherto undescribed phenomenon.
Clinical history
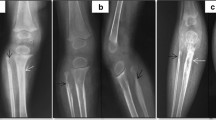
A 3-year-old boy presented with three episodes of fever and a right submandibular swelling of 3 cm in diameter, which was due to painless, but firm lymphadenopathies. Since there was no regression of the adenopathies, an excisional biopsy of a right neck lymph node was taken 4 months after the first consultation. Afterwards, the boy was referred to our center. He was in good general condition. Besides the submandibular lymphadenopathies, clinical examination also revealed a slightly elevated violaceous skin lesion as big as a rice-grain, situated left laterally of the mouth (Fig. 1a). There was no trombocytopenia, but still an elevation of the D-dimer level (2,007 μg/l) (normal values 0–500 μg/l), thyroglobulin (43.5 μg/l ) (normal values 0.0–25.0) and LDH (625 U/l) (normal values 240–480 U/l). Imaging revealed a prominent submandibular lymph node group and adenopathies along the right internal jugular vein (Fig. 1b). Furthermore, a lesion in the right thyroid lobe was seen, but could not further be specified on CT scan. Because of the presence of multiple lesions and the possibility of malignancy, a right hemithyroidectomy and a right lymph node dissection of levels I to IV was performed. Preoperatively, there was no connection between the thyroid lesion and the enlarged lymph nodes. During the same surgery, the skin lesion was excised. After the operation, there was a normalisation of the D-dimers (340 μg/l).

a A violaceous skin lesion at the left commissure of the lips. b CT scan: a prominent submandibular lymph node group at the right side
Materials and methods
The right thyroid lobe, the right neck dissection specimen and the skin lesion were received fresh. A small part of the lesion in the thyroid and the lymph nodes was snap-frozen in liquid-nitrogen-cooled isopentane. The rest of the specimens were fixed in 6% formalin and processed to paraffin. Five-micrometer thick tissue sections were subjected to haematoxylin and eosin. Immunohistochemical studies were performed on formalin-fixed, paraffin-embedded tissue, using a three-step indirect peroxidase complex method. The following antibodies were used: CD31 (1:50 dilution, monoclonal, Dako, Glostrup, Denmark), CD34 (1:10 dilution, monoclonal, Becton Dickinson, San Jose, USA), alfa-SMA (1:100 dilution, monoclonal, Dako, Glostrup, Denmark), HHV-8 (1:20 dilution, Novocastra, Newcastle, UK).
Pathological findings
The right thyroid lobe, measuring 2.2×1.5×1 cm, contained an ill-defined lesion of 1.3×0.9×1 cm. The right neck dissection specimen consisted of enlarged lymph nodes along the right jugular vein and next to the right submandibular gland, which was not infiltrated. The skin biopsy measured 0.5×0.5×0.7 cm.
Histopathological examination of the three resected specimens showed the same picture. The tumour was characterised by an infiltrative multilobular spindle cell proliferation. The infiltrative growth pattern caused destruction of the thyroid parenchyma (Fig. 2a) and the lymph node parenchyma (Fig. 2b). The skin biopsy showed that the tumour was situated in the deeper part of the dermis and in the upper part of the subcutis (Fig. 2c). The tumour consisted of nodules of compact spindle cell fascicles with hardly recognisable interspersed vascular spaces. Thin-walled dilated and probably lymphatic vessels were seen in-between and around the nodules (Fig. 3). The spindle cells did not show cytological atypia or nuclear pleomorphism. Mitotic activity was inconspicuous. Convincing microthrombi were very rare, as well as hyaline globules.

a A spindle cell proliferation with destructive infiltration of the thyroid (hematoxylin-eosin stain ×100). b A vascular spindle cell proliferation involving a lymph node (hematoxylin-eosin stain ×100). c A multilobular spindle cell proliferation in dermis and subcutis (hematoxylin-eosin stain ×50)

Thyroid: a dilated thin-walled vessel encircling a tumour nodule (hematoxylin-eosin stain ×100)
The tumour showed strong positivity for CD34 (Fig. 4) and CD31. Many SMA-positive spindle cells, presumably pericytes, were present around the vascular spaces. A HHV-8 stain was negative.

Thyroid: an infiltrative CD34-positive proliferation between the thyroid follicles (×100)
Based on these morphological and immunohistochemical findings, a diagnosis of KHE was made.
Discussion
The term ‘Kaposiform haemangioendothelioma’ was introduced in 1993 by Zukerberg et al. Ever since, fewer than 100 cases have been reported in the literature [1–11, 14–16, 18–20].
KHE usually occurs in early childhood, and often in the first decade of life. KHE mostly involves the skin and the retroperitoneum. The tumour occurs less commonly in the head and neck region [2, 5–7, 15, 20] and in the deep soft tissue of the extremities and the trunk [7, 20]. Rare cases have been described in the mediastinum [7], thymus (one case) [19] and scrotum (one case) [7]. To our knowledge, we present in this paper the first case involving the thyroid.
KHE is often associated with KMP. In our case, there was an elevation of D-dimers, an important marker of consumptive coagulopathy. Therefore, it seems likely that this child showed some evidence of KMP, although platelet count was normal and fibrin thrombi were rare. Yet the recent study of Lyons et al. mentioned that the number of platelet thrombi does not correlate with the presence of KMP [7]. Moreover, normalisation of D-dimers after resection of the lesions proves that the trigger for consumptive coagulopathy has been removed. This trigger has been thought to be related to unique architectural features that favour turbulent blood flow and platelet activation [7]. Absence or presence of KMP is an important prognostic factor, since life-threatening haemorrhage can cause mortality.
Our case illustrates both the nodules of compressed vessels and the ectatic vascular component of KHE. This biphasic pattern has been described before in the literature [1, 7, 9, 11, 15, 20].
In contrast to juvenile haemangioma, KHE shows no tendency to involute. KHE is a locally aggressive tumour, and distant metastasis is not described to date. When reviewing the literature, we found one case of congenital cutaneous multifocal haemangioendothelioma [4]. This report mentions the case of a newborn having multiple cutaneous lesions with the histopathological picture of KHE. All these lesions were confined to the skin. In the present case, we describe KHE in three anatomically distinct and separate lesions. Moreover, we do not have evidence of congenital disease.
Theoretically, one could consider metastatic and aggressive disease because of the separate locations. However, in our case, just as in all earlier described KHEs, there were no histological features of malignancy. In addition, some benign vascular lesions, like the spindle cell haemangioma, can give rise to multiple lesions in the same general area [13]. Finally, another benign vascular tumor, the retiform haemangioendothelioma, occasionally metastasises to the lymph nodes without systemic spread and without aggressive behaviour [12]. In our case, multifocal presentation seems more likely than metastasis from the right thyroid lobe to contralateral lymph nodes only and not to ipsilateral lymph nodes. Obviously, the patient will be followed very closely and only a long-term follow-up will be to disclose the true biologic behaviour. At present, it seems that KHE can be added to the list of vascular tumours with an occasional multifocal presentation.
References
Brasanac D, Janic D, Boricic I, Jovanovic N, Dokmanovic L (2003) Retroperitoneal kaposiform hemangioendothelioma with tufted angioma-like features in an infant with Kasabach–Merritt syndrome. Pathol Int 53:627–631
Chung MT, Chen CH, Chiu CH, Yang CP, Hsueh C, Jaing TH (2003) Successful nonoperative therapy for Kaposiform hemangioendothelioma involving the neck: report of 1 case. Otolaryngol Head Neck Surg 129:605–607
Fukunaga M, Ushigome S, Ishikawa E (1996) Kaposiform haemangioendothelioma associated with Kasabach–Merritt syndrome. Histopathology 28:281–284
Gianotti R, Gelmetti C, Alessi E (1999) Congenital cutaneous multifocal kaposiform hemangioendothelioma. Am J Dermatopathol 21:557–561
Hardisson D, Prim MP, De Diego JI, Patron M, Escribano A, Rabanal I (2002) Kaposiform hemangioendothelioma of the external auditory canal in an adult. Head Neck 24:614–617
Lalaji TA, Haller JO, Burgess RJ (2001) A case of head and neck kaposiform hemangioendothelioma simulating a malignancy on imaging. Pediatr Radiol 31:876–878
Lyons LL, North PE, Mac-Moune Lai F, Stoler MH, Folpe AL, Weiss SW (2004) Kaposiform hemangioendothelioma: a study of 33 cases emphasizing its pathologic, immunophenotypic, and biologic uniqueness from juvenile hemangioma. Am J Surg Pathol 28:559–568
Mac-Moune Lai F, To KF, Choi PC, Leung PC, Kumta SM, Yuen PP, Lam WY, Cheung AN, Allen PW (2001) Kaposiform hemangioendothelioma: five patients with cutaneous lesion and long follow-up. Mod Path 14:1087–1092
Martinez AE, Robinson MJ, Alexis JB (2004) Kaposiform hemangioendothelioma associated with nonimmune fetal hydrops. Arch Pathol Lab Med 128:678–681
Mentzel T, Mazzoleni G, Dei Tos AP, Fletcher CD (1997) Kaposiform hemangioendothelioma in adults. Clinicopathologic and immunohistochemical analysis of three cases. Am J Clin Pathol 108:450–455
Niedt GW, Greco MA, Wieczorek R, Blanc WA, Knowles DM (1989) Hemangioma with Kaposi’s sarcoma-like features: report of two cases. Pediatr Pathol 9:567–575
O’Hara CD, Nascimento AG (2003) Endothelial lesions of soft tissues: a review of reactive and neoplastic entities with emphasis on low-grade malignant (“borderline”) vascular tumors. Adv Anat Pathol 10:69–87
Perkins P, Weiss SW (1996) Spindle cell hemangioendothelioma: An analysis of 78 cases with reassessment of its pathogenesis and biologic behavior. Am J Surg Pathol 20:1196–1204
Sarkar M, Mulliken JB, Kozakewich HP, Robertson RL, Burrows PE (1997) Thrombocytopenic coagulopathy (Kasabach–Merritt phenomenon) is associated with Kaposiform hemangioendothelioma and not with common infantile hemangioma. Plast Reconstr Surg 100:1377–1386
Tello MA, Shields G, Gadre SA, Ryan M (2004) Pathology quiz case 2. Diagnosis: Kaposiform hemangioendothelioma (KHE). Arch Otolaryngol Head Neck Surg 130:991 Diag 993–994
Tsang WY, Chan JK (1991) Kaposi-like infantile hemangioendothelioma. A distinctive vascular neoplasm of the retroperitoneum. Am J Surg Pathol 15:982–989
Tsang WY (2002) Kaposiform haemangioendothelioma. In: Fletcher CDM, Unni KK, Mertens F (eds) World Health Organization classification of tumours. Pathology and genetics of tumours of soft tissue and bone. IARC, Lyon, pp 163–164
Vin-Christian K, McCalmont TH, Frieden IJ (1997) Kaposiform hemangioendothelioma. An aggressive, locally invasive vascular tumor that can mimic hemangioma of infancy. Arch Dermatol 133:1573–1578
Wilken JJ, Meier FA, Kornstein MJ (2000) Kaposiform hemangioendothelioma of the thymus. Arch Pathol Lab Med 124:1542–1544
Zukerberg LR, Nickoloff BJ, Weiss SW (1993) Kaposiform hemangioendothelioma of infancy and childhood. An aggressive neoplasm associated with Kasabach–Merritt syndrome and lymphangiomatosis. Am J Surg Pathol 17:321–328
Acknowledgement
We are grateful to Professor C. D. M. Fletcher, Harvard Medical School, Boston, for confirming the diagnosis.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Deraedt, K., Vander Poorten, V., Van Geet, C. et al. Multifocal kaposiform haemangioendothelioma. Virchows Arch 448, 843–846 (2006). https://doi.org/10.1007/s00428-006-0177-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00428-006-0177-6