
Abstract
Purpose
Peritoneal surface malignancies (PSM) are commonly known to have a dismal prognosis. Over the past decades, novel techniques such as cytoreductive surgery (CRS), hyperthermic intraperitoneal chemotherapy (HIPEC), and pressurized intraperitoneal aerosol chemotherapy (PIPAC) have been introduced for the treatment of PSM which could improve the overall survival and quality of life of patients with PSM. The decision to proceed with CRS and HIPEC is often challenging due the complexity of the disease, the extent of the procedure, associated side effects, and potential risks. Here, we present our experience with CRS and HIPEC to add to the ongoing discussion about eligibility criteria, technical approach, and expected outcomes and contribute to the evolution of this powerful and promising tool in the multidisciplinary treatment of patients with primary and secondary PSM.
Methods
A single-center retrospective chart review was conducted and included a total of 40 patients treated with CRS and HIPEC from April 2020 to September 2022 at the University Hospital Münster Department of Surgery. All patients had histologically confirmed primary or secondary peritoneal malignancies of various primary origins.
Results
Our study included 22 patients with peritoneal metastases from gastric cancer (55%), 8 with pseudomyxoma peritonei (20%), 4 with mesothelioma of the peritoneum (10%), and 6 patients with PSM originating from other primary tumor locations. Median PCI at time of cytoreduction was 4 (0–25). Completeness of cytoreduction score was 0 in 37 patients (92.5%), 1 in two patients (5%), and 2 in one patient (2.5%). Median overall survival across all patients was 3.69 years.
Conclusion
Complete cytoreduction during CRS and HIPEC can be achieved for patients with low PCI, for patients with high PCI in low-grade malignancies, and even for patients with initially high PCI in high-grade malignancies following a significant reduction of cancer burden due to extensive preoperative treatment with PIPAC and systemic chemotherapy.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Peritoneal surface malignancies (PSM) can be categorized into primary and secondary peritoneal malignancies [1]. The majority of cases are secondary peritoneal metastases arising from advanced intraperitoneal cancers. The most common primaries forming peritoneal metastases include ovarian, gastric, and colorectal cancers with around 61%, 14%, and 8% of patients developing peritoneal metastases during the course of their disease respectively [2,3,4]. Rarer entities that can lead to peritoneal metastases are hepatobiliary, appendiceal, small-bowel, and endometrial cancers. In addition, certain extraperitoneal cancers, such as breast and lung cancer, have been shown to cause peritoneal metastases in about 1% of patients [5, 6].
Far less common are primary peritoneal malignancies such as primary peritoneal carcinoma and malignant peritoneal mesothelioma [7] with an incidence rate of below 1 per 100,000 persons per year [8, 9].
Pseudomyxoma peritonei represents a special case and originates from mucinous tumors within the peritoneal cavity. While there have been descriptions of various origins, most patients with pseudomyxoma peritonei have appendiceal neoplasms [10]. When the primary tumor ruptures, components of the tumor, such as cells and mucin, spread to the peritoneal cavity to form mucinous ascites and new neoplastic sites within the peritoneal cavity [11].
The treatment of peritoneal surface malignancies remains a challenge for clinicians worldwide. Over the last decades, efforts have been made to evaluate and advance existing and novel treatment strategies to improve the poor prognosis of patients with peritoneal surface malignancies. One of the newer therapeutic strategies for patients with peritoneal cancers is pressurized intraperitoneal aerosol chemotherapy (PIPAC) [12,13,14,15,16,17,18]. During the PIPAC procedure, laparoscopy is performed, biopsies are taken, and vaporized chemotherapeutic agents are delivered to the peritoneal cavity to target peritoneal metastases as well as primary peritoneal malignancies [19,20,21]. Similar to HIPEC, PIPAC aims to deliver the chemotherapeutic agent directly to the peritoneal implants in order to increase the locoregional drug concentration and to reduce systemic side effects as compared to standard intravenous chemotherapy. PIPAC was shown to be safe, well tolerated by patients, and effective at reducing peritoneal cancer burden for peritoneal cancers of various origins [14, 22,23,24]. However, impact on survival is still being evaluated and remains unclear.
To date, the only potentially curative option for treatment of peritoneal surface malignancies relies on cytoreductive surgery (CRS) [25]. The objective of the surgical technique is to achieve complete resection of all visible macroscopic disease [26]. This is often complemented by the application of locoregional chemotherapy to treat residual microscopic disease [27], commonly performed as hyperthermic intraperitoneal chemotherapy (HIPEC) to enhance the cytotoxicity of the chemotherapeutic agents [28]. The combination of cytoreductive surgery and intraperitoneal chemotherapy aims at the complete eradication of tumor lesions, since chemotherapeutic agents are able to penetrate any remaining microscopic disease [29]. If a complete cytoreduction is achieved, long-term survival is possible for select patients and tumor histologies [30,31,32,33,34,35]. CRS and HIPEC are extended procedures causing extensive tissue trauma and can result in severe—sometimes even life-threatening—side effects and significant morbidity [36]. Therefore, the decision to proceed to CRS and HIPEC is often challenging for both patients and providers. While CRS and HIPEC has become standard of care for a subset of patients with PSM, there is ongoing debate and evolution of various aspects, such as indications, eligibility criteria, and technical standards. Here, we present our experience with CRS and HIPEC at the University Hospital Münster in Germany to add to this discussion and further characterize the role of CRS and HIPEC as a powerful and promising tool in the multidisciplinary treatment approach for primary and secondary peritoneal malignancies.
Methods
Study design
A single-center retrospective chart review was conducted. The analysis included a total of 40 patients treated with CRS and HIPEC from April 2020 to September 2022 at the University Hospital Münster Department of Surgery, a tertiary care center in the northwest of Germany. Prior approval was obtained from the local ethics committee (Ethik-Kommission der Ärztekammer Westfalen-Lippe und Westfälischen Wilhelms-Universität, No. 2022–347-f-S). The study was performed in accordance with the ethical principles of the Declaration of Helsinki.
Study population
The algorithm to assess eligibility for CRS and HIPEC included histopathological assessment of biopsies from primary cancer and peritoneal metastases, diagnostic laparoscopy, and cross-sectional imaging. Several patients had undergone laparotomy at outside facilities which had led to an incidental diagnosis of peritoneal cancer. If all necessary information to confirm eligibility could be extracted from the records, diagnostic laparoscopy was omitted. All patients had histologically confirmed primary or secondary peritoneal malignancies of various primary origins. When patients met eligibility criteria for cytoreduction and HIPEC prior to pseudo-neoadjuvant chemotherapy, treatment response was assessed by cross-sectional imaging after completion of preoperative chemotherapy which was—in the absence of any signs for progression—directly followed by CRS and HIPEC without additional laparoscopy. Patients enrolled in our PIPAC program and patients who had received the entire preoperative treatment at an outside facility underwent laparoscopy prior to CRS-HIPEC to confirm eligibility. Treatment plans for all patients were discussed by a multidisciplinary tumor board, after careful review of the medical record, weighing risk factors and potential benefit from the procedure in comparison to other treatment options. The following data points were collected: age, gender, BMI, ECOG, date of primary tumor diagnosis, date of diagnosis of peritoneal metastasis, tumor histology, previous surgeries and/or chemotherapies, date and details of the CRS-HIPEC procedure (PCI, completeness of cytoreduction, performed resections, number of anastomoses, type and dosage of drugs, HIPEC temperature, and duration), postoperative complications, length of hospital stay, overall survival, and tumor versus non-tumor-related cause of death.
Procedures and follow-up
After approval by the tumor board, the planned procedure was discussed in detail with the patients and their relatives and informed consent was obtained. Cytoreductive surgery and HIPEC were performed in one setting under general anesthesia. To gain access to the abdominal cavity, a median laparotomy was performed and prior scars, if present, were excised. The umbilicus was excised in all patients and submitted as a specimen for histological assessment. The abdomen was thoroughly examined for suspicious lesions and the Peritoneal Cancer Index (PCI) according to Sugarbaker was calculated [37]. Presence and amount of ascites were documented. Adhesiolysis was performed as necessary. A complete peritonectomy was performed including the parietal, the subphrenic, and pelvic portions. Minor and major omentectomies were performed, Lig. teres hepatis and Lig. falciforme hepatis were excised. Bilateral ovariectomies were performed in all females. Only 5 of 22 female patients (22.7%) were premenopausal. Three of them had pelvic disease affecting both ovaries mandating bilateral ovariectomies. Two of them, both mesothelioma patients, had pelvic disease involving only one ovary. Both patients had been counseled preoperatively and decided to proceed with bilateral ovariectomies. Prophylactic simultaneous appendectomy and cholecystectomy were performed when organs were still present. An oncologic resection of the primary tumor was performed including regional lymphadenectomies. Frozen sections of resection margins were sent as necessary. Additional resections—en-bloc, if necessary—were performed based on the extent of the disease to achieve a complete cytoreduction. The degree of completeness of cytoreduction was noted. Reconstruction was performed, hemostasis was checked, and the abdomen was irrigated. Inflow and outflow drains, as well as temperature probes, were placed through the abdominal wall before closing fascia and skin. Two 36-Fr silicon drains served as inflow drains entering the abdominal cavity via the right abdominal wall, with one ending deep in the pelvis and one deep in the upper abdomen. Three 36-Fr silicon drains were positioned superficially underneath the abdominal wall exiting through the left abdominal wall and serving as outflow drains. One of the temperature probes was attached to the pelvic inflow drain to measure the inflow temperature, and the other temperature probe was attached to one of the outflow tubes to measure the outflow temperature. The abdomen was filled with normal saline to confirm that there was no leakage. Adjustments were made as necessary to achieve a tight seal. HIPEC was performed using a closed abdominal technique [29, 38,39,40]. For mesothelioma patients, we used doxorubicin at 15 mg/m2 body surface area (BSA) and cisplatin at 75 mg/m2 BSA for 120 min at 42 °C. For all other tumor entities, we used mitomycin C at 30 mg/m2 BSA in three fractions over 90 min at 42 °C. After completion of the perfusion, chemotherapeutic agents were drained and the abdomen was irrigated with normal saline. The three outflow drains were removed, and the inflow drains (two) remained in situ to serve as postoperative drains. Data about the postoperative course was collected from the electronical medical record and the cancer registry of our university hospital. Complications according to the Clavien-Dindo classification and hospital length of stay were documented. Survival data was extracted from the medical record over the following months and years.
Endpoints
The primary endpoint was overall survival defined as years from date of diagnosis of primary tumor for tumors with synchronous peritoneal metastasis and date of diagnosis of metachronous peritoneal metastasis for tumors without synchronous peritoneal metastasis, respectively, to death, or censored if the patient was still alive at the last follow-up. Median survival was visualized by Kaplan–Meier graph using GraphPad Prism version 9 (GraphPad Software, Inc., San Diego, CA, USA).
Results
There was a total of 40 patients with peritoneal surface malignancies who were treated with CRS and HIPEC between April 2020 and September 2022. Twenty-two patients (55%) were female and 18 patients (45%) were male. Median age at time of surgery was 60 and ranged from 16 to 78 years. ECOG was either 0 (42.5%) or 1 (57.5%) at surgery (Table 1).
Twenty-two patients had peritoneal metastasis from gastric cancer (55%), 8 had pseudomyxoma peritonei (20%), 4 had mesothelioma of the peritoneum (10%), and 6 patients had PSM originating from other primary tumor locations (Fig. 1). Of note, the patient with ovarian cancer was initially diagnosed with urachal cancer with peritoneal metastases. After extensive multidisciplinary discussion, CRS and HIPEC with mitomycin were recommended. Postoperative pathology revealed a diagnosis of ovarian cancer and the patient was subsequently treated with platinum-based chemotherapy.

Location of primary tumor (n = 40). Abbreviations: CUP, cancer of unknown primary; LG-PMP, low-grade pseudomyxoma peritonei; HG-PMP, high-grade pseudomyxoma peritonei
Only four patients did not receive any surgical treatment before CRS-HIPEC and of the 36 patients who did, most had an exploratory laparotomy. 27.5% (11/40) of patients were treated with at least one cycle of PIPAC and those with two or more cycles of PIPAC made up 54.5% (6/11) of this group. Two patients (5%) had had CRS-HIPEC before. The majority of patients had received preoperative systemic chemotherapy. Fifty percent of patients (20/40) had received FLOT, 20% of patients (8/40) FOLFOX, and 17.5% (7/40) other regimes. 27.5% of patients (9/40) had not received any prior chemotherapy. Two patients (5%) had received preoperative radiochemotherapy (Table 1).
Within the subset of 11 patients who received PIPAC prior to undergoing CRS and HIPEC, 9 patients had gastric cancer (7 diffuse, 2 intestinal subtype) (Table 2). All of the gastric cancer patients had received systemic chemotherapy. Five patients with gastric cancer had only one cycle of PIPAC. All of these patients had met eligibility criteria for CRS-HIPEC at the first PIPAC procedure and underwent a change of treatment plan following repeated discussions in our multidisciplinary tumor board and in-depth consultation with the patients and their families. As these patients received only one PIPAC, we cannot assume that the PIPAC procedure contributed to the peritoneal cancer regression. Of note, two of the gastric cancer patients (one diffuse, one intestinal) who received two PIPACs in addition to systemic therapy demonstrated a dramatic response. They were initially excluded from CRS-HIPEC due to their large peritoneal cancer burden, with PCI scores of 35 and 27, respectively, which was found to be 5 and 1 at the time of the last PIPAC. Both patients had a PCI of 0 at CRS and HIPEC which was confirmed by pathological examination of the specimens submitted during cytoreduction. The non-gastric cancer patients of our PIPAC group represent individualized treatment decisions. The patient with the colonic mucinous adenocarcinoma had undergone multiple different chemotherapy regimens and six PIPAC cycles with moderate effect on the PCI which decreased to 25 (from 28). As the oncologist did not see further systemic treatment options and complete cytoreduction seemed feasible, the patient underwent CRS and HIPEC as an individualized treatment decision with good result. The LG-PMP patient was recommended to undergo CRS and HIPEC immediately following diagnosis, but specifically requested PIPAC to delay the decision to undergo major surgery in the face of an ongoing COVID wave.
Median PCI at time of cytoreduction was 4 ranging from 0 to 25. 67.5% had a PCI of 0 to 6 and 32.5% had a PCI of greater or equal 7. Five patients had a PCI of 0 at the time of CRS-HIPEC which was confirmed by pathological examination of the specimens submitted during cytoreduction. Four of these patients were gastric cancer patients (two diffuse, one intestinal, one mixed-type) and all of them had undergone preoperative chemotherapy resulting in regression. Two of the gastric cancer patients had been enrolled in our PIPAC as mentioned above. The 5th patient was a young mesothelioma patient who had undergone open ileocecectomy and local peritonectomy leading to the diagnosis of diffuse epitheloid malignant mesothelioma. After external review by national experts in the field, completion CRS-HIPEC was recommended given the young age of the patient.
Ascites was found in 32.5% of cases. During cytoreductive surgery, 97.5% of patients received a complete parietal peritonectomy, 90% omentectomies, 80% cholecystectomy, and 57.5% gastrectomy. All HIPEC procedures were done via closed approach and chemotherapeutic drugs used were either mitomycin C or cisplatin and doxorubicin. A total of 37 patients (92.5%) were treated with mitomycin C. A concentration of 30 mg/m2 BSA was used for 90 min at a temperature of 42°. Three patients (7.5%) were given a combination of cisplatin and doxorubicin. A concentration of 75 mg/m2 BSA and 15 mg/m2 BSA, respectively, was used for 120 min at a temperature of 42°. Of note, in one patient with gastric adenocarcinoma and peritoneal lesions, the diagnosis changed on final postoperative pathology review. Preoperatively, a biopsy of the peritoneal lesion was diagnosed as a metastasis of the histologically confirmed gastric adenocarcinoma. Postoperatively, the peritoneal lesions were diagnosed as epitheloid mesothelioma. This patient received HIPEC with mitomycin C based on the initial diagnosis. At the end of surgery, completeness of cytoreduction was 0 in 37 patients (92.5%), 1 in 2 patients (5%), and 2 in 1 patient (2.5%) (Table 3). The patient who received HIPEC despite a CC-2 score was a patient with a low-grade pseudomyxoma and a PCI of 18 who required a prolonged surgical procedure and multi-visceral resections (right hemicolectomy, low anterior resection, diverting loop ileostomy, distal gastrectomy, cholecystectomy, omentectomy, total parietal peritonectomy, splenectomy). We achieved a complete cytoreduction with the exception of a 1-cm nodule adjacent to the right portal pedicle. Following intraoperative consultation with our senior liver surgeon, resection of this nodule was considered feasible, but may have necessitated partial hepatectomy. Given the extent of the performed resections, we decided not to proceed any further to avoid the additional morbidity of a major hepatic resection. However, as only a single focus was not cleared, we opted to proceed with HIPEC to provide the patient with the benefit of treating microscopic disease within the peritoneal cavity while accepting future growth of the liver nodule with plans for a staged liver resection after recovery several months later.
Median length of hospital stay was 12 days with a range of 7 to 41 days. Four patients (10%) required reoperation. Thirty-day overall mortality was 7.5% (3/40). One patient died 30 days after surgery after an uneventful postoperative course and timely discharge from hemorrhagic shock caused by a Mallory-Weiss tear of the esophagus, as shown by post-mortem examination. Of note, the post-mortem examination showed an intact anastomosis and no aortoenteric fistula. Another patient died 14 days after surgery from hemorrhagic shock caused by an aortoenteric fistula at the esophagojejunal anastomosis having been treated at the time with endoluminal vacuum therapy for an anastomotic fistula, as shown by post-mortem examination. The third one died 27 days after surgery after initiation of comfort care following a series of reoperations for delayed anastomotic leak of the esophagojejunostomy.
Using the Clavien-Dindo classification to document postoperative complications, complications for nine patients were assessed as grade IIIa/IIIb, one as grade IVa/IVb, and two as grade V (Table 4). Six patients (15%) developed an anastomotic leakage. All anastomotic leakages appeared after gastrectomy at the site of the esophagojejunostomy. Every leak was internally audited and analyzed. Technically issues were found in two cases. In one case, the diameter of the circular stapler was too small for the size of the esophagus leading to increased tension on the anastomosis. In the second case, the 36-Fr silicon tube, which was left in upper abdomen after HIPEC, had obstructed the jejunal limb right distally to the esophagojejunostomy causing a mechanical obstruction. This resulted in a dilatation of the anastomosis and subsequent leakage, as the nasogastric tube had been removed accidentally. Both patients were successfully treated with endoluminal vacuum therapy. No technical issues could be identified in the remainder of patients. All leaks were treated with endoluminal vacuum therapy. Four patients underwent reoperation, and two patients died. The readmission rate within 30 days from discharge was 10% (4/40).
Seventeen of 37 patients (45.9%) received post-HIPEC chemotherapy following repeated discussion in our multidisciplinary tumor board: 12 of 19 (63.2%) gastric cancer patients, 2 of 8 (25%) pseudomyxoma peritonei patients (HG-PMP), 1 of 4 (25%) colon cancer patients, as well as the ovarian and CUP patients. Within the gastric cancer group, there was a delay in treatment due to prolonged recovery in 2 of 19 (10.5%) patients, and 2 of 19 (10.5%) patients were not considered fit for treatment.
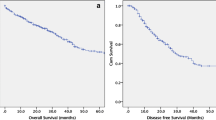
Overall median survival across all patients was 3.69 years from diagnosis (Fig. 2a). Three-, 6-, 9-, and 12-month survival rates were 100%, 92.5% (5% censored), 82.5% (10% censored), and 67.5% (17.5% censored), respectively. The subgroup of gastric cancer patients had a median survival of 1.26 years from the time of diagnosis (Fig. 2b). Three-, 6-, 9-, 12-, 15-, and 18-month survival rates were 100%, 95.5%, 81.8% (4.5% censored), 59.1% (13.6% censored), 40.9% (18.2% censored), and 22.7% (27.3% censored), respectively. When further differentiating based on tumor burden in the group of gastric cancer patients, the median survival for patients with PCI 0–6 was 1.13 years and 1.64 years for patients with PCI ≥ 7 (p = 0.3389) (Fig. 2c). Overall median survival for the whole study population calculated from the date of CRS-HIPEC was 0.83 years (Fig. 2d). Three-, 6-, 9-, and 12-month survival rates were 92.5%, 77.5% (10% censored), 55% (25% censored), and 35% (30% censored), respectively. The subgroup of gastric cancer patients had a median survival of 0.69 years from the date of CRS-HIPEC (Fig. 2e). Three-, 6-, 9-, 12-, 15-, and 18-month survival rates were 72.7% (4.5% censored), 54.5% (13.6% censored), 22.7% (27.3%), 13.6% (27.3% censored), 13.6% (27.3% censored), and 13.6% (27.3% censored), respectively. Gastric cancer patients with PCI 0–6 had a median survival of 0.69 years and patients with PCI ≥ 7 a median survival of 0.66 years (p = 0.6202) (Fig. 2f).

Overall survival. a Overall survival of entire patient cohort from time of diagnosis (years). b Overall survival of gastric cancer patients from time of diagnosis (years). c Overall survival of gastric cancer patients from time of diagnosis (years), grouped by PCI 0–6 and PCI ≥ 7. d Overall survival of entire patient cohort from time of HIPEC (years). e Overall survival of gastric cancer patients from time of HIPEC (years). f Overall survival of gastric cancer patients from time of HIPEC (years), grouped by PCI 0–6 and PCI ≥ 7. Abbreviations: PCI, Peritoneal Cancer Index
As of December 2022, 23 patients (57.5%) were still alive, while 10 patients (25%) had died of tumor related causes, 4 patients (10%) of perioperative complications, and 3 patients of unknown reasons, however, with documented tumor recurrence at time of death.
Discussion
Peritoneal surface malignancies are complex and advanced disease processes and overall associated with a poor prognosis. CRS and HIPEC as part of a multidisciplinary treatment approach can improve survival and have been shown to be the only potentially curative option for the treatment of peritoneal surface malignancies to date [25]. For example, the survival for gastric cancer patients with peritoneal metastasis has been reported to be 4.3 months when treated with best supportive care versus 11.0 months with palliative chemotherapy [41]. Survival can be extended to 12.1 months when treated with CRS or to 18.8 months by combining CRS and HIPEC [25]. A study comparing palliative surgery and systemic chemotherapy with CRS and HIPEC for colorectal cancer with peritoneal metastases showed a median overall survival of 12.5 months for the palliative surgery and chemotherapy group versus 33 months for the CRS-HIPEC group [42]. In the case of malignant peritoneal mesothelioma, survival varies greatly with treatment modalities. While palliative systemic treatment results in a survival of approximately 12 months, more recent studies focusing on CRS and HIPEC report an overall median survival of 53 months, with 5-year survival rates between 42 and 47% [30, 43, 44]. Survival for patients diagnosed with pseudomyxoma peritonei has been found to be much better with a reported median overall survival of 9.8 years after surgery, and reported 5-year and 10-year survival rates of 74% and 63% [31, 45].
However, CRS and HIPEC are extended procedures causing extensive tissue trauma and major inflammatory response which can lead to severe and even life-threatening side effects, complications, prolonged recovery time, and a significant mortality [36], which makes the decision to proceed to CRS and HIPEC challenging for both patients and clinicians. While CRS and HIPEC have become standard of care for a subset of patients with PSM, there is ongoing debate and evolution of various aspects, such as indications, eligibility criteria, and technical standards, and these aspects continue to change based on the available evidence. Our study represents unpolished data from our experience with CRS and HIPEC for the treatment of peritoneal cancer patients. In our cohort of 40 patients, 55% had peritoneal metastasis from gastric cancer, 20% pseudomyxoma peritonei, 10% mesothelioma of the peritoneum (10%), and 6 patients had PSM originating from other primary tumor locations including colon cancer. While CRS and HIPEC represent the standard of care for mesothelioma and PMP patients, there is more disagreement when it comes to gastric or colorectal cancer patients with peritoneal metastases. For example, PRODIGE 7, an influential randomized multicenter trial, questioned the use of HIPEC for patients with colorectal cancer and peritoneal metastases showing no benefit in overall survival for patients who underwent CRS and HIPEC compared to those who underwent CRS only, along with an increase in late postoperative complications in the HIPEC group [46]. The trial was heavily criticized for its limitations such as sample size calculation, the use of a heavily pretreated patient cohort, selection criteria, choice and duration of HIPEC regime (oxaliplatin for 30 min), and a long accrual period. Despite the criticism, the trial had a major impact on practice patterns and decreased the use of CRS-HIPEC for colorectal cancer patients [47]. This is now changing again, as several centers have shifted towards the use of mitomycin-based HIPEC and ongoing trials are investigating further HIPEC regimens for the treatment of colorectal cancer patients with peritoneal metastasis [47]. The role of CRS and HIPEC for gastric cancer with peritoneal metastasis also continues to be in evolution. One randomized controlled trial from Asia showed an overall survival benefit for CRS in combination with HIPEC as compared to CRS alone [40]. The recently published GASTRIPEC-I trial results did not show an overall survival benefit for the CRS-HIPEC group compared to the CRS only group, but significantly improved progression-free and metastasis-free survivals [48]. While additional trials have been designed to further investigate the promising role of CRS-HIPEC in gastric cancer patients with peritoneal metastasis, it is not yet considered standard of care and many patients are offered palliative chemotherapy only.
As a specialized center for PSM, the University Hospital Münster offers PIPAC treatment for patients with peritoneal cancers, ideally in combination with systemic therapy. Offering PIPAC treatment provided us with the opportunity to regularly assess treatment response by laparoscopy and allowed us to witness dramatic treatment responses in patients with gastric cancer and peritoneal metastases which had led to a complete eradication of a large peritoneal cancer burden in two patients. It is beyond the scope of this study, to discuss, if and how much the actual PIPAC treatment contributed to the regression, as both patients received extensive chemotherapy in addition. However, as we would have not performed the laparoscopies, if the patients had not been enrolled in our PIPAC program, it is unlikely that the patients would have received CRS-HIPEC otherwise. Another aspect of ongoing discussion is the extent of the peritoneal cancer burden that excludes a patient from CRS-HIPEC. Complete cytoreduction has been shown to be the most important predictor of survival [49,50,51,52] and the peritoneal cancer burden is often used to predict the feasibility of a complete cytoreduction. To quantify the tumor burden macroscopically, the Peritoneal Carcinomatosis Index (PCI) according to Sugarbaker [53,54,55] is determined. PCI ranges from 0 (indicating no visible peritoneal implants) to 39 (peritoneal cancer everywhere) [54]. Various PCI cutoffs have been suggested for different cancer histologies. For gastric cancer, a PCI of 6 or smaller is often suggested as a cutoff for proceeding with CRS/HIPEC given the high chance of complete cytoreduction [25, 56, 57]. In our patient cohort, about two thirds of patients had a PCI below 7, but we did include patients with higher PCIs when the distribution of carcinomatosis was favorable and a complete cytoreduction was feasible. We found no significant survival difference for the cohort with metastatic gastric cancer comparing patients with PCI of less than 7 and patient with a PCI of 7 and higher. The median overall survival of our gastric cancer cohort was over 15 months after CRS/HIPEC counting from the time of diagnosis, 8.3 months counting from the time of CRS/HIPEC. A major concern has always been the potential increase in complications when adding HIPEC after completion of cytoreductive surgery. We experienced an acceptable complication rate for CRS/HIPEC in our cohort with 25% grade III/IV complications and 5% in-hospital 30-day mortality. The anastomotic leak rate was 15%. The leaks appeared after gastrectomy at the site of the esophagojejunostomy and most of them were successfully treated with endoluminal vacuum therapy. All of our patients received HIPEC at the end of the surgery, so we do not have a direct comparison with a non-HIPEC group. However, several randomized and non-randomized studies showed no additional morbidity and mortality when comparing CRS with CRS-HIPEC [25, 58, 59].
CRS-HIPEC is a promising tool in the treatment of peritoneal surface malignancies with vast potential and there is ongoing change and evolution of this tool [60, 61]. Here, we presented our clinical experience with CRS and HIPEC at the University Hospital Münster in Germany to add to the discussion. As described, we provided tailored treatment for individual patients which did not always fit the criteria presented in studies or guidelines, but could serve as a starting point for future investigations, such as the use of PIPAC as pseudo-neoadjuvant treatment strategy in preparation for CRS-HIPEC.
Conclusion
CRS-HIPEC has the potential to drastically influence the course of disease in patients with peritoneal surface malignancies, and will continue to play a major role for these patients in the future. Additional studies will help to further specify the selection criteria for different patients and cancer types.
References
Cortés-Guiral D et al (2021) Primary and metastatic peritoneal surface malignancies. Nat Rev Dis Primers 7(1):91
Burg L et al (2020) Incidence and predictors of peritoneal metastases of gynecological origin: a population-based study in the Netherlands. J Gynecol Oncol 31(5):e58
Thomassen I et al (2014) Peritoneal carcinomatosis of gastric origin: a population-based study on incidence, survival and risk factors. Int J Cancer 134(3):622–628
Rijken A, Lurvink RJ, Luyer MDP, Nieuwenhuijzen GAP, van Erning FN, van Sandick JW, de Hingh IHJT (2021) The burden of peritoneal metastases from gastric cancer: a systematic review on the incidence, risk factors and survival. J Clin Med 10(21):4882. https://doi.org/10.3390/jcm10214882
Satoh H et al (2001) Peritoneal carcinomatosis in lung cancer patients. Oncol Rep 8(6):1305–1307
Bertozzi S et al (2015) Prevalence, risk factors, and prognosis of peritoneal metastasis from breast cancer. Springerplus 4:688
Klos D et al (2019) Trends in peritoneal surface malignancies: evidence from a Czech nationwide population-based study. World J Surg Oncol 17(1):182
Consonni D et al (2019) Peritoneal mesothelioma and asbestos exposure: a population-based case-control study in Lombardy Italy. Occup Environ Med 76(8):545–553
van Kooten JP et al (2022) Incidence, treatment and survival of malignant pleural and peritoneal mesothelioma: a population-based study. Thorax
Carr NJ et al (2016) A consensus for classification and pathologic reporting of pseudomyxoma peritonei and associated appendiceal neoplasia: the results of the Peritoneal Surface Oncology Group International (PSOGI) Modified Delphi Process. Am J Surg Pathol 40(1):14–26
Carr NJ et al (2017) The histopathological classification, diagnosis and differential diagnosis of mucinous appendiceal neoplasms, appendiceal adenocarcinomas and pseudomyxoma peritonei. Histopathology 71(6):847–858
Khomyakov V et al (2016) Bidirectional chemotherapy in gastric cancer with peritoneal metastasis combining intravenous XELOX with intraperitoneal chemotherapy with low-dose cisplatin and Doxorubicin administered as a pressurized aerosol: an open-label, Phase-2 study (PIPAC-GA2). Pleura Peritoneum 1(3):159–166
Tempfer CB (2015) Pressurized intraperitoneal aerosol chemotherapy as an innovative approach to treat peritoneal carcinomatosis. Med Hypotheses 85(4):480–484
Demtroder C et al (2016) Pressurized intraperitoneal aerosol chemotherapy with oxaliplatin in colorectal peritoneal metastasis. Colorectal Dis 18(4):364–371
Alyami M et al (2017) Multicentric initial experience with the use of the pressurized intraperitoneal aerosol chemotherapy (PIPAC) in the management of unresectable peritoneal carcinomatosis. Eur J Surg Oncol 43(11):2178–2183
Khosrawipour T, Khosrawipour V, Giger-Pabst U (2017) Pressurized intra peritoneal aerosol chemotherapy in patients suffering from peritoneal carcinomatosis of pancreatic adenocarcinoma. PLoS ONE 12(10):e0186709
Falkenstein TA et al (2018) First clinical data of Pressurized Intraperitoneal Aerosol Chemotherapy (PIPAC) as salvage therapy for peritoneal metastatic biliary tract cancer. Anticancer Res 38(1):373–378
Horvath P et al (2018) Pressurized intraperitoneal aerosol chemotherapy (PIPAC) for peritoneal metastases of pancreas and biliary tract cancer. Clin Exp Metastasis 35(7):635–640
Di Giorgio A, Macrì A, Ferracci F, Robella M, Visaloco M, De Manzoni G, Sammartino P, Sommariva A, Biacchi D, Roviello F, Pastorino R, Pires Marafon D, Rotolo S, Casella F, Vaira M (2023) 10 years of pressurized intraperitoneal aerosol chemotherapy (pipac): a systematic review and meta-analysis. Cancers (Basel) 15(4):1125. https://doi.org/10.3390/cancers15041125
Sgarbura O et al (2022) Consensus statement for treatment protocols in pressurized intraperitoneal aerosol chemotherapy (PIPAC). Pleura Peritoneum 7(1):1–7
Hubner M et al (2017) Feasibility and safety of pressurized intraperitoneal aerosol chemotherapy for peritoneal carcinomatosis: a retrospective cohort study. Gastroenterol Res Pract 2017:6852749
Nadiradze G et al (2016) Pressurized Intraperitoneal Aerosol Chemotherapy (PIPAC) with low-dose cisplatin and doxorubicin in gastric peritoneal metastasis. J Gastrointest Surg 20(2):367–373
Alyami M et al (2021) Pressurized intraperitoneal aerosol chemotherapy (PIPAC) for unresectable peritoneal metastasis from gastric cancer. Eur J Surg Oncol 47(1):123–127
Alyami M et al (2019) Pressurised intraperitoneal aerosol chemotherapy: rationale, evidence, and potential indications. Lancet Oncol 20(7):e368–e377
Bonnot PE et al (2019) Cytoreductive Surgery With or Without Hyperthermic Intraperitoneal Chemotherapy for Gastric Cancer With Peritoneal Metastases (CYTO-CHIP study): a propensity score analysis. J Clin Oncol 37(23):2028–2040
Sugarbaker PH (1995) Peritonectomy procedures. Ann Surg 221(1):29–42
Guerra-Londono CE et al (202) The role of hyperthermia in the treatment of peritoneal surface malignancies. Curr Oncol Rep
Ramirez MF et al (2022) Temperature management during cytoreductive surgery with hyperthermic intraperitoneal chemotherapy. Front Oncol 12:1062158
Glehen O, Mohamed F, Gilly FN (2004) Peritoneal carcinomatosis from digestive tract cancer: new management by cytoreductive surgery and intraperitoneal chemohyperthermia. Lancet Oncol 5(4):219–228
Yan TD et al (2009) Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy for malignant peritoneal mesothelioma: multi-institutional experience. J Clin Oncol 27(36):6237–6242
Chua TC et al (2012) Early- and long-term outcome data of patients with pseudomyxoma peritonei from appendiceal origin treated by a strategy of cytoreductive surgery and hyperthermic intraperitoneal chemotherapy. J Clin Oncol 30(20):2449–2456
Verwaal VJ et al (2008) 8-year follow-up of randomized trial: cytoreduction and hyperthermic intraperitoneal chemotherapy versus systemic chemotherapy in patients with peritoneal carcinomatosis of colorectal cancer. Ann Surg Oncol 15(9):2426–2432
Elias D et al (2010) Peritoneal colorectal carcinomatosis treated with surgery and perioperative intraperitoneal chemotherapy: retrospective analysis of 523 patients from a multicentric French study. J Clin Oncol 28(1):63–68
Goéré D et al (2013) Is there a possibility of a cure in patients with colorectal peritoneal carcinomatosis amenable to complete cytoreductive surgery and intraperitoneal chemotherapy? Ann Surg 257(6):1065–1071
van Driel WJ et al (2018) Hyperthermic intraperitoneal chemotherapy in ovarian cancer. N Engl J Med 378(3):230–240
Alyami M et al (2018) Ninety-day post-operative morbidity and mortality using the National Cancer Institute’s common terminology criteria for adverse events better describe post-operative outcome after cytoreductive surgery and hyperthermic intraperitoneal chemotherapy. Int J Hyperthermia 34(5):532–537
Jacquet P, Sugarbaker PH (1996) Clinical research methodologies in diagnosis and staging of patients with peritoneal carcinomatosis. Cancer Treat Res 82:359–374
Glehen O et al (2008) Hyperthermic intraperitoneal chemotherapy: nomenclature and modalities of perfusion. J Surg Oncol 98(4):242–246
Glehen O et al (2004) Cytoreductive surgery and intraperitoneal chemohyperthermia for peritoneal carcinomatosis arising from gastric cancer. Arch Surg 139(1):20–26
Yang XJ et al (2011) Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy improves survival of patients with peritoneal carcinomatosis from gastric cancer: final results of a phase III randomized clinical trial. Ann Surg Oncol 18(6):1575–1581
Wagner AD et al (2017) Chemotherapy for advanced gastric cancer. Cochrane Database Syst Rev 8(8):p Cd004064
Chua TC et al (2013) Summary of current therapeutic options for peritoneal metastases from colorectal cancer. J Surg Oncol 107(6):566–573
Yan TD et al (2007) A systematic review on the efficacy of cytoreductive surgery combined with perioperative intraperitoneal chemotherapy for diffuse malignancy peritoneal mesothelioma. Ann Oncol 18(5):827–834
Helm JH et al (2015) Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy for malignant peritoneal mesothelioma: a systematic review and meta-analysis. Ann Surg Oncol 22(5):1686–1693
Miner TJ et al (2005) Long-term survival following treatment of pseudomyxoma peritonei: an analysis of surgical therapy. Ann Surg 241(2):300–308
Quénet F et al (2021) Cytoreductive surgery plus hyperthermic intraperitoneal chemotherapy versus cytoreductive surgery alone for colorectal peritoneal metastases (PRODIGE 7): a multicentre, randomised, open-label, phase 3 trial. Lancet Oncol 22(2):256–266
Sommariva A et al (2022) Colorectal cancer with peritoneal metastases: the impact of the results of PROPHYLOCHIP, COLOPEC, and PRODIGE 7 trials on peritoneal disease management. Cancers (Basel) 15(1)
Rau B et al (2024) Effect of hyperthermic intraperitoneal chemotherapy on cytoreductive surgery in gastric cancer with synchronous peritoneal metastases: the phase III GASTRIPEC-I trial. J Clin Oncol 42(2):146–156
Glehen O et al (2010) Peritoneal carcinomatosis from gastric cancer: a multi-institutional study of 159 patients treated by cytoreductive surgery combined with perioperative intraperitoneal chemotherapy. Ann Surg Oncol 17(9):2370–2377
Canbay E et al (2014) Outcome data of patients with peritoneal carcinomatosis from gastric origin treated by a strategy of bidirectional chemotherapy prior to cytoreductive surgery and hyperthermic intraperitoneal chemotherapy in a single specialized center in Japan. Ann Surg Oncol 21(4):1147–1152
Chia CS et al (2016) Patients with peritoneal carcinomatosis from gastric cancer treated with cytoreductive surgery and hyperthermic intraperitoneal chemotherapy: is cure a possibility? Ann Surg Oncol 23(6):1971–1979
Rau B et al (2019) The efficacy of treatment options for patients with gastric cancer and peritoneal metastasis. Gastric Cancer 22(6):1226–1237
Giger-Pabst U et al (2018) Pressurized IntraPeritoneal Aerosol Chemotherapy (PIPAC) for the treatment of malignant mesothelioma. BMC Cancer 18(1):442
Harmon RL, Sugarbaker PH (2005) Prognostic indicators in peritoneal carcinomatosis from gastrointestinal cancer. Int Semin Surg Oncol 2(1):3
Sugarbaker PH, Jablonski KA (1995) Prognostic features of 51 colorectal and 130 appendiceal cancer patients with peritoneal carcinomatosis treated by cytoreductive surgery and intraperitoneal chemotherapy. Ann Surg 221(2):124–132
Yarema R et al (2019) Hyperthermic intraperitoneal chemotherapy (HIPEC) in combined treatment of locally advanced and intraperitonealy disseminated gastric cancer: a retrospective cooperative Central-Eastern European study. Cancer Med 8(6):2877–2885
Rau B et al (2020) Peritoneal metastasis in gastric cancer: results from the German database. Gastric Cancer 23(1):11–22
Patel M et al (2023) Effect of hyperthermic intraperitoneal chemotherapy (HIPEC) on survival and recurrence rates in advanced gastric cancer- a systematic review and meta-analysis. Int J Surg
Martins M et al (2022) Impact of cytoreductive surgery with hyperthermic intraperitoneal chemotherapy in the treatment of gastric cancer with peritoneal carcinomatosis: a systematic review and meta-analysis. Ann Surg Oncol 29(12):7528–7537
Ukegjini K, Guidi M, Lehmann K, Süveg K, Putora PM, Cihoric N, Steffen T (2023) Current research and development in hyperthermic intraperitoneal chemotherapy (HIPEC)-a cross-sectional analysis of clinical trials registered on clinicaltrials.gov. Cancers (Basel) 15(7):1926. https://doi.org/10.3390/cancers15071926
Manzanedo I, Pereira F, Pérez-Viejo E, Serrano Á (2023) Gastric cancer with peritoneal metastases: current status and prospects for treatment. Cancers (Basel) 15(6):1777. https://doi.org/10.3390/cancers15061777
Author information
Authors and Affiliations
Contributions
MR and JCS conceptualized the study. MR and JCS collected, analyzed, and interpreted the data. MR and JCS wrote the original draft of the manuscript. AE, TMN, and AP reviewed and edited the manuscript. JCS supervised the project. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Reese, M., Eichelmann, AK., Nowacki, T.M. et al. The role of cytoreductive surgery and HIPEC for the treatment of primary and secondary peritoneal malignancies—experience from a tertiary care center in Germany. Langenbecks Arch Surg 409, 113 (2024). https://doi.org/10.1007/s00423-024-03309-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00423-024-03309-9