
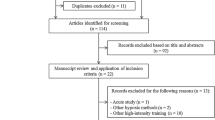
Abstract
Purpose
To investigate (1) the boosting effects immediately and 4 weeks following 2-week, 6-session repeated-sprint training in hypoxia (RSH2-wk, n = 10) on the ability of team-sport players in performing repeated sprints (RSA) during a team-sport-specific intermittent exercise protocol (RSAIEP) by comparing with normoxic counterpart (CON2-wk, n = 12), and (2) the dose effects of the RSH by comparing the RSA alterations in RSH2-wk with those resulting from a 5-week, 15-session regimen (RSH5-wk, n = 10).
Methods
Repeated-sprint training protocol consisted of 3 sets, 5 × 5-s all-out sprints on non-motorized treadmill interspersed with 25-s passive recovery under the hypoxia of 13.5% and normoxia, respectively. The within- (pre-, post-, 4-week post-intervention) and between- (RSH2-wk, RSH5-wk, CON2-wk) group differences in the performance of four sets of RSA tests held during the RSAIEP on the same treadmill were assessed.
Results
In comparison with pre-intervention, RSA variables, particularly the mean velocity, horizontal force, and power output during the RSAIEP enhanced significantly immediate post RSH in RSH2-wk (5.1–13.7%), while trivially in CON2-wk (2.1–6.2%). Nevertheless, the enhanced RSA in RSH2-wk diminished 4 weeks after the RSH (− 3.17–0.37%). For the RSH5-wk, the enhancement of RSA immediately following the 5-week RSH (4.2–16.3%) did not differ from that of RSH2-wk, yet the enhanced RSA was well-maintained 4-week post-RSH (0.12–1.14%).
Conclusions
Two-week and five-week RSH regimens could comparably boost up the effects of repeated-sprint training in normoxia, while dose effect detected on the RSA enhancement was minimal. Nevertheless, superior residual effects of the RSH on RSA appear to be associated with prolonged regimen.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
In intermittent-type sports, such as football and handball, the repeated-sprint ability (RSA) of players, which refers to their ability in sustaining the highest speed over a series of sprints (≤ 6 s), interspersed with short (≤ 30 s) recovery periods, is of the essence in determining the final outcome of a game by associating to the appropriateness of technical and tactical behaviors and cognitive choices (Mohr et al. 2005). For augmenting the competitive edge in matches, sports teams usually adopt specific repeated-sprint training (RST) regimens in different training periods to maximize players’ performance (Ferrari Bravo et al. 2007; Turner and Stewart 2013). Since last decade, massive evidence has shown that RST under hypoxia (RSH) could boost up the effects of normoxic RST on players’ sea-level RSA (Brocherie et al. 2017). Enhanced perfusion and O2 utilization in skeletal muscles, rather than erythrocytosis resulting from prolonged hypoxic exposure, were the partly attributions (Millet et al. 2019). Although RSH was purported to ergogenically enhance the RSA, the boosting effects were mostly demonstrated in RSA tests by repeating sprints for a given distance with uniform interval recovery time in between, or in the Yo–Yo intermittent recovery test (Bangsbo and Mohr 2012; Brocherie et al. 2017). The validation of RSH by examining its beneficial effects on players’ ability in performing repeated sprints during a simulated prolonged intermittent-type sports game scenario, which is more ecological, has never been examined.
General consensus have long been reached among coaches in team sports that periodization of training could provide systematic variation of physical conditioning to players, directing their resultant physiological adaptations to meet the training goals of the sport (Plisk and Stone 2003) However, providing appropriate physical conditioning to players within the time allow, while they have varied training goals, concurrent training and practices, and extended season of competition requires considerable precise information of each conditioning item and parameter for planning (Gamble 2006). The effective duration of RSH, sensibly, would become an essential factor in determining the practicability of RSH in team sports. In previous studies, the training volume adopted in RSH was diverse with duration (weeks) x frequency (sessions wk−1) ranging from 2 × 2 to 5 × 3 (Millet et al. 2019). Nonetheless, most of the RSH regimens with diverged training volume were reported to improve athletes’ RSA significantly (Beard et al. 2019a, b; Brocherie et al. 2015; Galvin et al. 2013). The brief RSH regimen composed of less training sessions (Beard et al. 2019a, b) may be practically relevant to in-season shock microcycle training. Yet, prolonged RSH compared to the brief counterparts, which may be more favorable to morphological muscle adaptations, i.e., sarcoplasmic reticulum and muscle fiber size (Ross and Leveritt 2001), may potentially lead to greater enhancement in RSA that may be meaningful to players in physical conditioning in pre-season. The dose–response effects of RSH on the enhancement of the RSA during a simulated intermittent-type sports game situation have never been investigated. It has been reported that the molecular beneficial adaptations to RSH in skeletal muscles decayed 3-week post-intervention, while associated improved RSA did not (Brocherie et al. 2018). The residual effects of RSH on the special RSA was also not clear. Improved understanding of the immediate and residual effects of RSH on the RSA could facilitate coaches to condition players in different seasonal phases by engaging in the specific training regimen.
The purposes of this study were to examine (1) the boosting effects immediately and 4 weeks following a short-term RSH regimen (RSH2-wk: 2 weeks × 3 sessions wk−1) on the RSA of team-sport players during a team-sport-specific intermittent exercise protocol (RSAIEP) by comparing with their normoxic counterparts (CON2-wk: 2 weeks × 3 sessions wk−1); and (2) the dose effects of RSH on the immediate post- and 4-week post-training RSA enhancement by comparing the specific adaptations of RSH2-wk with those resulting from an identical RSH regimen with apparent longer training duration (RSH5-wk: 5 weeks × 3 sessions wk−1). It was hypothesized that the RSH2-wk regimen would boost up the immediate and residual training effects of normoxic RST on players’ RSA during the RSAIEP, while the boosting effects following the RSH5-wk would be significantly greater than that of RSH2-wk.
Methods
Participants
Using G*Power software to perform a priori, two-tailed power calculation at an alpha of 0.05 and a power of 80%, and based on our pilot study findings of RSH on RSA (effect size of 1.2) in trained athletes, a minimum of 10 participants in each group were required for this study. 32 male players from university football and handball teams volunteered to participate in the study. After being fully informed of the experimental procedures and possible exercise- and blood test-induced discomfort, players gave their written informed consent. Ethical approval for this study was obtained from the Committee on the Use of Human and Animal Subjects in Teaching and Research at Macao Polytechnic University. The study was conducted in accordance with the Declaration of Helsinki.
Experimental design
For examining the effects of RSH on the specific RSA, all players participated in the intervention of RST under normoxia or hypoxia. Within a week prior to the intervention, the pre-training RSA of the players during the RSAIEP that was taken place on a non-motorized treadmill, as well as their maximum performance of the Yo–Yo intermittent recovery test were assessed. Afterwards, 22 players with matched RSA (mean velocity of repeated sprints) were randomly assigned into RSH2-wk (n = 10) or CON2-wk (n = 12). The rest players with comparable RSA were assigned into RSH5-wk (n = 10) to receive the 5-week RSH. The interventions of the three groups were taken place simultaneously during late off-season and pre-season period. During the period, the players received sports training for 2–3 h day−1, 4–5 days wk−1. The training sessions were composed various physical conditioning including sport-specific conditioning, functional training, ball work and recovery sessions. All the training sessions of CON2-wk and RSH2-wk, and the training sessions of RSH5-wk in the first 2 weeks were scheduled on the same days to equalize the possible influence of sport-team training on the RST in each group. During the intervention, RST was carried out on the same non-motorized treadmill which was placed inside a normobaric hypoxic chamber, while players were blinded to the hypoxic level. Following the training, identical RSA tests were conducted 2 days (immediate effect), and 4 weeks (residual effect) after the last RST session. The differences between RSH2-wk vs CON2-wk, as well as RSH5-wk vs RSH2-wk in the alterations in RSA among pre-, post- and 4-week post-RST trials were compared.
All the exercise tests were scheduled at the same time of day to control for diurnal variation influences and were separated by a minimum of 2 days to avoid residual fatigue induced by preceded exercise test. During the study period, all players were instructed to maintain their dietary habits. Prior to each test, players refrained from eating for at least 2 h, and were prohibited to take any additional energy supplements.
Procedures
Preliminary tests and familiarization trials
Prior to the experimental trials, players’ physical characteristics including \(\dot{V}\)O2max and percentage of body fat were assessed as previously reported (Nie et al. 2022; Tong et al. 2001). Afterwards, the maximum treadmill braking resistance (TRmax) and the maximal sprint velocity on the treadmill that were the required criteria for subsequent treadmill ergometry were determined individually. The TRmax in kp was defined as the maximum resistance of the treadmill belt that the players can move consecutively for three steps. The maximal sprint velocity was measured by performing three maximal 4-s sprints on the treadmill at 5% TRmax, each separated by 14 s of passive recovery. The highest velocity obtained in a single second from the three sprints was the result (Zois et al. 2013). The assessments of \(\dot{V}\)O2max and maximal sprint velocity were repeated after intervention. Following preliminary testing, players were familiarized with the repeated-sprint tests that was incorporated into the RSAIEP on the treadmill. This familiarization period introduced the testing equipment and protocols and provided the players with experience of exercising at assigned walking and running speed.
Experimental trials
Team-sport specific RSA assessment
The assessment of the RSA during the RSAIEP has been reported recently (Sirotic and Coutts 2008; Tong et al. 2019). Briefly, the RSAIEP required players to work on a non-motorized treadmill (Force 3, Woodway, USA) with braking resistance set at 5% TRmax for ~ 30 min. The RSAIEP was interspersed with 42 8-s standing still (19.2% overall duration), 75 8-s walking (34.2%), 56 8-s jogging (25.6%), 36 6-s running (12.3%), 20 4-s dashing (4.6%), and 24 3-s sprinting (4.1%) (Fig. 1). The speed for each foregoing activity was defined at 0%, 20%, 35%, 50%, 70% and 100% of the maximal sprint velocity, respectively. During the RSAIEP, all players were required to perform the six activities on the treadmill by complying with the velocity assigned.

Team-sport-specific intermittent exercise protocol with 4 sets of repeated-sprint test each composed of 3 × 4-s all-out sprints interspersed in it. Texts are activity (time for each bout, number of bouts, percentage of overall duration)
In addition, 4 sets of RSA test each composed of 3 × 4-s all-out sprints at 20% TRmax, with 14-s passive recovery in between, were incorporated into the RSAIEP at the beginning (1 set), middle (2 sets), and end (1 set) of the protocol. During each sprint, the alterations in velocities, horizontal force, and power output were recorded at 25 Hz using the Woodway Force 3.0 software. The measurement of the horizontal force on the treadmill as well as the preceded calibration of the force sensor for the measurement were performed in accordance with the guidelines manufacturer provided. For the calculation of peak and mean velocity of each sprint, the start point was standardized to 1 m s−1; from this point, a 4-s period was calculated. The average of peak (P-Vel) and mean (M-Vel) velocities, mean horizontal force (M-Hf), and mean power output (M-Po) of the three sprints in each set, as well as the total work done (WTot) of the RSAIEP (excluded the 4 sets of RSA test) were the results for analysis. During the four sets of the RSA tests, all players were required to exercise all-out in each 4-s sprint bout and avoid any pacing strategy in repeating the tests.
Before the RSAIEP, participants performed a 10-min standardized warm-up exercise including a 5-min motorized treadmill run at moderate intensity and a 5-min dynamic stretching exercise mainly using the legs. Following capillary sampling from fingertip for blood lactate measurement, and performance of one bout of each activity and three bouts of 5-s submaximal sprints on the non-motorized treadmill for warm-up purposes, the RSAIEP protocol commenced. Exercise heart rate (HR) was monitored using a Polar HR monitor (H6, Finland). Five minutes after the RSAIEP, fingertip blood sampling was repeated. The pre- and post-RSAIEP blood samples were collected for examining the change in blood lactate (ΔLa) using the Lactate Scout + analyzer (EKF Diagnostics, UK). Within 30 min after the RSAIEP, players were required to score from 0 to 10 based on the CR-10 RPE scale (Borg et al. 1985) on how hard they perceived the RSAIEP. The session rating of perceived exertion (s-RPE) for quantifying the associated internal exercise stress was then calculated as (Foster et al. 2001):
Yo–Yo intermittent recovery test-Level 1(Yo–Yo IR1)
The test consisted of 2 × 20-m intervals of running interspersed by regular 10-s recovery periods. The players ran back and forward the 20 m on ground by following the pre-set signal that control the speed. The speed of the intermittent run increased progressively stage-by-stage. The players continued the intermittent run until fail to complete the run in time twice. The total running distance covered was the result.
Interventions
In this study, all players’ RST were performed on the same Woodway non-motorized treadmill which was placed in a hypoxic chamber with dimensions of 7 m (length) × 5 m (width) × 3 m (height). The O2 concentration inside the chamber can be adjusted within the range from 21% (sea-level) to 11% (hypoxia) using Welltech hypoxic system [HS500, Welltech, China].
The RST protocol was consisted of three sets of 5 × 5-s sprints interspersed with 25-s passive recovery at the ratio of exercise to recovery of 1:5, and with 5-min passive recovery in between sets (Brocherie et al. 2017). The treadmill resistance was set at 20% of TRmax. For CON2-wk, players performed three sessions of the RST under normoxia on alternate days per week for 2 weeks. The temperature was kept at 22 °C. For RSH, players performed identical training protocol under normobaric hypoxia, with inspired O2 fraction set at 13.5% corresponding to that of altitude of 3500 m, three sessions per week for 2 weeks in RSH2-wk, and that for 5 weeks in RSH5-wk. The specific RSH variables of inspired O2 fraction and ratio of exercise to recovery, as well as the passive recovery modality have been shown to be able to induce maximum stress of hypoxia in players during the specific training (Tong et al. 2021). All players were blinded to the hypoxic level during the intervention.
Prior to the repeated-sprint exercise in each session, players rested on a chair for 2 min in the hypoxic chamber. Their peripheral capillary O2 saturation (SpO2) was monitored using a pulse oximeter (Masimo, USA). The SpO2 displayed on the oximeter was hidden from them and was recorded at the end of the monitoring period. Following three bouts of 5-s submaximal sprints (70–90% all-out effort) on the non-motorized treadmill for warm-up purposes, the RST protocol commenced. Exercise HR were monitored using the same Polar HR monitor throughout the training session. s-RPE was measured using the same CR-10 RPE scale. The velocity and power output of each sprint were recorded. At the time when players demonstrated the adaptation to a given external training load by significant increase in the average of the mean power output of each set from original level in consecutive two sessions, the load would be increased by increasing the treadmill resistance with each increment of 1 kp.
Statistical analyses
The Shapiro–Wilk normality test revealed that data for all variables were normally distributed. The differences in physical characteristics, TRmax, and RST variables (Tables 1 and 2) among the three groups (CON2-wk, RSH2-wk, and RSH5-wk) were assessed using one-way analysis of variance (ANOVA) with repeated measures. To examine the differences in \(\dot{V}\)O2max, maximal sprint velocity, Yo–Yo IR1, as well as the exercise stress variables and WTot of RSAIEP among trials (pre-, post-, 4-week post-RST) and across the three groups (Tables 3 and 4), two-way ANOVA with repeated measures were computed. For the variables of the treadmill RSA test (Fig. 2a–d), the differences among sets (1st–4th sets), across trials, and between groups were assessed by applying three-way ANOVA with repeated measures in two factors. Post hoc analyses for ANOVA, using the Bonferroni test for identifying simple main effects, were performed when a significant interaction was detected. Partial eta squared (ηρ2) was used to indicate the effect size and to measure the main and interaction effects, where values of 0.04 = small, 0.25 = medium, and 0.64 = large effect size (Ferguson 2009). The effect size of pairwise comparison was revealed by calculating Cohen's d, where d = 0.2, 0.5, and 0.8 indicate small, medium, and large effect sizes, respectively (Cohen 1988). Statistical significance was set at p < 0.05, and values are reported as means ± SD.

a Peak velocity, b mean velocity, c mean horizontal force, and d mean power output across the four sets (1st–4th sets) of the repeated-sprint test held during the RSAIEP in the three trials (pre-RST, post-RST, 4-week post-RST) of the CON2-wk, RSH2-wk, and RSH5-wk. Three-way ANOVA (Trials x Sets x Groups): F-ratio, p value (ηρ2); a significant different from corresponding 1st set value in pre-RST trial at p < 0.05, b significant different from corresponding 1st set value in post-RST trial at p < 0.05, c significant different from corresponding 1st set value in 4-week post-RST trial at p < 0.05, *significant different from corresponding pre-RST value at p < 0.05, α significant different from corresponding CON2-wk value at p < 0.05
Results
Table 1 shows the players’ physical characteristics and TRmax. All variables did not vary among the CON2-wk, RSH2-wk, and RSH5-wk.
All players in the CON2-wk, RSH2-wk, and RSH5-wk were able to complete the RST with attendance of 100%. No adverse events were reported during training in either group. The external training load of all players in CON2-wk and RSH2-wk were maintained at original level throughout the intervention, while nine of the ten players in RSH5-wk had increased their treadmill resistance of 1 kp either in the 3rd or 4th week of the 5-week RSH. Table 2 shows the averages of the O2 concentration in the hypoxic chamber, and of the players’ SpO2, post-exercise HR, and s-RPE recorded in each training session during the intervention period of the three groups. During the intervention, the O2 concentration inside the hypoxic chamber was not different between RSH2-wk and RSH5-wk, and both were significantly lower than that of CON2-wk. The pre-exercise SpO2 of the players in RSH2-wk and RSH5-wk declined significantly in comparison with that of CON2-wk (Cohen’s d = 10.9, 9.3), while the alteration of SpO2 between the two RSH groups was not different. For the internal training load of the RST, the post-exercise HR as well as the s-RPE among the three training regimens were not different.
This study aims to examine the boosting effects of CON2-wk vs RSH2-wk, and RSH2-wk vs RSH5-wk, on the ability of team-sport players in performing \(\dot{V}\)O2max and maximal sprint velocity tests, Yo–Yo IR1, and repeated sprints during RSAIEP, the results of the comparisons between CON2-wk vs RSH5-wk were not reported. In Tables 3 and 4, and Fig. 2a–d, all the selected variables of players’ exercise performance prior to the RST were not different among the CON2-wk, RSH2-wk, and RSH5-wk.
RSH2-wk vs CON2-wk
The alterations in \(\dot{V}\)O2max, maximal sprint velocity, and Yo–Yo IR1 performance post RST are shown in Table 3. In comparison with pre-RST values, \(\dot{V}\)O2max and maximal sprint velocity did not change significantly post RST in both RSH2-wk and CON2-wk. For the performance of Yo–Yo IR1 in RSH2-wk, significant improvements in the post-RST and 4-week post-RST trials (Cohen’s d = 1.03, 0.88) were observed. Contrastingly, Yo–Yo IR1 performance in CON2-wk did not change.
Table 4 shows the post-exercise HR, ΔLa, s-RPE and WTot during the RSAIEP in the pre-, post- and 4-week post-RST trials in CON2-wk, RSH2-wk, and RSH5-wk. For the variables of post-exercise HR, ΔLa, s-RPE, there was no significant difference among the pre-, post- and 4-week post-RST trials in both CON and RSH groups. Nevertheless, the WTot of the RSAIEP in the post-RST, but not the 4-week post-RST, trial was significantly greater than that of pre-RST in both groups (Cohen’s d, CON2-wk = 0.78; RSH2-wk = 0.38). The increased WTot was not different between the CON and RSH groups.
In this study, players’ RSA were assessed by measuring the P-Vel, M-Vel, M-Hf, and M-Po in the four sets of RSA test that were held during the RSAIEP. The alterations in the RSA variables among the four tests in the pre-, post-, and 4-week post-RST trials, and their interactions across CON2-wk, RSH2-wk, and RSH5-wk are shown, respectively, in Fig. 2a–d. In the pre-, post- and 4-week post-RST trials, the changes in the P-Vel during the RSA tests, in comparison with the corresponding 1st set value, were generally not significant in both CON2-wk and RSH2-wk (Fig. 2a), with only a minor decrease found in the 3rd set during the 4-week post-RST trial in CON2-wk (Cohen’s d = 1.43). Following the 2-week RSH in RSH2-wk, the P-Vel in the post-RSH trial, in comparison with the corresponding pre-RSH value, did not alter, while a significant increase in P-Vel was noted in the 3rd set of the 4-week post-RSH trial (Cohen’s d = 2.05). Related change was not found in CON2-wk.
For the time course of M-Vel (Fig. 2b), marked decrease in the pre-RST trial was observed in both groups, with the M-Vel in the 3rd set of the RSA test reduced significantly from the 1st set (Cohen’s d, CON2-wk = 0.99, RSH2-wk = 0.67). Following the 2-week intervention, the decreased M-Vel was still observed in the post- and 4-week post-RST trials (Cohen’s d = 0.86, ≥ 0.77) in CON2-wk, while the decrease in M-Vel was absent in RSH2-wk. In comparison with corresponding pre-RSH value, significant increases in M-Vel were found in the 2nd to 4th sets of the post- and 4-week post-RSH trials in RSH2-wk (Cohen’s d ≥ 1.18, ≥ 1.06). M-Vel did not increase in CON2-wk post intervention.
In pre-RST trial, M-Hf and M-Po (Fig. 2c, d) during the RSAIEP decreased markedly from the 1st set of the RSA test in both CON2-wk and RSH2-wk (Cohen’s d ≥ 0.89, ≥ 0.94). The declines in the two variables did not occur post RSH in RSH2-wk, while the decrease in M-Po was still observed in CON2-wk (Cohen’s d ≥ 0.97). In comparison with the corresponding pre-RST value, significant increase in M-Hf and M-Po in the 2nd to 4th sets of the RSA test were found in RSH2-wk (Cohen’s d ≥ 0.93), but not in CON2-wk. The increased post-RST M-Hf and M-Po in RSH2-wk were significantly greater than the corresponding CON2-wk values (Cohen’s d ≥ 0.92). Four weeks after the intervention, the two increased variables diminished, returning to pre-RST level. Marked decrease in M-Hf and M-Po during the RSAIEP recurred in the 4-week post-RSH trial in both CON2-wk and RSH2-wk (Cohen’s d ≥ 0.76, ≥ 0.93) despite the variables in selected timepoints were still greater than corresponding pre-RSH or CON values (Cohen’s d ≥ 1.08).
RSH5-wk vs RSH2-wk
In consistent with RSH2-wk, post-RSH \(\dot{V}\)O2max and maximal sprint velocity in RSH5-wk did not change, while the performance of the Yo-Yo IR1 following the 5-week RSH improved significantly (Cohen’s d, post-RSH = 0.89, 4-week post-RSH = 0.58, Table 3). The improvements, either in post-RSH or 4-week post-RSH trial, did not differ between the two RSH groups.
The increase in WTot reported in the RSH2-wk during the RSAIEP in the post-RSH, but not the 4-week post-RSH, trial was also observed in the RSH5-wk (Cohen’s d = 0.67), and the changes between the two RSH groups were not different. Moreover, the differences in ΔLa and s-RPE among the pre-, post- and 4-week post-RSH trials and across the RSH2-wk and RSH5-wk were also not significant. Nonetheless, increased post-exercise HR in the post-RSH and 4-week post-RSH trials were recorded in the RSH5-wk (Cohen’s d = 11.4, 11.1, Table 4).
In RSH5-wk, the changes in the four RSA variables across the four sets of the RSA test during the pre-RSH RSAIEP were in line with those reported in RSH2-wk (Fig. 2a–d). Furthermore, the increases in P-Vel and M-Vel post RSH (Cohen’s d ≥ 0.98, ≥ 1.09), as well as the persistence of the two RSA variables throughout the RSAIEP in the post- and 4-week post-RSH trials, that were recorded in RSH2-wk, were also observed in RSH5-wk, and the increased P-Vel and M-Vel were not different between the two groups. For the M-Hf and M-Po, the increases in the two RSA variables post RSH in RSH5-wk (Cohen’s d ≥ 1.52, ≥ 1.41), as well as their lack of decline throughout the RSAIEP in the post-RSH trial were consistent with those in RSH2-wk. The increased M-Hf and M-Po did not differ between the two groups. Nonetheless, the recurrence of the decrease in M-Hf and M-Po, that occurred in the 4-week post-RSH trial in RSH2-wk, was not observed in RSH5-wk despite the differences in M-Hf and M-Po in the 4-week post-RSH trial were not significant between the two groups.
Discussion
This study was designed to investigate whether team-sport players participate in a short-term, low-volume RST regimen (3 sessions wk−1 for 2 weeks) under hypoxia could boost up the RST effects on the RSA during an endurance-type team-sport specific intermittent exercise protocol; and whether the boosting effects on the specific RSA could be augmented by a corresponding RSH regimen with longer training duration and associated greater training volume (3 sessions wk−1 for 5 weeks). The present findings show that marked enhancement in the RSA variables and in their sustainability of best performance during the RSAIEP were noted in RSH2-wk immediately and 4 weeks following the 2-week RST regimen in hypoxic, while the alterations in the RSA in CON2-wk were not significant. Nevertheless, the immediate training effects of the 2-week RSH appeared to be diminished 4 weeks after the intervention. For the RSH carried out for 5 weeks in RSH5-wk, the enhanced RSA immediately following the hypoxic training did not differ from that of RSH2-wk, while the immediate training effects of the RSH on the RSA variables and their sustainability of best performance during the RSAIEP were well-maintained 4 weeks post training. Accordingly, the study hypothesis that 2-week RST in hypoxia would boost up the immediate and residual training effects of the corresponding normoxic RST on the RSA of team-sport players during the RSAIEP was partially supported, while the one associated to the dose effect of RSH on the RSA was challenging.
RSH2-wk vs CON2-wk
The beneficial effects of low-volume RSH have been verified repeatedly in previous studies using various RSA tests. Gatterer et al. (2015) found that eight sessions of RSH in 12 days in soccer players could enhance their meantime of 6 × 40-m sprints in a greater extent by comparing with that resulted from normoxia. Faiss et al. (2015) reported greater improvement after six sessions of RSH in 2 weeks in skiers’ ability to repeat the 10-s double-poling sprint. Furthermore, the six RSH sessions in 3 weeks was shown to benefit the enhancement of the performance of 8 × 20-m sprints in rugby players (Hamlin et al. 2017). To the best of our knowledge, the present study is the first randomized-controlled investigation demonstrating the boosting effects of a short-term, low-volume RSH regimen on the enhancement of RSA of team-sport players during a protocol used for prolonged intermittent-type sport simulation. In comparison with the RST under normoxia, it was found that the six sessions of RSH held in 2 weeks could enhance the players’ RSA to a greater extent, particularly revealing in the M-Vel, M-Hf, and M-Po, and eventually allowed them to sustain the best sprint performance throughout the RSAIEP. The greater enhancement of the RSA in RSH2-wk than CON2-wk was in line with the alterations in the Yo–Yo IR1 performance in the two groups. It is known that the Yo–Yo test is with high reliability in evaluating the ability of the players to perform intense football-specific repeated high-intensity run (Bangsbo and Mohr 2012). The corresponding changes in the performances of the RSA and Yo–Yo test following the 2-week RSH might be empirical evidence to support the potentiality of the specific RSH regimen in acutely boosting up players’ repeated-sprint capacity in endurance-type team sports.
Following the RSH in RSH2-wk, players’ maximal velocity in the 4-s sprint and \(\dot{V}\)O2max did not increase significantly. These are in accordance with the previous notions that the boosting effects of RSH were evident mainly in athletes’ sustainability of the best sprint performance during repeated sprints rather than the peak performance of a single bout of the repeated sprints or their \(\dot{V}\)O2max (Brocherie et al. 2017). The lack of alteration in the maximal sprint velocity, which highly depends upon the capacity for using high-energy phosphates (Serresse et al. 1988), might partly associate with the less improvement in P-Vel during the post-RSH RSAIEP. It also reflected that the markedly increase in M-Vel recorded during the repeated-sprint protocol was not likely to be the result of augmentation of corresponding P-Vel. For the negligible change in \(\dot{V}\)O2max, it was concomitant with the increases in WTot, M-Hf and M-Po during the post-RSH RSAIEP with no changes in ΔLa, and s-RPE, suggesting that the extra enhancement of the RSA at sea-level following the RSH was possibly to be the results of the potential adaptive mechanisms emerged in skeletal muscles. Indeed, the long-term severe challenge imposed on the functional reserve of O2 diffusing capacity in fast-twitch fibres (FT) during RSH have been shown to induce maximal compensatory vasodilation and angiogenesis to increase the microvascular O2 delivery of the muscles (Casey and Joyner 2012; Faiss et al. 2013; Hellsten and Hoier 2014). Such physiological adaptations to RSH inevitably augment the O2 utilization and improve the removal of waste metabolites in FT, allowing them to behave more closely to their oxidative efficient slow-twitch counterparts, and eventually facilitating the resynthesis of phosphocreatine following every all-out sprint (Cleland et al. 2012). These peripheral changes in addition of the beneficial adaptations arise through oxygen-sensing pathways (i.e., increases in vascularization and acid–base regulatory capacity), and up-regulation of transcriptional factors involved in O2-signaling and O2-carrying capacity might have contributed to the RSH-resulted augmentation of RSA (Millet et al. 2019).
Four weeks following the RSH, the sustainability of the best performance in M-Hf and M-Po that had been observed in the post-RSH trial throughout the RSAIEP declined, although the RSA variables at selected timepoints were still higher than the corresponding pre-RSH or control values. The declines in the M-Hf and M-Po suggested that the immediate training effects of the 2-week RSH appeared to be diminished 4 weeks after the intervention. Brocherie et al. (2018) have shown that the transcriptional regulations in skeletal muscles triggered by 14 days of passive normobaric hypoxic exposure with the addition of six sessions of RSH returned to baseline levels by 3-week post-intervention. The associated adaptations in blood perfusion and O2 extraction in the FT which are reliant on regular hypoxic stress to maintain genetic expression were inevitably reduced, and eventually attenuated the boosted-up performance of the muscles (Hamlin et al. 2017). Nevertheless, Yo–Yo IR1 performance in the 4-week post-RST trial did not fall concomitantly from the post-RSH level. This was in line with the RSH-enhanced M-Vel that was well-maintained throughout the 4-week post-RST RSAIEP, although sprinting acceleration has been shown to be associated with the ability to produce and apply high levels of force in the horizontal direction (Hermosilla-Palma et al. 2022). Our current findings could not clearly explain the different responses in the RSA variables. Speculatively, the impact on the central motor drive during the RSH, independent of the muscular adaptations that were favorable to FT force output, might have up-regulated musculoskeletal stiffness, potentially leading advantages to stride frequency and associated velocity of the repeated sprints and the maximal intermittent run (Bishop and Girard 2013).
RSH5-wk vs RSH2-wk
In comparison with RSH2-wk, the augmented training volume by lengthening the training duration in RSH5-wk did not lead to marked greater enhancements in the RSA variables [average of increases from pre-RST levels in four RSA tests in RSH5-wk vs RSH2-wk: P-Vel 4.2% (range 1.6–6.1%) vs 5.1% (3.3–6.7%); M-Vel 6.0% (2.4–8.7%) vs 7.3% (4.7–9.5%); M-Hf 10.2% (4.9–14.7%) vs 7.5% (2.8–10.6%); M-Po 16.3% (7.5–23.5%) vs 13.7% (6.8–18.1%), p > 0.05]. Although the enhancement of the Yo–Yo IR1 performance tended to be greater following the 5-week RSH (22.2% vs 18.3%, p > 0.05), the difference did not achieve the significance level. The trivial differences between the two training regimens in the responses of the RSA and the Yo–Yo IR1 performance to the RSH implied that most of the 5-week RSH-induced alterations in the players’ RSA were accomplished within the six sessions held in the first 2 weeks. The lack of marked contribution from the training sessions in later 3 weeks to their RSA leads to postulations that the up-regulation process in the skeletal muscle adaptation to the RSH and associated augmented perfusion and O2 extraction in FT plateaued out in the first 2 weeks of the 5-week RSH, or there might be factors limiting players’ RSA performance despite possible greater adaptations had been induced in FT after the relative prolonged intervention. The possible factors, such as various neurally mediated mechanisms in working musculatures as well as their motor unit recruitment strategies, which are independent of muscle metabolism, have been shown critical in fatigue resistance over repeated sprints (Girard et al. 2011). Nonetheless, one should note that the 2-week RSH had boosted up the players’ sustainability of the best sprint performance efficaciously throughout the RSAIEP. We, therefore, could not exclude the possibility that the duration of ~ 30 min of the RSAIEP adopted in the present study might have not adequately to demonstrate the potential superiority of the 5-week RSH in sustaining the best sprint performance. This speculation was further supported by the evidence of the recurrence of the declines of the M-Hf and M-Po that was only observed in the 4-week post-RSH trial of RSH2-wk, but not in that of RSH5-wk. The present findings could not clearly explain the discrepancies between the two RSH regimens in the maintenance of the residual boosting effects on players’ RSA during the RSAIEP. Nevertheless, we noted that the M-Hf and M-Po augmented greatly during the post-RSH RSAIEP in RSH5-wk, suggesting that there might be a considerable reserve in musculature in counteracting the inevitable diminution of the RSH-induced adaptations in consequence of the removal of the hypoxic stimulations in the 4 weeks following the intervention. The marked augmentations of the M-Hf and M-Po might have been entailed from the more desirable physiological adaptations in musculature resulting from the relative greater training volume in the 5-week RSH (Bishop et al. 2019). Nevertheless, we should not neglect the possibility that the prolonged RSH on non-motorized treadmill in RSH5-wk, in comparison with RSH2-wk, might have favoured the morphological and neurological adaptations in players’ leg muscles to increase greater strength that might benefit fatigue resistance during the 4-week post-RSH RSAIEP (Folland and Williams 2007; Franks et al. 2012). Moreover, the enhanced RSA in the post- and 4-week post-RSH trials might have also due to players’ concurrent sport-team training. Nonetheless, the possible influence of the sport-team training was thought to be trivial based on the fact that marked changes in the RSA variables had never been observed in CON2-wk. Regardless, the residual boosting effects of the 5-week RSH on the RSA that could be maintained for at least 4 weeks post training, in a practical sense, are advantageous to players in optimizing their conditioning manoeuvre particularly during pre-season preparatory phase.
Limitations
In the present study, there are some limitations deserve discussion. The duration of ~ 30 min of the RSAIEP appeared to be not adequate to fully reveal the potential differences in the time course of the RSA variables of players, especially in the post-RSH trial, among experimental groups. A team-sport-specific intermittent exercise protocol last for 45 min or longer may possibly increase its discriminative power in examining the within- and between-group differences in the RSA variables among experimental trials. Moreover, the lack of normoxic control group for the 5-week intervention could not identify the net beneficial effects of hypoxia during the RSH on player’s RSA. Yet the comparison of the training effects of RSH between RSH5-wk and RSH2-wk in the present study could demonstrate the characteristics of the two RSH regimens for which the information would assist sport-team coaches in optimizing the conditioning of players using different RSH regimens in different phases of a training year. Furthermore, the sprints performed on the treadmill during the RSA tests were linear in nature, unlike those sprints performed during a real game with multiple changes of direction. To include an additional test specifically designed to assess the repeated sprinting ability when changing direction may improve the relevance of the study outcomes to a game situation. Besides, this study did not provide sufficient evidence about the relevant RSH-induced structural and molecular changes in skeletal muscles, the mechanisms referred for elucidating our findings are postulated. Related measurements are suggested to be included in future studies. Finally, the present findings of RSA in response to the two RSH regimens were obtained from male collegiate athletes during pre-season phase, the applications of the current findings as guidelines in writing a training plan for the purpose of in-season conditioning in elite professional athletes, or in female athletes who had been demonstrated with arterial O2 desaturation to be less sensitive to hypoxic stimuli (Billaut and Smith 2009), should be with cautions. Further investigations aimed at the responses of these special populations to the RSH during competition period are suggested.
In conclusion, 2-week and 5-week RST under hypoxia could comparably boost up the effects of the RST on the performance of multiple RSA tests held during a team-sport-specific intermittent treadmill exercise protocol in men’s players immediate post training. Four weeks from the last training session of the 2-week RSH, the boosting effects on the players’ RSA appeared to be diminished, although selected RSA variables were still higher than the corresponding pre-training or normoxic-control levels. In contrast, the 4-week residual training effects of the 5-week RSH could be well-maintained at immediate post training levels. The present findings suggest that six sessions of RSH held in 2 weeks may act as a reliable shock microcycle training regimen in prolonged intermittent-type team sports to boost up players’ RSA by at most 4 weeks. For the 5-week RSH regimen, the relative long-term maintenance of the training effects on the RSA of team-sport players may facilitate them in building up repeated-sprint foundation during preparatory phase before competition season.
Data availability
The data sets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Code availability
Not applicable.
Abbreviations
- ANOVA:
-
Analysis of variance
- AU:
-
Arbitrary units
- CON2-wk :
-
Control group received repeated-sprint training in normoxia for 2 weeks
- FT:
-
Fast-twitch fibres
- HR:
-
Exercise heart rate
- HRmax :
-
Maximum heart rate
- M-Hf:
-
Mean horizontal force
- M-Po:
-
Mean power output
- M-Vel:
-
Mean velocity
- P-Vel:
-
Peak velocity
- RSA:
-
Repeated-sprint ability
- RSAIEP :
-
Team-sport-specific intermittent exercise protocol
- RSH:
-
Repeated-sprint training in hypoxia
- RSH2-wk :
-
Experimental group received repeated-sprint training in hypoxia for 2 weeks
- RSH5-wk :
-
Experimental group received repeated-sprint training in hypoxia for 5 weeks
- RST:
-
Repeated-sprint training
- SpO2 :
-
Peripheral capillary O2 saturation
- s-RPE:
-
Session rating of perceived exertion
- TRmax :
-
Maximum treadmill braking resistance
- \(\dot{V}\)Emax :
-
Maximum minute ventilation
- \(\dot{V}\)O2max :
-
Maximum oxygen uptake
- WTot :
-
Total work done
- Yo–Yo IR1:
-
Yo–Yo intermittent recovery test-level 1
- ΔLa:
-
Change in blood lactate
- ηρ 2 :
-
Partial eta squared
References
Bangsbo J, Mohr M (2012) Fitness testing in football: fitness training in soccer II. (Fitness training in soccer). Bangsbosport.
Beard A, Ashby J, Chambers R, Brocherie F, Millet GP (2019a) Repeated-sprint training in hypoxia in international rugby union players. Int J Sports Physiol Perform 14:850–854
Beard A, Ashby J, Kilgallon M, Brocherie F, Millet GP (2019b) Upper-body repeated-sprint training in hypoxia in international rugby union players. Eur J Sport Sci 19:1175–1183
Billaut F, Smith K (2009) Sex alters impact of repeated bouts of sprint exercise on neuromuscular activity in trained athletes. Appl Physiol Nutr Metab 34:689–699
Bishop DJ, Girard O (2013) Determinants of team-sport performance: implications for altitude training by team-sport athletes. Br J Sports Med 47(Suppl 1):i17-21
Bishop DJ, Botella J, Granata C (2019) CrossTalk opposing view: exercise training volume is more important than training intensity to promote increases in mitochondrial content. J Physiol 597:4115–4118
Borg G, Ljunggren G, Ceci R (1985) The increase of perceived exertion, aches and pain in the legs, heart rate and blood lactate during exercise on a bicycle ergometer. Eur J Appl Physiol 54:343–349
Brocherie F, Girard O, Faiss R, Millet GP (2015) High-intensity intermittent training in hypoxia: a double-blinded, placebo-controlled field study in youth football players. J Strength Cond Res 29:226–237
Brocherie F, Girard O, Faiss R, Millet GP (2017) Effects of repeated-sprint training in hypoxia on sea-level performance: a meta-analysis. Sports Med 47:1651–1660
Brocherie F, Millet GP, D’Hulst G et al (2018) Repeated maximal-intensity hypoxic exercise superimposed to hypoxic residence boosts skeletal muscle transcriptional responses in elite team-sport athletes. Acta Physiol (oxf) 222(1):e12851
Casey DP, Joyner MJ (2012) Compensatory vasodilatation during hypoxic exercise: mechanisms responsible for matching oxygen supply to demand. J Physiol 590:6321–6326
Cleland SM, Murias JM, Kowalchuk JM et al (2012) Effects of prior heavy-intensity exercise on oxygen uptake and muscle deoxygenation kinetics of a subsequent heavy-intensity cycling and knee-extension exercise. Appl Physiol Nutr Metab 37:138–148
Cohen J (1988) Statistical power analysis for the behavioral sciences, 2nd edn. Lawrence Erlbaum Associates, Hillsdale, MI
Faiss R, Léger B, Vesin JM et al (2013) Significant molecular and systemic adaptations after repeated sprint training in hypoxia. PLoS ONE 8:e56522
Faiss R, Willis S, Born DP et al (2015) Repeated double-poling sprint training in hypoxia by competitive cross-country skiers. Med Sci Sports Exerc 47:809–817
Ferguson CJ (2009) An effect size primer: a guide for clinicians and researchers. Prof Psychol Res Pr 40:532–538
Ferrari Bravo D, Impellizzeri FM, Rampinini E et al (2007) Sprint vs. interval training in football. Int J Sports Med 29:668–674
Folland JP, Williams AG (2007) The adaptations to strength training: morphological and neurological contributions to increased strength. Sports Med 37:145–168
Foster C, Florhaug JA, Franklin J et al (2001) A new approach to monitoring exercise training. J Strength Cond Res 15:109–115
Franks KA, Brown LE, Coburn JW, Kersey RD, Bottaro M (2012) Effects of motorized vs non-motorized treadmill training on hamstring/quadriceps strength ratios. J Sports Sci Med 11:71–76
Galvin HM, Cooke K, Sumners DP, Mileva KN, Bowtell JL (2013) Repeated sprint training in normobaric hypoxia. Br J Sports Med 47(Suppl 1):i74-79
Gamble P (2006) Periodization of training for team sports athletes. Strength Cond J 28:56–66
Gatterer H, Klarod K, Heinrich D et al (2015) Effects of a 12-day maximal shuttle-run shock microcycle in hypoxia on soccer specific performance and oxidative stress. Appl Physiol Nutr Metab 40:842–845
Girard O, Mendez-Villanueva A, Bishop D (2011) Repeated-sprint ability - part I: factors contributing to fatigue. Sports Med 41:673–694
Hamlin MJ, Olsen PD, Marshall HC, Lizamore CA, Elliot CA (2017) Hypoxic repeat sprint training improves rugby player’s repeated sprint but not endurance performance. Front Physiol 8:24
Hellsten Y, Hoier B (2014) Capillary growth in human skeletal muscle: physiological factors and the balance between pro-angiogenic and angiostatic factors. Biochem Soc Trans 42:1616–1622
Hermosilla-Palma F, Loro-Ferrer JF, Merino-Muñoz P et al (2022) Changes in the mechanical properties of the horizontal force-velocity profile during a repeated sprint test in professional soccer players. Int J Environ Res Public Health 20:704
Millet GP, Girard O, Beard A, Brocherie F (2019) Repeated sprint training in hypoxia - an innovative method. Dtsch Z Sportmed 70:115–122
Mohr M, Krustrup P, Bangsbo J (2005) Fatigue in soccer: a brief review. J Sports Sci 23:593–599
Nie J, Tong TK, Zhou Y et al (2022) Cardiac autonomic disturbance following resistance and sprint-interval exercises in non-obese and obese young men. Appl Physiol Nutr Metab 47:949–962
Plisk SS, Stone MH (2003) Periodization strategies. Strength Cond J 25:19–37
Ross A, Leveritt M (2001) Long-term metabolic and skeletal muscle adaptations to short-sprint training: implications for sprint training and tapering. Sports Med 31:1063–1082
Serresse O, Lortie G, Bouchard C, Boulay MR (1988) Estimation of the contribution of the various energy systems during maximal work of short duration. Int J Sports Med 9:456–460
Sirotic AC, Coutts AJ (2008) The reliability of physiological and performance measures during simulated team-sport running on a non-motorised treadmill. J Sci Med Sport 11:500–509
Tong TK, Fu FH, Chow BC (2001) Nostril dilatation increases capacity to sustain moderate exercise under nasal breathing condition. J Sports Med Phys Fitness 41:470–478
Tong TK, Baker JS, Zhang H, Kong Z, Nie J (2019) Effects of specific core re-warm-ups on core function, leg perfusion and second-half team sport-specific sprint performance: a randomized crossover study. J Sports Sci Med 18:479–489
Tong TK, Tao ED, Chow BC, Baker JS, Jiao JJ (2021) Acute performance responses to repeated treadmill sprints in hypoxia with varying inspired oxygen fractions, exercise-to-recovery ratios and recovery modalities. Eur J Appl Physiol 121:1933–1942
Turner AN, Stewart PF (2013) Repeat sprint ability. Strength Cond J 35:37–41
Zois J, Bishop D, Fairweather I, Ball K, Aughey RJ (2013) High-intensity re-warm-ups enhance soccer performance. Int J Sports Med 34:800–805
Funding
This research was funded by Macao Polytechnic University (Grant No. RP/FCSD-03/2022).
Author information
Authors and Affiliations
Contributions
Conception and design of research: TKT, QS and ZK; acquisition of data: QS, TKT, and JN; formal analysis of data: TKT and QS; interpretation of data: QS, TKT, JN, HF, XT and ZK; writing of the original draft: TKT, QS, JN and ZK; review and editing of manuscript: QS, TKT, JN, HZ, XT and ZK; supervision of research: QS, TKT and ZK.
Corresponding author
Ethics declarations
Conflict of interest
No conflicts of interest, financial or otherwise, are declared by the authors.
Ethical approval
Ethical approval for this study was obtained from the Committee on the Use of Human and Animal Subjects in Teaching and Research at Macao Polytechnic University. The study was conducted in accordance with the Declaration of Helsinki.
Consent to participate and publication
Informed consent was obtained from all individual participants included in the study.
Additional information
Communicated by Guido Ferretti.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Shi, Q., Tong, T.K., Nie, J. et al. Repeated-sprint training in hypoxia boosts up team-sport-specific repeated-sprint ability: 2-week vs 5-week training regimen. Eur J Appl Physiol 123, 2699–2710 (2023). https://doi.org/10.1007/s00421-023-05252-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-023-05252-x