
Abstract
Anaplastic carcinoma of the thyroid gland (ACT) is a highly malignant tumor that is almost invariably associated with a fatal outcome. It demonstrates a variety of peculiar histological features, with squamoid, giant cell and spindle cell growth patterns. The spindle cell variant of ACT is usually indistinguishable from a true sarcoma and it can simulate fibrosarcoma, malignant fibrous histiocytoma (MFH), hemangiopericytoma and angiosarcoma or rhabdomyosarcoma. Although a rhabdomyosarcomatous appearance has sometimes been mentioned in the literature, true skeletal muscle differentiation has never been consistently proved. We report two cases of ACT with rhabdomyosarcomatous differentiation, as demonstrated by means of immunohistochemistry and electron microscopy. Both cases disclosed a very similar histological appearance, with a main population of small, pleomorphic, round-to-oval cells arranged in a storiform pattern, admixed with scattered pleomorphic giant cells, an image similar to that of the usual type of MFH. Stains for epithelial markers showed only few, scattered, weakly positive cells. Thyroglobulin and calcitonin were negative in tumor cells in both cases. On the contrary, positivity to vimentin was strong and generalized. Immunomarkers of muscular differentiation showed a consistent positivity. At the ultrastructural level, the cells disclosed the same spindle and pleomorphic morphology, with large, bizarre nuclei and cytoplasm with abundant mitochondria, rough endoplasmic reticulum, secretory granules and lipid droplets. There were also cells with wide cytoplasm filled with filamentous material, either of actin or myosin, as well as Z-band material. In conclusion, the cases reported here show a clear-cut rhabdomyosarcomatous differentiation of ACT, confirmed both immunohistochemically and ultrastructurally, a feature not previously reported in the literature. These findings may contribute to the broadening of the differentiation spectrum of this unusual neoplasm.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Anaplastic (undifferentiated) carcinoma of the thyroid gland (ACT) is a highly malignant tumor that is almost invariably associated with a fatal outcome [3, 7, 16, 17, 26]. It demonstrates a variety of peculiar histological features, with squamoid, giant cell and spindle cell growth patterns [1, 3].
From the morphological point of view, the spindle cell variant of ACT is indistinguishable from a true sarcoma. Thus, ACT can simulate fibrosarcoma, malignant fibrous histiocytoma (MFH), hemangiopericytoma, angiosarcoma or rhabdomyosarcoma [8, 21, 22]. However, the presence of recognizable epithelial foci, immunohistochemical positivity for keratins and the ultrastructural presence of desmosomes and microvilli favor the diagnosis of an epithelial malignancy [1, 2, 10, 12, 14, 18, 19, 23].
Although a rhabdomyosarcomatous appearance has sometimes been mentioned in the literature [3, 17], true skeletal muscle differentiation has never been consistently proved. We report the first two cases of ACT with rhabdomyosarcomatous differentiation, as demonstrated by means of immunohistochemistry and electron microscopy.
Case reports
Case 1
A 59-year-old man with a personal history of heavy smoking and alcohol abuse was admitted to hospital because of a rapidly growing neck mass, which had developed during the previous 3 months and was accompanied by dysphony and weight loss. Physical examination disclosed paralysis of the left recurrent nerve. A computerized axial tomography was performed, revealing the existence of a thyroid tumor invading the retrotracheal region. A right hemithyroidectomy was carried out, together with partial esophageal resection and pharingo-jejunostomy. Following surgery, the patient received radiation therapy (linear accelerator 18 Mv photons). A later computerized axial tomography demonstrated bilateral pulmonary metastases. The patient then received chemotherapy, but he developed a progressive respiratory distress and died 15 months after diagnosis and surgery. Autopsy was not allowed.
Case 2
A 62-year-old man with no interesting clinical history presented a rapidly enlarging mass in the left anterior cervical region. On physical examination, the tumor was nut-sized and apparently confined within the thyroid. A few days later, the patient suffered a sudden growth in the anterior region of his neck, together with severe hoarseness. A fine-needle aspiration biopsy was performed, followed by a total thyroidectomy and tracheostomy. The early postoperative period was satisfactory, with no remarkable event. After surgery, I131 gammagraphy was carried out, demonstrating cervical thyroid remnants. Chest radiography, hepatic ultrasonography and bone gammagraphy were negative. The patient was initially given radiotherapy, but after a few weeks he was lost for treatment and follow-up.
Materials and methods
After fixation of the surgical specimens in 10% formaldehyde solution, tissue samples were taken from different areas and embedded in paraffin. Multiple 3-µm sections were obtained by means of a standard microtome and then stained with haematoxylin and eosin. Immunohistochemistry was performed using paraffin-embedded material and the avidinbiotin-peroxidase technique. The antisera employed and their working dilution are shown in Table 1.
For electron microscopy examination, fresh specimens were fixed in 2.5% glutaraldehyde solution (buffered pH 7.4) and postfixed in 2% osmium tetroxide. After dehydration, the tissue blocks were embedded in Epon 812 (TAAB Lab, England). Ultrathin sections were stained with uranyl acetate and lead citrate, and examined under a Jeol-Jem 1010 electron microscope (Tokyo, Japan).
Results
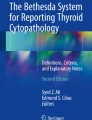
Both cases disclosed a very similar histological appearance, with a large population of small, pleomorphic, round-to-oval cells arranged in a storiform pattern, admixed with scattered pleomorphic giant cells, an image similar to that of the usual type of MFH. In some areas, the small cells adopted a spindle cell configuration, with fascicles and bundles reminiscent of fibrosarcoma (Fig. 1a).

Histological appearance and immunomarkers of muscular differentiation. a Round and oval cells in storiform pattern (case 1). b Pleomorphic cell population with small and giant cells (case 2). Muscle-specific actin (c; case 1), desmin (d; case 2), myogenin (e; case 1), myogenin (f; case 2), MyoD1 (g; case 1), smooth muscle actin (h; case 2)
The small cells revealed a scant, pale cytoplasm, which was occasionally more prominent, giving the cell a rhabdomyoblast-like appearance. On the cell, however, no cross-striations were seen. The nuclei were irregular and showed prominent nucleoli. The pleomorphic giant cells were mono- and multinucleated, with bizarre, hyperchromatic nuclei and a wide, acidophilic, sometimes slightly granular cytoplasm. They were more abundant in case 2 (Fig. 1b). Atypical mitotic figures were frequent, reaching 18 mitoses per 10 high power fields (HPF) in case 1. Necrotic areas were prominent in both cases, often surrounded by a palisading of tumor cells. Both tumors showed a marked vascularization, the vessels sometimes adopting a branched pattern, similar to that of hemangiopericytoma. Pseudovascular channels, caused by artifactual retraction of tumor cells, were also seen in some areas. A diagnosis of anaplastic carcinoma was given in each case.
Both tumors grew in a markedly aggressive manner, substituting and entrapping the follicular parenchyma of the thyroid and invading the neighboring cervical structures, spreading into the skeletal muscles of the neck. Case 2 reached the esophageal wall, the tumor ulcerating the mucosa and forming an exophitically protruding mass.
Immunohistochemical results for epithelial markers (cytokeratin AE1/AE3 and CAM 5.2 cocktails, EMA) showed only few, scattered, weakly positive cells. The number of cells stained was not significantly different with any of these markers, which only showed strong reactivity in the entrapped thyroid follicles. Thyroglobulin and calcitonin were negative in tumor cells in both cases.
However, positivity to vimentin was strong and generalized. Immunomarkers of muscular differentiation showed a consistent positivity (Fig. 1c–h): muscle-specific actin (HHF35) was expressed by a large number of cells in case 1, in the form of islets of positive cells; whereas it reacted only focally in case 2. In contrast, desmin was more extensively expressed in case 2; myoglobin was widely positive in both cases; Myo-D1 showed clear nuclear positivity only in case 1 (staining less than 5% of tumor cells), with unspecific, scattered cytoplasmic reactivity in case 2; myogenin reacted against tumor cells in both cases, this reactivity being focal and more marked in case 1 (10–20% of tumor cells) than in case 2 (<5%); and, finally, smooth muscle actin was positive only in case 2, where it was expressed in a diffuse manner.
At the ultrastructural level, the cells disclosed the same spindle and pleomorphic morphology (Fig. 2c), with large, bizarre nuclei and cytoplasm with abundant mitochondria, rough endoplasmic reticulum and ribosomes, glycogen, lysosomes, secretory granules and lipid droplets (Fig. 2a). There were also cells with wide cytoplasm filled with filamentous material, either of actin (thin filaments) or myosin (thick filaments), as well as Z-band material (Fig. 2a, b). Rudimentary cell-to-cell junctions were found (Fig. 2c, inset).

Electron microscopic features. a Ultrastructural evidence of numerous organelles and myoblastic differentiation, thin filaments are placed randomly and with focal densities (inset; case 1). b Cross section showing thick and thin filaments, Z-band material and ribosomal complexes (case 2). c Tumor showing irregular cell size and nuclear shape with euchromatin, and isolated cell-to-cell junctions (inset; case 2)
Discussion
From the histological point of view, anaplastic thyroid tumors can resemble undifferentiated epithelial neoplasms or may be composed of spindle cells mimicking a sarcoma. The variety of peculiar histological features that characterize ACT has led to different morphological classifications, in which squamoid, giant cell and spindle cell growth patterns are the most accepted [3, 17, 26].
The spindle cell and pleomorphic variants of ACT are indistinguishable from a true sarcoma. In this sense, ACT has been repeatedly described as fibrosarcoma, malignant fibrous histiocytoma, hemangiopericytoma, angiosarcoma or rhabdomyosarcoma [1, 3, 7, 8, 16, 17, 21, 22, 26]. However, the evidence of epithelial differentiation on an immunohistochemical and/or ultrastructural basis favors the diagnosis of an epithelial neoplasm [10, 11, 12, 13, 14, 15, 17, 18]. On the contrary, true sarcomas of the thyroid gland seem to be exceedingly unusual [3, 7, 16, 17, 26]. Altogether, this distinction appears rather academic, given the fact that both entities share a common clinical presentation and an almost invariably fatal outcome.
Despite the frequent notations of a rhabdomyosarcomatous appearance, no evidence of muscular differentiation has been consistently demonstrated. Some authors regard the pleomorphic variant of ACT as a mimicker of rhabdomyosarcoma, given the presence of spindle and pleomorphic cells arranged in a storiform pattern, often showing a wide, acidophilic cytoplasm [3, 17]. Nevertheless, neither immunoreactivity against muscular markers nor ultrastructural evidence of myogenic structures have been directly associated with this particular histological pattern of ACT. Isolated data of desmin expression [16] and ultrastructural presence of actin filaments [3] can be found in the literature, but they have not deserved any specific mention as indicative of skeletal or smooth muscle differentiation.
The cases reported here clearly showed skeletal muscle differentiation from the immunohistochemical point of view. First, the tumor cells of both cases reacted against muscle-specific actin and desmin, which are the most universally employed markers of myogenic commitment [20, 24, 25, 27, 28]. Desmin was more extensively expressed in case 2, but there was no doubt of its positivity in case 1, where well-defined islets of positive cells were seen. It has been shown, however, that actin and desmin can be expressed in different degrees by a variety of benign and malignant soft tissue tumors, thus making these two proteins not specific to muscle differentiation [24, 25]. Besides, muscle-specific actin can be seen (to a variable extent) in smooth muscle tumors—i.e., leyomiosarcoma, a malignancy also occurring in the thyroid gland [5, 13, 15, 29].
We also performed immunostaining against three specific skeletal muscle markers: myoglobin, Myo-D1 and myogenin. Care must be taken with the interpretation of the results using these antibodies, as has been frequently reported in the literature [4, 9]. This issue notwithstanding, we were able to demonstrate positivity to all three in the two cases studied. Myoglobin stained uniformly, clearly revealing the cytoplasms of tumor cells over a tea-colored background, a stain not attributable only to an edge-effect of the technique. Myo-D1 and myogenin are two myogenic transcriptional regulators, which appear to play a critical role in the commitment of mesenchymal progenitor cells to the myogenic cell line. These proteins are found in normal fetal muscle and are thought to be absent in adult muscle [6]. We found nuclear positivity against myogenin in both cases, although it was limited to a relatively small percentage of cells, which ranged from 5% to 20%. This variability has already been reported for the different subtypes of rhabdomyosarcoma, but it does not question the specificity of myogenin [4].
Ultrastructurally, there was a clear-cut skeletal muscle differentiation in both cases, defined by the presence of myofilaments and Z-bands in the cytoplasm of rhabdomyoblast-like tumor cells. Such definite structures have not been reported to date in ACT, despite an isolated mention to the existence of actin filaments [3]. Moreover, the cases reported here showed the mature form of myofilament disposition, i.e., thin filaments of actin surrounding a thick myosin filament. No ultrastructural features of smooth muscle differentiation were seen in any case, thus confirming the immunohistochemical expression of myogenic markers as corresponding to skeletal muscle.
The scarcely expressed epithelial phenotype finds correlation both immunohistochemically and ultrastructurally. The expression of cytokeratins was weak and focal, but mostly confined to rhabdomyoblast-like tumor cells. This feature has already been reported in ACT [19], and seems to correspond with the scarcity of epithelial differentiation as revealed by electron microscopy. In our cases, we could only find a few, rather rudimentary, desmosomes between some tumor cells, in the context of a loosely cohesive neoplastic population, most if not all undifferentiated carcinoma.
In conclusion, cases reported here show a clear-cut rhabdomyosarcomatous differentiation of ACT, confirmed both imunohistochemically and ultrastructurally, a feature not previously reported in the literature. These findings may contribute to the expansion of the spectrum of differentiation for this unusual neoplasm.
References
Aldinger KA, Saaman NA, Ibáñez M (1978) Anaplastic carcinoma of the thyroid: a review of 84 cases of spindle and giant cell carcinoma. Cancer 41:2267–2275
Beltrami CA, Criante P, Di Loreto C (1989) Immunocytochemistry of anaplastic carcinoma of thyroid gland. Appl Pathol 7:122–133
Carcangiu ML, Steeper T, Zampi G, Rosai J (1984) Anaplastic thyroid carcinoma. A study of 70 cases. Am J Clin Pathol 83:135–158
Cessna MH, Zhou H, Perkins SL, Tripp SR, Layfield L, Daines C, Coffin CM (2001) Are myogenin and MyoD1 expression specific for rhabdomyosarcoma? A study of 150 cases, with emphasis on spindle cell mimics. Am J Surg Pathol 25:1150–1157
Chetty R, Clark SP, Dowling JP (1993) Leyomyosarcoma of the thyroid: immunohistochemical and ultrastructural study. Pathology 25:203–205
Dias P, Dilling M, Houghton P (1994) The molecular basis of skeletal muscle differentiation. Semin Diagn Pathol 11:3–14
Donnell CA, Pollock WJ, Sybers WA (1987) Thyroid carcinosarcoma. Arch Pathol Lab Med 11:1169–1172
Eusebi V, Carcangiu ML, Dina R (1990) Keratin-positive epithelioid angiosarcoma of the thyroid: a report of four cases. Am J Surg Pathol 14:737–747
Furlong MA, Mentzel T, Fanburg-Smith JC (2001) Pleomorphic rhabdomyosarcoma in adults: a clinicopathologic study of 38 cases with emphasis on morphologic variants and recent skeletal muscle-specific markers. Mod Pathol 14:595–603
Graham H, Daniel C (1974) Ultrastructure of an anaplastic carcinoma of the thyroid. Am J Clin Pathol 61:690–696
Hofstädter F (1980) Electron microscopic investigations about the differentiation of thyroid carcinoma. Pathol Res Pract 169:304–322
Hurlimann J, Gardiol D, Scazziga B (1987) Immunohistology of anaplastic thyroid carcinoma. A study of 43 cases. Histopathol 11:567–580
Iida Y, Katoh R, Yoshioka M, Oyama T, Kawaoi A (1993) Primary leyomyosarcoma of the thyroid gland. Acta Pathol Jpn 43:71–75
Jao W, Gould VE (1975) Ultrastructure of anaplastic (spindle and giant cell) carcinoma of the thyroid. Cancer 35:1280–1292
Kawahara E, Nakanishi I, Terahata S, Ikegaki S (1988) Leyomyosarcoma of the thyroid gland. A case report with comparative study of five cases of anaplastic carcinoma. Cancer 62:2558–2563
Lampertico P (1993) Anaplastic (sarcomatoid) carcinoma of the thyroid gland. Semin Diagn Pathol 10:159–168
LiVolsi VA (ed) (1990) Surgical pathology of the thyroid. In: Major problems in pathology, vol. 22. Saunders, Philadelphia, PA
LiVolsi VA, Brooks JJ, Arendash-Durand B (1987) Anaplastic thyroid tumors. Immunohistology. Am J Clin Pathol 87:434–442
Miettinen M, Franssila KO (2000) Variable expression of keratins and nearly uniform lack of thyroid transcription factor 1 in thyroid anaplastic carcinoma. Hum Pathol 31:1139–1145
Miettinen M, Lehto VP, Virtanen I (1984) Antibodies to intermediate filament proteins in the diagnosis and classification of human tumors. Ultrastruct Pathol 7:83–107
Mills SE, Stallings RG, Austin MB (1986) Angiomatoid carcinoma of the thyroid gland. Am J Clin Pathol 86:674–678
Ordóñez NG, Hickey RC, Samaan NA (1987) Anaplastic thyroid carcinoma. Cancer Bulletin 39:318–323
Ordóñez NG, El-Naggar AK, Hickey RC, Samaan NA (1991) Anaplastic thyroid carcinoma. Imunocytochemical study of 32 cases. Am J Clin Pathol 96:15–24
Rangdaeng S, Truong LD (1991) Comparative immunohistochemical staining for desmin and muscle-specific actin. A study of 576 cases. Am J Clin Pathol 96:32–45
Roholl PJ, Elbers HR, Prinsen R, Claessens JA, van Unnik JA (1990) Distribution of actin isoforms in sarcomas: an immunohistochemical study. Hum Pathol 21:1269–1274
Rosai J, Carcangiu ML, DeLellis RA (1992). Tumors of the thyroid gland (Atlas of tumor pathology). Armed Forces Institute of Pathology, Washington DC
Schürch W, Skalli O, Seemayer TA, Gabbiani G (1987) Intermediate filament proteins and acti isoforms as markers for soft tissue tumor differentiation and origin. I. Smooth muscle tumors. Am J Pathol 128:91–103
Skalli O, Gabbiani G, Babai F, Seemayer TA, Pizzolato G, Schürch W (1988) Intermediate filament proteins and acti isoforms as markers for soft tissue tumor differentiation and origin. II. Rhabdomyosarcomas. Am J Pathol 130:515–531
Thompson LDR, Wenig BM, Adair CF, Shmookler BM, Heffess CS (1997) Primary smooth muscle tumors of the thyroid gland. Cancer 79:579–587
Acknowledgements
This work was supported by FIS grant 01/0673.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Carda, C., Ferrer, J., Vilanova, M. et al. Anaplastic carcinoma of the thyroid with rhabdomyosarcomatous differentiation: a report of two cases. Virchows Arch 446, 46–51 (2005). https://doi.org/10.1007/s00428-004-1123-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00428-004-1123-0