
Abstract
Purpose
Data regarding decompression stress after deep closed-circuit rebreather (CCR) dives are scarce. This study aimed to monitor technical divers during a wreck diving expedition and provide an insight in venous gas emboli (VGE) dynamics.
Methods
Diving practices of ten technical divers were observed. They performed a series of three consecutive daily dives around 100 m. VGE counts were measured 30 and 60 min after surfacing by both cardiac echography and subclavian Doppler graded according to categorical scores (Eftedal–Brubakk and Spencer scale, respectively) that were converted to simplified bubble grading system (BGS) for the purpose of analysis. Total body weight and fluids shift using bioimpedancemetry were also collected pre- and post-dive.
Results
Depth-time profiles of the 30 recorded man-dives were 97.3 ± 26.4 msw [range: 54–136] with a runtime of 160 ± 65 min [range: 59–270]. No clinical decompression sickness (DCS) was detected. The echographic frame-based bubble count par cardiac cycle was 14 ± 13 at 30 min and 13 ± 13 at 60 min. There is no statistical difference neither between dives, nor between time of measurements (P = 0.07). However, regardless of the level of conservatism used, a high incidence of high-grade VGE was detected. Doppler recordings with the O’dive were highly correlated with echographic recordings (Spearman r of 0.81, P = 0.008).
Conclusion
Although preliminary, the present observation related to real CCR deep dives questions the precedence of decompression algorithm over individual risk factors and pleads for an individual approach of decompression.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Although, there is no universally accepted definition, the popularity of “technical diving” has increased in the diving community over the last 20 years (Mitchell and Doolette 2013). This term encompasses all kind of diving beyond the generally accepted limits of 40 m for recreational diving. According to the NOAA, it includes deep (in the range of 50–140 m, sometimes even deeper), decompression, mixed-gas, and multi-gas diving for non-professional purpose (Mixed-gas diving 2017).
These deeper and longer dives translate into an increased risk of decompression sickness (DCS) (Lundell et al. 2019; Peddie and Watson 2020). Indeed, technical divers use decompression tools, whose functioning is based on predictive models that are made operational through algorithms whose aim is to deal with the gas and vascular gas emboli (VGE) load. However, most of these models, simple or complex, owe their functioning not so much to an underlying theory, but to data fitting (Angelini 2018). Indeed, validated decompression procedures are the results of human dive trial in which both risks factors for DCS, and dive outcomes are well-documented. Then, if the dive profile falls within the range of operational validity of a specific model, the resulting decompression schedule may be used with a fair degree of safety. This is, however, not the case for technical divers as depths and decompression schedules are well outside of the range of any testing. Even more, many modifications to the decompression schedule, implemented by technical divers, such as gradient factors or deep stops, have not been validated by any human dive trials (Doolette and Mitchell 2013). Although several thousand dives are reported to have been conducted safely in the field, one cannot assume a similar degree of confidence without proper data gathering (Imbert et al. 2019; Buzzacott et al. 2014), It has indeed already been demonstrated that technical diving in open circuit up to 70 m is associated with a high decompression stress (Ljubkovic et al. 2010).
However, within technical diving, one of the most important emerging trends is the shift from open circuit diving to close-circuit rebreather (CCR) diving, which is unfortunately associated with a tenfold increased fatality rate compared to open circuit (OC) scuba diving (Fock 2013). Besides the complexity of CCRs, which means that they are more prone to failure than OC equipment, the lack of formal detailed dive planning facilitated by the availability of continuous decompression solutions produced by decompression computers might also explain these figures (Fock 2006). These are only hypothesis as available medical literature about CCR diving is scarce. Recently, one study was published on the oxidative stress caused by hyperoxic CCR diving (Bosco et al. 2018), but not much is known about VGE dynamics, which is a universally accepted predisposing condition for DCS (Wienke 2009). Indeed, regardless of the decompression algorithm used, detectable VGE may be measured after recreational, technical and (to a lesser degree) professional diving (Dunford et al. 2002). The amount of VGE is considered to be statistically related to the risk of DCS after a dive (Imbert et al. 2019).
Therefore, contributions of organizations like divers alert network (DAN) may help to better understand the consequences on the decompression stress of these extrapolations outside of the tested range. Recently, a team of researchers from DAN Europe participated in a technical diving expedition to the Red Sea whose goal was to dive unusual wrecks in the Gulf of Suez (SS Zealote—110 m of sea water (msw) or SS Dacca—125 msw for instance). Although most of the planned dives would have been placed in the “extreme exposure” category in the DCIEM decompression tables, it was not the purpose of the research team to recommend any specific diving procedure. This study only aimed to monitor divers and provide an insight of their post-dive physiological status and VGE dynamics.
Methods
The diving expedition took place from 13 to 20 March 2020, aboard the Red Sea Explorers liveaboard MV Nouran. This observational study was conducted in accordance with the Declaration of Helsinki. Ethics approval was obtained from the Bio-Ethical Committee for Research and Higher Education, Brussels (No B200-2020-088). Prior to departure, informed written consent was sought from the ten divers participating in the expedition. All divers were assessed fit to dive by their own diving medicine specialist prior to the expedition.
Diving procedures
Dives were conducted from a 36-m dive boat based out of Hurghada—Egypt. On-board facilities included continual blending of nitrox and trimix gas mixes and pure oxygen (O2). Due to the outbreak of the COVID-19 pandemic, all planned dives could not be achieved. Since no adequate medical support could have been provided in case of any diving related problem, it was decided to stop diving according to DAN Europe directions and European Committee for Hyperbaric Medicine (ECHM) guidelines. Therefore, the dives were conducted over a 5-day period only, with two dives a day (30–65 msw) with a surface interval of 3–4 h between dives on day 1 and 2, followed by 3 consecutive days with a single dive around 100 msw deep or beyond (Day 3: 64 msw; Day 4: 98 msw and Day 5: 123 msw). The first 2 days were used to accustom the whole diving team and boat crew to scientific procedures and not full data collection allowing us to perfect the installation work, but also to allow divers to fine tune their set-ups and procedures.
Typically, a dive briefing was conducted before the dive on each of six wreck sites. Then, divers were dropped directly over the wreck. Weather conditions were good with daily air temperature between 25 and 30 °C, and surface water temperature between 24 and 28 °C. All dives were conducted with the help of underwater scooters.
During the dive, divers relied on their dive computers (Shearwater Petrel dive computers) with build-in ZHL-16C algorithm, to incorporate the readings from the CCR O2 cells to calculate decompression requirements. However, based on experience and utilization of dive-planning software, most divers had a fair idea of the required total dive time and final stop time for a given bottom time. Each diver had the liberty to personalize their own decompression schedule as desired, by selecting a different ‘conservatism’ by means of gradient factors (GF), determining maximum allowed super-saturation limits for the deep and shallow parts of the dive. Therefore, little formal dive planning was performed, and participants, although in team, essentially dived ‘solo’. In general, bottom time was planned on estimated decompression obligation rather than gas requirements.
All divers used JJ-CCRs rebreather (JJ-CCR ApS, Presto, Denmark) equipped with an integrated multi-gas decompression computer Petrel 2 (Shearwater Research Inc, Richmond, BC, Canada). A detailed description of the functioning of these units is beyond the scope of this article but interested readers may referred to the review by Walker and Murphy-Lavoie (2021). Basically, with a CCR, the exhaled gas is scavenged, scrubbed of carbon dioxide, enriched with oxygen, and then sent back to the diver in the breathing loop. The oxygen consumed by the diver via metabolic consumption is replaced to maintain a selected partial pressure of O2 (PPO2). All divers used a PPO2 set point of 1.3 ATA at depth and for ascent, then, for most of the divers, this was manually increased when arriving at a depth of 6 msw to be between 1.5 and 1.6 ATA (i.e., breathing 100% O2). Diluent gas for all 100 msw dives and beyond was trimix 10/70 (O2 10%, helium 70%, nitrogen 20%). All gas compositions were verified using a helium/O2 analyzer (ATA PRO, Analox, UK). All divers also carried 3–4 off-board (‘bail-out’) dive tanks to allow an independent return to the surface in the event of CCR failure. These ‘stage cylinders’ (or ‘stages’) contained either trimix, nitrox or pure oxygen depending on the decompression planning. One diver carried a second rebreather as bail-out.
Measurements
Evaluation of decompression stress and of the potential benefit of preventive measures has been done historically based on the presence or absence of clinical symptoms of DCS. However, for obvious ethical reasons, this is not acceptable in the field of recreational diving (Ozyigit et al. 2019). Although imperfect, it is now accepted that research projects can use VGE data as a surrogate endpoint (Doolette 2016; Balestra et al. 2019). Different methods of detection of VGE are possible, such as Doppler ultrasonic bubble detectors or 2D cardiac echography (Mollerlokken et al. 2016). During field studies, bubbles are usually detected in the right atrium, ventricle, and pulmonary artery. Then, the amount of detected VGE is graded according to different systems, either, categorical (Eftedal and Brubakk 1997), semi-quantitatively (Germonpre et al. 2014) or continuous (Imbert et al. 2019; Papadopoulou et al. 2018; Balestra et al. 2016).
In the present setting, two measurements were taken at 30- and 60-min post-dive. This number of measurements were limited by practical reasons. VGE signals were measured using both a portable echocardiography device (Sonosite M-Turbo, FUJIFILM Sonosite Inc, Amsterdam, The Netherlands) with a sectorial array ultrasound probe on a four-chamber view by an experienced researcher (CB), and by divers’ self-assessment using the O’Dive sensor (Doppler ultrasound signals) positioned under the clavicle and then transmitted to a smartphone equipped with the O’Dive technical application (Azoth Systems, Ollioules, France). This version of the application includes the possibility to enter various gas mixes (bottom gas, deco gas) into the data, select open or closed-circuit diving, provide gradient factors, as well as a link to upload the actual dive profile directly from the dive computer. Once synchronized, Doppler data are analyzed directly by the Azoth Systems server, according to an undisclosed protocol (Hugon et al. 2018).
The echocardiographic VGE signals over the 1 min recording were evaluated by frame-based bubble counting as described by Germonpré et al. (2014), but also scored according to the Eftedal–Brubakk categorical score (Eftedal and Brubakk 1997), while Doppler signals recording retrieved from the server were blindly reviewed to obtain a posteriori bubble grade according to the expanded Spencer scale. For the purpose of comparison and correlation testing both categorical score were converted within the simplified bubble grading system (BGS) (Marroni et al. 2004).
Since several reports suggest that post-dive dehydration could promote the development of DCS or at least modified VGE production (Blatteau et al. 2008; Fahlman and Dromsky 2006; Sengun et al. 2012; Skogland et al. 2008), subjects were weighed on an electronic device (Mini Crane Scale OCS-300, Vetek Weighing AB, Väddö, Sweden; precision ± 50 g) before and 15 min after surfacing. Simultaneously, intracellular, extracellular, and total body water were also estimated by means of multifrequency tetrapolar impedancemetry (Biody Expert system, Cagnes sur Mer, France).
Statistical analysis
After evaluation of the normality distribution with the Kolmogorov–Smirnov test, differences between pre- and post-dive measurements were assessed using either Friedman test with Dunn’s post-hoc or one-way ANOVA with Bonferroni post-hoc as appropriate for multiple comparisons and by paired t-test or Mann–Whitney for simple comparison. Correlation between echographic and O’Dive bubble grades was evaluated through a Pearson r calculation. A P value of < 0.05 was considered significant for all statistical tests. Statistical analysis was performed using GraphPad Prism version 9.1.0 for MacOS (GraphPad Software, San Diego, CA, USA).
Results
All divers were males, were declared medically fit to dive prior to the first dive and in possession of a valid diving certification (at least GUE CCR diver level 2) and insurance. They were all familiar with diving at depth of 100 msw or beyond. Characteristics of the divers are shown in Table 1.
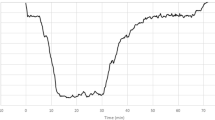
A typical recorded profile is shown in Fig. 1. Depth-time profiles of the 30 man-dives are given in Fig. 2. The average depth was 97.3 ± 26.4 msw [100 msw; 70–120] with a runtime of 160 ± 65 min [130 min; 105–207]. Run time was primarily affected by the maximal depth and bottom time but also by the level of conservatism which was altered by selecting gradient factors to modify the allowed maximum super-saturation limits) at each diver’s discretion as illustrated in Table 2.

Typical record of diving profile at a maximum depth of 120 msw and 11 min bottom time. PPO2 partial pressure of oxygen (Green line), PPHe partial pressure of helium (Brown line), PPN2 partial pressure of nitrogen (Grey line). The Black line correspond to the depth profile while the red zone illustrates the decompression ceiling

Mean and standard deviation of depth and dive time (n = 30)
There were no incidents of divers breaching their decompression profile as calculated by their dive computers. One diver developed unusual fatigue, suggestive of potential DCS, after the 6th dive; the diver chose not to be treated and continued diving for the remainder of the expedition. His symptoms resolved spontaneously. All divers flew home more than 48 h after the last dive, without developing any symptoms of DCS.
Because of technical and organizational mishaps, only seven full sets out of ten datasets were available for analysis.
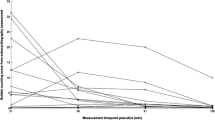
Results of the echocardiographic frame-based bubble counting are shown in Fig. 3. The mean bubble count per cardiac cycle was 14 ± 13 at 30 min and 13 ± 13 at 60 min. Because of data variability, no statistical significance was identified neither between dives, nor between times of measurement (P = 0.07, Friedman test).

Individual bubble count changes after 100 m depth dives
When converted into BGS, echographic bubble grades were highly correlated with the BGS given by Azoth System’s analysis based on the Doppler recording made (Spearman r of 0.81, P = 0.008).
Total body water was reduced by 1.0 ± 1.2 l between pre- and post-dive measurements. However, this was not statistically significant (P = 0.4, Mann–Whitney). No variation is seen in intracellular (pre: 61.8 ± 1.1 vs. post: 61.9 ± 0.9%, P = 0.4, paired t-test) and extracellular water (pre: 38.4 ± 0.7 vs. post: 38.3 ± 0.9%, P = 0.7, paired t-test) either (Fig. 4). No specific correlation was identified between BMI or hydration status and bubble grade.

Total body water (TBW), extracellular (ECW) and intracellular water (ICW) difference after one 100 msw bounce-dive to 123 msw
Discussion
Since the reconfiguration of Biomarine CCR155, one of the first mixed gas rebreathers to be adopted by sport divers in the early 1990s, the use of CCRs by recreational or technical divers has become increasingly common. This, however, comes with a cost, as the fatality rates for rebreather diving are 8–10 times higher than for open circuit diving (Fock 2013). Although the primary trigger for most of these accidents can be identified as a failure of the ‘human–machine interface’, two-thirds of fatal dives were associated with a high-risk dive or high-risk behavior such as solo diving, exceeding depth limits, or carrying insufficient gases. The latter two are directly related to decompression management, which is a major factor in diver’s safety. Unfortunately, decompression data regarding the effects of mixed-gases deeper than 70 msw are known mainly from saturation diving, which shares little similarity with bounce diving (Brubakk et al. 2014). Indeed, in saturation diving, when all the tissues are at the equilibrium, the divers may spend an indefinite period under pressure for the same decompression obligation, while in bounce-diving, there is a significative imbalance between the time spent at depth and the time spent decompressing (Doolette and Mitchell 2013). Oxygen exposure, dry decompression and ascent speed are also major differences between these two types of diving. As a result, the optimization of decompression from deep bounce dives is one of the most debated and controversial issues in technical diving, which need to be supported by field data. ‘Algorithm-validation dive trials are known to not extrapolate well to technical diving (Doolette and Mitchell 2013). Therefore, technical diving is still conducted with empirical, unvalidated models, that aim to reduce VGE load as the critical factor.
The results of this observational study suggest they may not be capable of doing so. Indeed, although the diving profile were allegedly conservative according to the decompression algorithm used, a high incidence of high-grade VGE was detected. Moreover, it seems that the deepest divers, while using similar decompression scheme, exhibit different bubbling patterns, a feature already demonstrated in an open circuit single exposure (Papadopoulou et al. 2018). More, regardless of the level of conservatism used, the amount of detectable VGE is rather constant from dive to dive. Indeed, it can be observed that VGE counts do not significantly increase with succeeding dives, despite the facts that these dives may be considered ‘provocative’ with depths repeatedly > 39 msw daily. This highlights the importance of individual factors to manage decompression safety. It must also be noted that the lone diver who developed unusual fatigue suggestive of potential DCS, owned the highest bubble grade, highest BMI and lowest fitness level among the divers who volunteered for this observational study. Although anecdotal, this might also be seen as an argument for a more diver-centric approach.
During this observational study, two individual parameters were measured, dehydration and physical status. Although animal studies have produced conflicting results, divers’ hydration state has long been considered as a critical point for decompression safety. This is partially supported among humans by a field study demonstrating that pre-dive hydration reduces VGE (Gempp et al. 2009). In this study, using a shallower profile (30 min/30 msw with a 9 min safety stop at 3 msw), in the absence of pre-hydration, the plasma volume was significantly reduced by 2.2% as well as the total body water with a mean 1.2 l, ranging from 800 to 1500 ml. In our setting, the dives were deeper and longer (160 min/100 msw) and seem to dehydrate the diver in a similar fashion (mean of 1.0 l, ranging from 500 to 2400 ml); however, there was no significant difference between pre- and post-dive measurements. Also, fluids shift between the extracellular and intracellular did not seem to occur. This might be explained by CCR technology, which uses a closed loop. It is indeed a known fact in anesthesiology that a closed-circuit conserve respiratory heat and humidity. It is also known that relationships between VGE grades and age, maximal oxygen uptake, and percent body fat might also exist. Younger, slimmer, or aerobically fitter divers produced fewer bubbles compared with older, fatter, or poorly physically fit divers (Carturan et al. 2002). Coincidentally, although declared fit to dive, the heaviest bubbler was closer to the second diver profile with some minor comorbidities than to the first description. Nonetheless, we couldn’t demonstrate such correlation among our results. More research is needed to extrapolate on this specific hypothesis.
It must be acknowledged that the number of subjects is low, so the reproducibility and power of the study cannot be ascertained. However, given the technical difficulty of retrieving exploitable data (the ideal tool being cardiac echography recordings) in the field, an easier way to gather reliable data needs to be considered. Recently, the detection of VGE in subclavian veins has been proposed and validated (Hugon et al. 2018), and a simple, do-it-yourself tool has been developed and is currently marketed. The feasibility of the O’Dive system for collection of diver’s VGE data has been recently reported (Germonpre et al. 2020). In this study, divers performed the O’Dive measurements on themselves without any problems. There appears to be an excellent correlation between the BGS reported by the O’Dive (Azoth Systems server data) and the Eftedal–Brubakk scores obtained from the echocardiography images. This would indicate that in the future, O’Dive measurements could well become a major asset in large-scale diving decompression research. For the present time however, we recommend that O’Dive data still be ‘backed’ by a validated VGE measurement.
Conclusion
In conclusion, the present observation represents an original dataset regarding VGE count related to CCR deep trimix dives performed in open sea, by technical divers. Although preliminary, it questions the precedence of decompression algorithm over individual risk factors and pleads for an individual approach of decompression. It also highlights the gap of knowledge to develop comprehensive diving guidelines regarding deep CCRs diving.
Data availability
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- BGS:
-
Simplified bubble grading system
- CCR:
-
Closed-circuit rebreather
- DAN:
-
Divers alert network
- DCS:
-
Decompression sickness
- ECW:
-
Extracellular water
- ICW:
-
Intracellular water
- OC:
-
Open circuit
- PPO2 :
-
Partial pressure of oxygen
- TBW:
-
Total body water
- VGE:
-
Vascular gas emboli
References
Angelini S (2018) Dive computer decompression models and algorithms: philosophical and practical views. Underw Technol 35(2):51–61. https://doi.org/10.3723/ut.35.051
Balestra C, Theunissen S, Papadopoulou V, Le Mener C, Germonpre P, Guerrero F, Lafere P (2016) Pre-dive whole-body vibration better reduces decompression-induced vascular gas emboli than oxygenation or a combination of both. Front Physiol 7(586):586. https://doi.org/10.3389/fphys.2016.00586
Balestra C, Germonpre P, Rocco M, Biancofiore G, Kot J (2019) Diving physiopathology: the end of certainties? Food for Thought. Minerva Anestesiol 85(10):1129–1137. https://doi.org/10.23736/S0375-9393.19.13618-8
Blatteau JE, Gempp E, Balestra C, Mets T, Germonpre P (2008) Predive sauna and venous gas bubbles upon decompression from 400 kPa. Aviat Space Environ Med 79(12):1100–1105. https://doi.org/10.3357/asem.2377.2008
Bosco G, Rizzato A, Quartesan S, Camporesi E, Mrakic-Sposta S, Moretti S, Balestra C, Rubini A (2018) Spirometry and oxidative stress after rebreather diving in warm water. Undersea Hyperb Med 45(2):191–198
Brubakk AO, Ross JAS, Thom SR (2014) Saturation diving; physiology and pathophysiology. In: Terjung R (ed) Comprehensive physiology. John Wiley & Sons Inc, Hoboken, pp 1229–1272. https://doi.org/10.1002/cphy.c130048
Buzzacott P, Lambrechts K, Mazur A, Wang Q, Papadopoulou V, Theron M, Balestra C, Guerrero F (2014) A ternary model of decompression sickness in rats. Comput Biol Med 55:74–78. https://doi.org/10.1016/j.compbiomed.2014.10.012
Carturan D, Boussuges A, Vanuxem P, Bar-Hen A, Burnet H, Gardette B (2002) Ascent rate, age, maximal oxygen uptake, adiposity, and circulating venous bubbles after diving. J Appl Physiol 93(4):1349–1356. https://doi.org/10.1152/japplphysiol.00723.1999
Doolette DJ (2016) Venous gas emboli detected by two-dimensional echocardiography are an imperfect surrogate endpoint for decompression sickness. Diving Hyperb Med 46(1):4–10
Doolette DJ, Mitchell SJ (2013) Recreational technical diving part 2: decompression from deep technical dives. Diving Hyperb Med 43(2):96–104
Dunford RG, Vann RD, Gerth WA, Pieper CF, Huggins K, Wacholtz C, Bennett PB (2002) The incidence of venous gas emboli in recreational diving. Undersea Hyperb Med 29(4):247–259
Eftedal O, Brubakk AO (1997) Agreement between trained and untrained observers in grading intravascular bubble signals in ultrasonic images. Undersea Hyperb Med 24(4):293–299
Fahlman A, Dromsky DM (2006) Dehydration effects on the risk of severe decompression sickness in a swine model. Aviat Space Environ Med 77(2):102–106
Fock A (2006) Health status and diving practices of a technical diving expedition. Diving Hyperb Med 36(4):179–185
Fock AW (2013) Analysis of recreational closed-circuit rebreather deaths 1998–2010. Diving Hyperb Med 43(2):78–85
Gempp E, Blatteau JE, Pontier JM, Balestra C, Louge P (2009) Preventive effect of pre-dive hydration on bubble formation in divers. Br J Sports Med 43(3):224–228. https://doi.org/10.1136/bjsm.2007.043240
Germonpre P, Papadopoulou V, Hemelryck W, Obeid G, Lafere P, Eckersley RJ, Tang MX, Balestra C (2014) The use of portable 2D echocardiography and ‘frame-based’ bubble counting as a tool to evaluate diving decompression stress. Diving Hyperb Med 44(1):5–13
Germonpre P, Van der Eecken P, Van Renterghem E, Germonpre FL, Balestra C (2020) First impressions: use of the Azoth Systems O’Dive subclavian bubble monitor on a live aboard dive vessel. Diving Hyperb Med 50(4):405–412. https://doi.org/10.28920/dhm50.4.405-412
Hugon J, Metelkina A, Barbaud A, Nishi R, Bouak F, Blatteau JE, Gempp E (2018) Reliability of venous gas embolism detection in the subclavian area for decompression stress assessment following scuba diving. Diving Hyperb Med 48(3):132–140. https://doi.org/10.28920/dhm48.3.132-140
Imbert JP, Egi SM, Germonpre P, Balestra C (2019) Static metabolic bubbles as precursors of vascular gas emboli during divers’ decompression: a hypothesis explaining bubbling variability. Front Physiol 10:807. https://doi.org/10.3389/fphys.2019.00807
Ljubkovic M, Marinovic J, Obad A, Breskovic T, Gaustad SE, Dujic Z (2010) High incidence of venous and arterial gas emboli at rest after trimix diving without protocol violations. J Appl Physiol 109(6):1670–1674. https://doi.org/10.1152/japplphysiol.01369.2009
Lundell RV, Arola O, Suvilehto J, Kuokkanen J, Valtonen M, Räisänen-Sokolowski AK (2019) Decompression illness (DCI) in Finland 1999–2018: special emphasis on technical diving. Diving Hyperb Med 49(4):259–265. https://doi.org/10.28920/dhm49.4.259-265
Marroni A, Bennett PB, Cronje FJ, Cali-Corleo R, Germonpre P, Pieri M, Bonuccelli C, Balestra C (2004) A deep stop during decompression from 82 fsw (25 m) significantly reduces bubbles and fast tissue gas tensions. Undersea Hyperb Med 31(2):233–243
Mitchell SJ, Doolette DJ (2013) Recreational technical diving part 1: an introduction to technical diving methods and activities. Diving Hyperb Med 43(2):86–93
Mixed-gas diving (2017). In: McFall G, Heine JN, Bozanic J (eds) NOAA diving manual, 6th edn. Best Publishing Company, Flagstaff
Mollerlokken A, Blogg SL, Doolette DJ, Nishi RY, Pollock NW (2016) Consensus guidelines for the use of ultrasound for diving research. Diving Hyperb Med 46(1):26–32
Ozyigit T, Yavuz C, Egi SM, Pieri M, Balestra C, Marroni A (2019) Clustering of recreational divers by their health conditions in a database of a citizen science project. Undersea Hyperb Med 46:171–183
Papadopoulou V, Germonpre P, Cosgrove D, Eckersley RJ, Dayton PA, Obeid G, Boutros A, Tang MX, Theunissen S, Balestra C (2018) Variability in circulating gas emboli after a same scuba diving exposure. Eur J Appl Physiol 118(6):1255–1264. https://doi.org/10.1007/s00421-018-3854-7
Peddie C, Watson J (2020) Diving incident report 2019. BSAC National Diving Committee on Diving Incident. British Sub-Aqua Club, London
Sengun S, Uslu A, Aydin S (2012) Application of multifrequency bioelectrical impedance analysis method for the detection of dehydration status in professional divers. Medicina 48(4):203–210
Skogland S, Stuhr LB, Sundland H, Olsen RE, Hope A (2008) Venous gas emboli in normal and dehydrated rats following decompression from a saturation dive. Aviat Space Environ Med 79(6):565–569. https://doi.org/10.3357/asem.2199.2008
Walker IJ, Murphy-Lavoie HM (2021) Diving rebreathers. In: StatPearls. StatPearls Publishing Copyright © 2021, StatPearls Publishing LLC, Treasure Island
Wienke BR (2009) Diving decompression models and bubble metrics: modern computer syntheses. Comput Biol Med 39(4):309–331. https://doi.org/10.1016/j.compbiomed.2008.12.013
Acknowledgements
The authors would like to sincerely thank and commend the JJ-CCR passionate divers present for their dedication during the experiments, but we could not forget the whole crew of Red Sea Explorers (Hurgada), with special attention to Faisal Khalaf and Olga Martinelli.
Funding
The authors received no funding for this work.
Author information
Authors and Affiliations
Contributions
CB, FG, and PL contributed to the study conception and design. Material preparation, data collection and analysis were performed by CB, FG, PG, PL. The first draft of the manuscript was written by CB and PL. PG and FG revised the manuscript critically for important intellectual content and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
Study approved by the he Bio-Ethical Committee for Research and Higher Education, Brussels (No B200-2020-088).
Consent for publication
Not applicable.
Additional information
Communicated by Guido Ferretti.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Balestra, C., Guerrero, F., Theunissen, S. et al. Physiology of repeated mixed gas 100-m wreck dives using a closed-circuit rebreather: a field bubble study. Eur J Appl Physiol 122, 515–522 (2022). https://doi.org/10.1007/s00421-021-04856-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-021-04856-5