
Abstract
Purpose
Findings concerning the effects of exhaustive exercise on cognitive function are somewhat equivocal. The purpose of this study was to identify physiological factors that determine executive function after exhaustive exercise.
Methods
Thirty-two participants completed the cognitive tasks before and after an incremental exercise until exhaustion (exercise group: N = 18) or resting period (control group N = 14). The cognitive task was a combination of a Spatial Delayed-Response (Spatial DR) task and a Go/No-Go task, which requires executive function. Cerebral oxygenation and skin blood flow were monitored during the cognitive task over the prefrontal cortex. Venous blood samples were collected before and after the exercise or resting period, and blood catecholamines, serum brain-derived neurotrophic factor, insulin-like growth hormone factor 1, and blood lactate concentrations were analyzed.
Results
In the exercise group, exhaustive exercise did not alter reaction time (RT) in the Go/No-Go task (pre: 861 ± 299 ms vs. post: 775 ± 168 ms) and the number of error trials in the Go/No-Go task (pre: 0.9 ± 0.7 vs. post: 1.8 ± 1.8) and the Spatial DR task (pre: 0.3 ± 0.5 vs. post: 0.8 ± 1.2). However, ΔRT was negatively correlated with Δcerebral oxygenation (r = −0.64, P = 0.004). Other physiological parameters were not correlated with cognitive performance. Venous blood samples were not directly associated with cognitive function after exhaustive exercise.
Conclusion
The present results suggest that recovery of regional cerebral oxygenation affects executive function after exhaustive exercise.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Cognitive function is one of the major determinants of performance in sports and may be impaired under exhaustive conditions. Recent studies summarized the effects of exhaustive exercise on cognitive function, but the findings are somewhat equivocal (Chang et al. 2012; McMorris 2016a). Exercise has many physiological effects on the human brain (Ide and Secher 2000; Nybo and Secher 2004; Ogoh and Ainslie 2009). Thus, several physiological factors are likely to be related to interaction between cognitive function and exhaustive exercise. In the present study, we attempted to determine physiological factors that affect cognitive function under exhaustive conditions. To this end, cognitive function was assessed after exhaustive exercise, since it is difficult to complete a cognitive task that lasts for a long time during exhaustive exercise.
Cerebral oxygenation reflects the balance between oxygen availability and utilization (Boushel et al. 2001). During incremental exercise, cerebral oxygenation measured from the prefrontal cortex increases up to moderate-to-hard intensities, then decreases at very hard intensity near exhaustion (Rooks et al. 2010). In contrast, cerebral oxygenation quickly recovers after exhaustive exercise (Ando et al. 2010; Gonzalez-Alonso et al. 2004). Provided that oxygen availability could be compromised under exhaustive condition, the degree of recovery of cerebral oxygenation may be crucial for cognitive function after exhaustive exercise. Therefore, in the present study, we first hypothesized that recovery of cerebral oxygenation is associated with cognitive function after exhaustive exercise.
Exercise affects brain circuits involving neurotransmitters including dopamine, noradrenaline, serotonin, adrenocorticotropic hormone, and cortisol (Dietrich and Audiffren 2011; McMorris 2016a; Meeusen and De Meirleir 1995; Nybo and Secher 2004). Some of these physiological changes are potential candidates that affect cognitive function (Brisswalter et al. 2002; Chmura et al. 1994; McMorris 2016a). Exhaustive exercise substantially increases circulating catecholamine concentrations (Chmura et al. 1994; Gonzalez-Alonso et al. 2004). Given that catecholamine does not readily cross the blood–brain barrier (Cornford et al. 1982), venous blood catecholamine concentrations are almost entirely the result of peripheral activity (McMorris 2016a). However, increases in circulating adrenaline and noradrenaline activate β-adrenoceptors on the afferent vagus nerve (McGaugh et al. 1996; Miyashita and Williams 2006), which terminates in the nucleus tractus solitarii (NTS) within the blood–brain barrier (McMorris 2016b). Noradrenergic cells in the NTS project to the locus coeruleus (LC) and stimulate noradrenaline synthesis and release to other parts of the brain (McMorris 2016a). Thus, increases in circulating catecholamines induced by exhaustive exercise may be critical to cognitive performance. Therefore, it is worth investigating whether cognitive performance after exhaustive exercise is associated with alterations in venous blood catecholamine concentrations. Furthermore, alternations in brain-derived neurotrophic factor (BDNF) (Lee et al. 2014; Piepmeier and Etnier 2015; Winter et al. 2007), insulin-like growth hormone factor 1 (IGF-1) (Cassilhas et al. 2012; Cotman and Berchtold 2002; Ding et al. 2006), and blood lactate (Tsukamoto et al. 2016) may be contributing factors that affect cognitive function after exercise. We also examined whether alterations in BDNF, IGF-I, and blood lactate are associated with cognitive function after exhaustive exercise.
The purpose of this study was to examine the effects of exhaustive exercise on cognitive function and to identify physiological factors that determine cognitive function. The findings from the present study extend our prior knowledge and may help to develop methods to prevent impairments in cognitive performance under exhaustive conditions.
Materials and methods
Participants
Thirty-four healthy male participants were recruited in this study. However, two participants were not able to complete cognitive task after exhaustive exercise due to total exhaustion. Thus, 32 healthy male participants completed the cognitive tasks [exercise group: N = 18, age = 23.2 ± 2.1 years; height = 1.71 ± 0.06 m; body mass = 66.8 ± 5.9 kg; peak oxygen uptake (\(\dot{V}{\text{O}}_{{2{\text{peak}}}}\)) = 48.2 ± 6.6 ml/kg/min, control group: N = 14, age = 22.3 ± 2.3 years; height = 1.70 ± 0.06 m; body mass = 64.4 ± 9.5 kg; \(\dot{V}{\text{O}}_{{2{\text{peak}}}}\) = 47.7 ± 7.4 ml/kg/min]. The participants were physically active and did not have any history of cardiovascular, cerebrovascular, or respiratory disease. All participants gave written informed consent to participation. This study was approved by the ethics committee of Fukuoka University and was in accordance with the Declaration of Helsinki.
Cognitive task
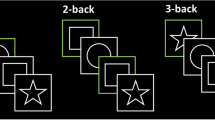
Cognitive task was a combination of Spatial Delayed Response (Spatial DR) and Go/No-Go tasks (Harada et al. 2004; Komiyama et al. 2015). The Spatial DR task required working memory, and the Go/No-Go task required response inhibition and executive control. Hence, the present cognitive task required executive function. The details of the cognitive task were previously described (Komiyama et al. 2015). Figure 1 summarizes the present cognitive task. In the Spatial DR task, a visual stimulus was presented in one of the eight locations surrounding a fixation point. The participants were asked to remember the location, where the visual stimulus was presented. Then, the Go/No-Go task was started. On each trial, one of a pair of figures was presented at the center of the computer display. One figure was identified at the outset as the target. On any given trial, if the presented figure was the target (“Go trial”), participants released a shift key as quickly as possible. If the figure was not the target (“No-Go trial”), participants continued holding the shift key down. After the Go/No-Go task, participants continued with the Spatial DR task. Visual stimuli were presented at eight locations surrounding the fixation point. The participants pressed the button on a portable ten-key pad to indicate the location that they remembered. The portable ten-key pad and computer keyboards were horizontally situated above both sides of the ergometer’s handlebars. The participants pressed the ten-key pad with their right index finger (Spatial DR task) and pressed the shift button on the keyboard with their left index finger (Go/No-Go task).

Spatial delayed response (Spatial DR) task and Go/No-Go task. At the beginning of the Spatial DR task, a visual cue was presented at one of the eight locations. The participants remembered the location during the Go/No-Go task. After the Go/No-Go task, participants responded by pressing the button of the ten-key corresponding to the remembered location. In this case, participants had to press the number 6
After the participants had completed four or five successive trials (pseudorandomly determined) in the Go/No-Go task, the other figure became the target. After the next four or five successive trials were completed, a new pair of figures was presented. The participants did not know when the correct response and the figure would be reversed or when the new pair of figures would be presented. The cognitive tasks continued until the participants had completed 20 trials of each task. To assess cognitive function, we used reaction time (RT) of the Go trial in the Go/No-Go task and number of error trials of each task. In the Go/No-Go task, error trials were defined as omitting the response in the Go trial, or an incorrect response in the No-Go trial. For calculation of number of error trials, we excluded trials immediately after the relationship between correct response and figure was reversed or one of a new pair of figures was presented. In the Spatial DR task, error trials were defined as incorrect responses to the remembered location.
Experimental procedure
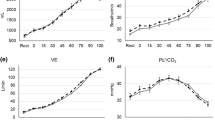
A few days before the experiment, the participants completed practice blocks of the cognitive task at rest and during cycling until RT decreased within three SD from the mean. On the day of the experiment, the participants arrived at the laboratory at least 1 h before the experiment. At the beginning of the experiment, venous blood sample was collected from the antecubital vein. The left earlobe was pricked with a safety lancet and 2 µl capillary blood was collected. Systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured from the right arm in a sitting position. Then, the participants performed the cognitive task at rest sitting on a cycle ergometer (75XLII, COMBI Wellness, Tokyo, Japan). After the cognitive task, ratings of perceived exertion (RPE; 6–20 Borg scale) (Borg 1975) were recorded. In the exercise group, the participants started an incremental exercise test until exhaustion. Following a warm-up period at 10 W for 1 min, the maximal exercise test was initiated with 20 W increments every minute in a ramp manner. The pedaling rate was freely chosen over 50 revolution per minute (rpm) by each participant. The maximal exercise test was stopped when the participants were no longer able to maintain a pedaling rate of 50 rpm. We measured ventilatory parameters using a gas analysis system (ARCO-2000, ARCO System, Chiba, Japan), and peak oxygen uptake was determined as the highest oxygen uptake attained. RPE was recorded after the cessation of exercise. The participants performed the cognitive task 2 min after the maximal exercise test. Then, venous and capillary blood sample was collected, followed by blood pressure measurement. In the control group, the participants completed the measurement in the same manner except for exercise. We used the average time (16 min 1 s) of the maximal exercise in the exercise group as the duration of resting period in the control group. Thus, the experiments in the control group were conducted after all experiments in the exercise group had completed. The participants in the control group also performed the incremental exercise test until exhaustion within a week after the main experiment and confirmed that \(\dot{V}{\text{O}}_{{2{\text{peak}}}}\) was not different between groups (P = 0.86, two-sample t test). Throughout the experiment, the ambient temperature was maintained at 22 °C and the relative humidity was controlled approximately at 50%.
Measurement
Cerebral oxygenation was continuously monitored over the prefrontal cortex with a near-infrared spectroscopy (NIRS) (BOM-L1 TRW, Omegawave, Tokyo, Japan), as previously described (Ando et al. 2010). A probe holder contained one light source probe and two detectors placed at 2 cm (detector 1) and 4 cm (detector 2) from the source. The probe holder was attached at the right side of the forehead, so that midpoint of the detectors covers the Fp2 position of the international electroencephalographic 10–20 system. We used positions of Fpz and F8 as landmarks. The source generated three wavelengths of near-infrared light (780, 810, and 830 nm). Based on the modified Beer–Lambert law, continuous measurement of concentration changes in oxyhemoglobin (oxy-Hb) and deoxyhemoglobin (deoxy-Hb), and tissue scattering and attenuation coefficients were measured with the three wavelengths of near-infrared light. After movement artifacts were removed, hemoglobin concentrations were calculated using near-infrared light received by each detector without detrend. Total hemoglobin (total-Hb) is calculated as the sum of oxy-Hb and deoxy-Hb. Cerebral oxygenation is expressed as oxy-Hb/total-Hb × 100 (i.e., as a percentage). Hence, cerebral oxygenation reflects proportion of oxy-Hb, and the definition of cerebral oxygenation is different from other studies using different devices (e.g., Tobias et al. 2008). We assessed relative changes in cerebral oxygenation from the baseline in response to exhaustive exercise and the cognitive tasks. In the present study, the hemoglobin concentrations received by detector 1 were subtracted from those received by detector 2, which allowed us to reduce effects of near-surface blood flow on hemoglobin concentrations in the cortical tissue (see also limitation in “Discussion”).
Skin blood flow was monitored from the right side of the forehead with a laser Doppler flow probe (FLO-C1, Omegawave, Tokyo, Japan). The probe of skin blood flow was placed side by side with the probe of NIRS, and both probe holders were wrapped by a black cloth to shield them from the light. Before the experiment, we confirmed that there was no cross-talk when we measured cerebral oxygenation and skin blood flow simultaneously. Before the cognitive task at rest, we measured averaged oxy-Hb, deoxy-Hb, total-Hb, cerebral oxygenation, and skin blood flow for 30 s as a baseline while sitting on the ergometer. Oxy-Hb, deoxy-Hb, total-Hb, and cerebral oxygenation during the cognitive tasks were averaged and expressed relative to the baseline. Relative changes in skin blood flow were expressed as a percentage.
Plasma samples were obtained from heparinized blood samples at centrifugation at 3000 rpm for 15 min and stored at −80 °C until analysis. Plasma adrenaline, noradrenaline, and dopamine concentrations were determined using a high-performance liquid chromatography system (Shimadzu, Kyoto, Japan). Relative changes in adrenaline, noradrenaline, and dopamine were expressed as a percentage. Serum samples were obtained from venous blood by centrifugation and were stored until analysis. Serum BDNF concentration was measured using the Quantikine Human BDNF Immunoassay (R&D systems, Minneapolis, USA). For BDNF analysis, data from one participant in the control group were excluded due to technical problem. Serum IGF-1 concentration was determined using an immunoradiometric assay (IGF-1 IRMA Daiichi, TFB, Tokyo, Japan) and a Wallac 1460 Gamma Counter (Wallac, Turku, Finland). Blood lactate concentration was determined by the lactate oxidase method, using an automated analyzer (Lactate Pro, Arkray, Kyoto, Japan).
Data and statistical analysis
Two-way analysis of variance (ANOVA) with time (pre and post) as the within-subject factor and group as the between-subject factor was performed. When an interaction was observed, we performed a paired t test with Bonferroni correction. Sample size was calculated from our preliminary results and we observed that, at least, 13 participants would be needed. We performed the Shapiro–Wilk test before correlation analysis to test if data are normally distributed. Pearson’s correlation test was used to establish a correlation between alterations in cognitive performance and physiological parameters when data are normally distributed. Spearman’s correlation test was used when data are not normally distributed. For correlation analysis, provided p values were corrected with false-discovery rate correction (Glickman et al. 2014) for each physiological variable. All data are expressed as mean ± SD. The significance level was set at P < 0.05.
Results
Cognitive function
Figure 2 illustrates RT in the Go/No-Go task (A), number of error trials in the Go/No-Go (B), and the Spatial DR (C) tasks. We observed no significant main effects of time [F(1,30) = 1.33, P = 0.26, η 2p = 0.04] and group [F(1,30) = 0.02, P = 0.88, η 2p = 0.001] on RT. No interaction was observed between time and group [F(1,30) = 1.02, P = 0.32, η 2p = 0.03]. These results indicate that RT did not change in the exercise (pre: 861 ± 299 ms vs. post: 775 ± 168 ms) and control (pre: 833 ± 234 ms vs. post: 827 ± 221 ms) groups. In contrast, we found a significant interaction between time and group on number of error trials in the Go/No-Go task [F(1,30) = 7.43, P = 0.01, η 2p = 0.20]. The difference in number of error trials in the Go/No-Go task was not significant in the exercise (pre: 0.9 ± 0.7 vs. post: 1.8 ± 1.8, P = 0.04) and control (pre: 1.0 ± 0.8 vs. post: 0.6 ± 0.6, P = 0.06) groups after Bonferroni correction. Error trials in the Spatial DR task was affected by neither time [F(1,30) = 1.44, P = 0.24, η 2p = 0.05] nor group [F(1,30) = 3.13, P = 0.09, η 2p = 0.09], which indicates that accuracy of the Spatial DR task was not altered in both groups.

Reaction time (a) and number of error trials in the Go/No-Go (b) and Spatial DR tasks (c) in the exercise and control groups
Physiological parameters
Figure 3 illustrates an example of alterations in cerebral oxygenation and skin blood flow in the exercise group. Cerebral oxygenation gradually increased during low-to-moderate exercise, then decreased until exhaustion. Nevertheless, cerebral oxygenation quickly recovered after the cessation of exercise, and recovered to the baseline level during the cognitive task. In contrast, skin blood flow increased during incremental exercise until exhaustion, and remained elevated after exercise.

Example of alterations in cerebral oxygenation (a) and skin blood flow (b). Black bars show the duration of the cognitive task. Gray bars show the duration of the incremental exercise. Horizontal dashed lines indicate the respective baselines. Note that data were resampled for clarification
Table 1 summarizes the results of physiological parameters. In the exercise group, we found no differences in oxy-Hb, deoxy-Hb, total-Hb, and cerebral oxygenation between pre- and post-values. In contrast, skin blood flow increased after exercise (P = 0.003), showing that skin blood flow remained elevated during the cognitive task after exhaustive exercise. Plasma adrenaline, noradrenaline, and dopamine concentrations significantly increased after exercise (P = 0.03, P < 0.001, and P < 0.001). Serum BDNF did not change after exercise, whereas serum IGF-1 significantly increased after exercise (P < 0.001). Blood lactate concentration and RPE significantly increased after exercise (P < 0.001 and P < 0.001). DBP slightly but significantly decreased after exercise (P = 0.02). In the control group, we found no alterations in physiological parameters between the measurements.
Correlation analysis
In the exercise condition, ΔRT was not correlated with Δnumber of error trials in the Go/No-Go task (r = −0.03, P = 0.90), showing that there was no speed-accuracy tradeoff.
Table 2 summarizes the results of correlation analysis between cognitive performance and physiological parameters. In the exercise group, we observed that ΔRT was negatively correlated with Δcerebral oxygenation (r = −0.64, P = 0.004, Fig. 4). Alterations in other physiological parameters were not correlated with cognitive performance in the exercise and control groups (all Ps > 0.05).

Relationship between Δcerebral oxygenation and ΔRT (a) and between Δadrenaline and ΔRT (b)
In the exercise group, Δskin blood flow was not correlated with Δoxy-Hb (r = 0.43, P = 0.08), Δdeoxy-Hb (r = 0.19, P = 0.44), Δtotal-Hb (r = 0.38, P = 0.12), and Δcerebral oxygenation (r = 0.20, P = 0.44). In the Control group, Δskin blood flow was not correlated with Δoxy-Hb (r = 0.09, P = 0.76), Δdeoxy-Hb (r = −0.01, P = 0.99), Δtotal-Hb (r = 0.05, P = 0.86), and Δcerebral oxygenation (r = −0.01, P = 0.97). These results indicate that alterations in skin blood flow were not associated with alterations in oxy-Hb, deoxy-Hb, total-Hb, and cerebral oxygenation.
Discussion
The major findings of this study were: (1) ΔRT was negatively correlated with Δcerebral oxygenation and (2) alterations in BDNF, IGF-1, and blood lactate concentrations were not correlated with cognitive function after exhaustive exercise. These results suggest that recovery of cerebral oxygenation affects speed of response in the cognitive task after exhaustive exercise. Venous blood samples were not directly associated with cognitive function after exhaustive exercise. The present results suggest that recovery of prefrontal oxygenation affects executive function after exhaustive exercise.
A previous study indicated that decreases in cerebral oxygenation were not related to cognitive impairments during strenuous exercise (Ando et al. 2011). Another study also reported that inhibitory control was maintained despite decrease in cerebral oxygenation during exercise near exhaustion (Schmit et al. 2015). In contrast, impaired cognitive performance during heavy exercise was associated with decrease in cerebral oxygenation (Mekari et al. 2015). The discrepancies are probably due to the differences in exercise intensity, duration, and physical fitness of participants. In the present study, we observed that ΔRT was negatively correlated with Δcerebral oxygenation after exhaustive exercise, which indicates that recovery of prefrontal oxygenation affected cognitive function after exhaustive exercise. Exercise may facilitate implicit information by enhanced noradrenergic and dopaminergic systems (Dietrich and Audiffren 2011). This implies that brain neurotransmitters could play a key role in alterations in speed of response during and after exercise. At the cellular level, the turnover of several neurotransmitters seems to be altered under hypoxia (Raichle and Hornbein 2001). This means that oxygen availability is critical for the turnover of neurotransmitters. In the case that oxygen availability was compromised in the brain areas under exhaustive condition, it can be speculated that reduced oxygen availability affected neurotransmitters turnover and impaired speed of response in the cognitive task. In contrast, sufficient recovery of oxygen availability would impair less speed of response even after exhaustive exercise. Therefore, it is plausible that degree of cerebral oxygenation recovery affected RT after exhaustive exercise. The present findings may suggest that the maintenance and recovery of cerebral oxygenation are a key determinant of cognitive performance in sports under exhaustive situations. However, it should be noted that substantial decrease in cerebral oxygenation did not impair cognitive function during moderate exercise under hypoxia (Ando et al. 2013; Komiyama et al. 2015). Given that cerebral blood flow does not match the metabolic demand during heavy exercise (Ogoh and Ainslie 2009), the present association between cognitive function and cerebral oxygenation may be limited to the exhaustive condition, where regional cerebral metabolism could be compromised.
Moderate exercise has been suggested to increase arousal level to an optimal level and improve cognitive function (Brisswalter et al. 2002; Chang et al. 2012; Lambourne and Tomporowski 2010). However, further increases in arousal level (i.e., over-arousal) may produce neural noise and impair cognitive performance (McMorris 2016a). Since the original hypothesis by Cooper (Cooper 1973), the association between arousal level and catecholamines has been implicated (Chmura et al. 1994; McMorris 2016a). Indeed, one would expect that increases in catecholamine concentrations lead to over-arousal and have negative effects on cognitive function following heavy exercise (McMorris 2016a). In the present study, however, we observed no relationships between alterations in cognitive function and circulating catecholamines. These results indicate that circulating catecholamines were not directly associated with cognitive function after exhaustive exercise. Hence, the present study may suggest that cognitive performance is not predictable from circulating blood catecholamines after exhaustive exercise.
It has been suggested that upregulation of BDNF expression is associated with neuroplasticity (Cotman and Berchtold 2002; Voss et al. 2013). In contrast, less is known how alterations in BDNF affect cognitive function after acute exercise. In the present study, there was no association between cognitive function and serum BDNF after exhaustive exercise, suggesting that alterations in peripheral BDNF are not related to cognitive function after exhaustive exercise. Given that peripheral BDNF is merely indicative of central concentration, the real effects of BDNF on cognitive function are probably downstream of synthesis and release (McMorris 2016a). Alternatively, a recent review summarized that peripheral BDNF is closely related to memory task and is not implicated more broadly in explaining the effects of acute exercise on other types of cognitive performance (Piepmeier and Etnier 2015). Thus, another possible explanation for the absence of the association between alterations in serum BDNF and cognitive function may be that executive function was assessed in the present study.
IGF-1 has multipotent neuroprotective effects and has been demonstrated as a potent mediator of the multi-beneficial effects of exercise on the brain (Nishijima et al. 2016). Previous studies using both human and rodent models have suggested that serum IGF-1 increases following acute resistance exercise or resistance exercise training (Borst et al. 2001; Cassilhas et al. 2007, 2012; Tsai et al. 2014). In the present study, serum IGF-1 significantly increased after exhaustive exercise. We used the maximal exercise test, which is thought to recruit motor units containing fast fibers to a greater extent. Thus, it is reasonable that serum IGF-1 concentration increased after the exercise until exhaustion. It has been suggested that increases in serum IGF-1 after resistance exercise may contribute to cognitive improvements (Cassilhas et al. 2012; Cotman and Berchtold 2002; Ding et al. 2006). However, in the present study, alterations in cognitive performance were not correlated with increases in serum IGF-1. Hence, this result suggests that alterations in serum IGF-1 are not directly associated with cognitive function after exhaustive exercise. Nonetheless, it is less clear whether alterations in IGF-1 are associated with cognitive function after acute exercise. Further studies are needed to examine whether increases in IGF-1 may be responsible for alterations in cognitive function after acute exercise.
A recent study suggested that blood lactate may play a key role in improvements in cognitive function after high-intensity exercise (Tsukamoto et al. 2016). In the present study, blood lactate concentration substantially increased after exhaustive exercise. However, alterations in cognitive performance were not correlated with increases in blood lactate concentration. This result suggests that increases in blood lactate are not directly associated with cognitive function after exhaustive exercise. Rather, lactate is well known to be taken up in the brain, which serves as an energy fuel (Quistorff et al. 2008; van Hall 2010). Hence, in the present study, it is likely that lactate served as an energy fuel in the brain areas after exhaustive exercise.
We have to acknowledge limitations in the present study. First, although we proposed several candidates that affect cognitive function, many physiological alterations occur simultaneously in response to acute exercise. Changes in cerebral circulation, blood catecholamines, and growth and neurotrophic factors were not isolated with other physiological changes induced by acute exercise. Hence, we cannot exclude confounding factors, and sophisticated protocols are still necessary to reveal contribution of each physiological change. In the present study, we focused on how alterations in physiological variables affect executive function. In that sense, the present perspective may be more homeostatic than allostatic. However, given that research investigating activity and relationship among the multiple regulatory loops would be helpful to understand physiological regulatory systems (Ramsay and Woods 2014), further study should focus on the integration and contribution of different systems (e.g., Ekkekakis et al. 2016).
Second, recent studies challenged the validity and/or reliability of the measurement using NIRS (Sorensen et al. 2012; Takahashi et al. 2011). In particular, concerns raised by recent criticisms are the contamination of skin blood flow. However, even if it might be difficult to exclude the effects of extracranial blood flow completely, we expected that the effects of near-surface blood flow on cerebral oxygenation were reduced by subtraction of data from different source-detector distances. The subtraction was performed based on the assumption that NIRS signals are primarily originated from skin blood flow when distance between the source and the detector was 20 mm. Takahashi et al. (2011) suggested that NIRS signals primarily reflect skin blood flow even when distance between optodes was 30 mm. Furthermore, we observed that oxy-Hb detected at channel 1 was significantly correlated with skin blood flow (r = 0.61, P = 0.007), suggesting that NIRS signals are affected by skin blood flow in the present study. Hence, we expected that subtraction reduced the effects of near-surface blood flow. Nevertheless, we have to admit that further evaluation using the state-of-the-art method (e.g., Yucel et al. 2015) is needed to understand how exhaustive exercise alters cerebral oxygenation.
Finally, the present study was not a randomized cross-over study and number of participants was not equal, which may limit the impact of the study. Given that psychological as well as physiological factors determine endurance performance (e.g., attentional strategies, Bertollo et al. 2015), further studies are required to examine the effects of exhaustive exercise on cognitive performance in a randomized cross-over design.
Conclusion
We examined executive function after exhaustive exercise and attempted to identify physiological factors that determine executive function. The present results indicate that recovery of prefrontal oxygenation affects cognitive function after exhaustive exercise. In many sports, players are required to make decisions quickly and accurately even after exhaustive intermittent exercise. The present findings suggest that quick recovery of cerebral oxygenation may play a key role in cognitive performance in such a situation. In the present study, we focused on how physiological factors affect executive function. However, the effects of exhaustive exercise are multifaceted. Multimodal and multidisciplinary perspective is necessary to understand the issue. In addition to measurements used in the present study, integration and contribution of different systems should be further investigated.
Abbreviations
- BDNF:
-
Brain-derived neurotrophic factor
- DBP:
-
Diastolic blood pressure
- Deoxy-Hb:
-
Deoxyhemoglobin
- DR:
-
Delayed-response
- IGF-1:
-
Insulin-like growth hormone factor 1
- NIRS:
-
Near-infrared spectroscopy
- NTS:
-
Nucleus tractus solitarii
- Oxy-Hb:
-
Oxyhemoglobin
- RPE:
-
Ratings of perceived exertion
- RT:
-
Reaction time
- SBP:
-
Systolic blood pressure
- SD:
-
Standard deviation
- Total-Hb:
-
Total hemoglobin
References
Ando S, Yamada Y, Kokubu M (2010) Reaction time to peripheral visual stimuli during exercise under hypoxia. J Appl Physiol 108(5):1210–1216. doi:10.1152/japplphysiol.01115.2009
Ando S, Kokubu M, Yamada Y, Kimura M (2011) Does cerebral oxygenation affect cognitive function during exercise? Eur J Appl Physiol 111(9):1973–1982. doi:10.1007/s00421-011-1827-1
Ando S, Hatamoto Y, Sudo M, Kiyonaga A, Tanaka H, Higaki Y (2013) The effects of exercise under hypoxia on cognitive function. PLoS One 8(5):e63630. doi:10.1371/journal.pone.0063630
Bertollo M, di Fronso S, Filho E, Lamberti V, Ripari P, Machado Reis V, Comani S, Bortoli L, Robazza C (2015) To focus or not to focus: is attention on the core components of action beneficial for cycling performance? Sport Psychol 29(2):110–119
Borg G (ed) (1975) Simple rating for estimation of perceived exertion. Physical work and effort. Pergamon, New York
Borst SE, De Hoyos DV, Garzarella L, Vincent K, Pollock BH, Lowenthal DT, Pollock ML (2001) Effects of resistance training on insulin-like growth factor-I and IGF binding proteins. Med Sci Sports Exerc 33(4):648–653
Boushel R, Langberg H, Olesen J, Gonzales-Alonzo J, Bulow J, Kjaer M (2001) Monitoring tissue oxygen availability with near infrared spectroscopy (NIRS) in health and disease. Scand J Med Sci Sports 11(4):213–222
Brisswalter J, Collardeau M, Rene A (2002) Effects of acute physical exercise characteristics on cognitive performance. Sports Med 32(9):555–566
Cassilhas RC, Viana VA, Grassmann V, Santos RT, Santos RF, Tufik S, Mello MT (2007) The impact of resistance exercise on the cognitive function of the elderly. Med Sci Sports Exerc 39(8):1401–1407. doi:10.1249/mss.0b013e318060111f
Cassilhas RC, Lee KS, Fernandes J, Oliveira MG, Tufik S, Meeusen R, de Mello MT (2012) Spatial memory is improved by aerobic and resistance exercise through divergent molecular mechanisms. Neuroscience 202:309–317. doi:10.1016/j.neuroscience.2011.11.029
Chang YK, Labban JD, Gapin JI, Etnier JL (2012) The effects of acute exercise on cognitive performance: a meta-analysis. Brain Res 1453:87–101. doi:10.1016/j.brainres.2012.02.068
Chmura J, Nazar K, Kaciuba-Uscilko H (1994) Choice reaction time during graded exercise in relation to blood lactate and plasma catecholamine thresholds. Int J Sports Med 15(4):172–176. doi:10.1055/s-2007-1021042
Cooper CJ (1973) Anatomical and physiological mechanisms of arousal, with special reference to the effects of exercise. Ergonomics 16(5):601–609. doi:10.1080/00140137308924551
Cornford EM, Braun LD, Oldendorf WH, Hill MA (1982) Comparison of lipid-mediated blood–brain-barrier penetrability in neonates and adults. Am J Physiol 243(3):C161–C168
Cotman CW, Berchtold NC (2002) Exercise: a behavioral intervention to enhance brain health and plasticity. Trends Neurosci 25(6):295–301
Dietrich A, Audiffren M (2011) The reticular-activating hypofrontality (RAH) model of acute exercise. Neurosci Biobehav Rev 35(6):1305–1325. doi:10.1016/j.neubiorev.2011.02.001
Ding Q, Vaynman S, Akhavan M, Ying Z, Gomez-Pinilla F (2006) Insulin-like growth factor I interfaces with brain-derived neurotrophic factor-mediated synaptic plasticity to modulate aspects of exercise-induced cognitive function. Neuroscience 140(3):823–833. doi:10.1016/j.neuroscience.2006.02.084
Ekkekakis P, Vazou S, Bixby WR, Georgiadis E (2016) The mysterious case of the public health guideline that is (almost) entirely ignored: call for a research agenda on the causes of the extreme avoidance of physical activity in obesity. Obes Rev 17(4):313–329. doi:10.1111/obr.12369
Glickman ME, Rao SR, Schultz MR (2014) False discovery rate control is a recommended alternative to Bonferroni-type adjustments in health studies. J Clin Epidemiol 67(8):850–857. doi:10.1016/j.jclinepi.2014.03.012
Gonzalez-Alonso J, Dalsgaard MK, Osada T, Volianitis S, Dawson EA, Yoshiga CC, Secher NH (2004) Brain and central haemodynamics and oxygenation during maximal exercise in humans. J Physiol 557(Pt 1):331–342. doi:10.1113/jphysiol.2004.060574
Harada T, Okagawa S, Kubota K (2004) Jogging improved performance of a behavioral branching task: implications for prefrontal activation. Neurosci Res 49(3):325–337. doi:10.1016/j.neures.2004.03.011
Ide K, Secher NH (2000) Cerebral blood flow and metabolism during exercise. Prog Neurobiol 61(4):397–414
Komiyama T, Sudo M, Higaki Y, Kiyonaga A, Tanaka H, Ando S (2015) Does moderate hypoxia alter working memory and executive function during prolonged exercise? Physiol Behav 139:290–296. doi:10.1016/j.physbeh.2014.11.057
Lambourne K, Tomporowski P (2010) The effect of exercise-induced arousal on cognitive task performance: a meta-regression analysis. Brain Res 1341:12–24. doi:10.1016/j.brainres.2010.03.091
Lee JK, Koh AC, Koh SX, Liu GJ, Nio AQ, Fan PW (2014) Neck cooling and cognitive performance following exercise-induced hyperthermia. Eur J Appl Physiol 114(2):375–384. doi:10.1007/s00421-013-2774-9
McGaugh JL, Cahill L, Roozendaal B (1996) Involvement of the amygdala in memory storage: interaction with other brain systems. Proc Natl Acad Sci USA 93(24):13508–13514
McMorris T (2016a) Beyond the catecholamine hypothesis for an acute exercise–cognition interaction: a neurochemical perspective. In: McMorris T (ed) Exercise–cognition interaction: neuroscience perspective. Elsevier, Amsterdam, pp 65–103
McMorris T (2016b) Developing the catecholamines hypothesis for the acute exercise-cognition interaction in humans: lessons from animal studies. Physiol Behav 165:291–299. doi:10.1016/j.physbeh.2016.08.011
Meeusen R, De Meirleir K (1995) Exercise and brain neurotransmission. Sports Med 20(3):160–188
Mekari S, Fraser S, Bosquet L, Bonnery C, Labelle V, Pouliot P, Lesage F, Bherer L (2015) The relationship between exercise intensity, cerebral oxygenation and cognitive performance in young adults. Eur J Appl Physiol 115(10):2189–2197. doi:10.1007/s00421-015-3199-4
Miyashita T, Williams CL (2006) Epinephrine administration increases neural impulses propagated along the vagus nerve: role of peripheral beta-adrenergic receptors. Neurobiol Learn Mem 85(2):116–124. doi:10.1016/j.nlm.2005.08.013
Nishijima T, Torres-Aleman I, Soya H (2016) Exercise and cerebrovascular plasticity. Prog Brain Res 225:243–268. doi:10.1016/bs.pbr.2016.03.010
Nybo L, Secher NH (2004) Cerebral perturbations provoked by prolonged exercise. Prog Neurobiol 72(4):223–261. doi:10.1016/j.pneurobio.2004.03.005
Ogoh S, Ainslie PN (2009) Cerebral blood flow during exercise: mechanisms of regulation. J Appl Physiol 107(5):1370–1380. doi:10.1152/japplphysiol.00573.2009
Piepmeier AT, Etnier JL (2015) Brain-derived neurotrophic factor (BDNF) as a potential mechanism of the effects of acute exercise on cognitive performance. J Sport Health Sci 4(1):14–23. doi:10.1016/j.jshs.2014.11.001
Quistorff B, Secher NH, Van Lieshout JJ (2008) Lactate fuels the human brain during exercise. FASEB J 22(10):3443–3449. doi:10.1096/fj.08-106104
Raichle M, Hornbein T (2001) The high-altitude brain. In: Hornbein T, Schoene R (eds) High altitude: an exploration of human adaptation. Marcel Dekker, New York, pp 377–423
Ramsay DS, Woods SC (2014) Clarifying the roles of homeostasis and allostasis in physiological regulation. Psychol Rev 121(2):225–247. doi:10.1037/a0035942
Rooks CR, Thom NJ, McCully KK, Dishman RK (2010) Effects of incremental exercise on cerebral oxygenation measured by near-infrared spectroscopy: a systematic review. Prog Neurobiol 92(2):134–150. doi:10.1016/j.pneurobio.2010.06.002
Schmit C, Davranche K, Easthope CS, Colson SS, Brisswalter J, Radel R (2015) Pushing to the limits: the dynamics of cognitive control during exhausting exercise. Neuropsychologia 68:71–81. doi:10.1016/j.neuropsychologia.2015.01.006
Sorensen H, Secher NH, Siebenmann C, Nielsen HB, Kohl-Bareis M, Lundby C, Rasmussen P (2012) Cutaneous vasoconstriction affects near-infrared spectroscopy determined cerebral oxygen saturation during administration of norepinephrine. Anesthesiology 117(2):263–270. doi:10.1097/ALN.0b013e3182605afe
Takahashi T, Takikawa Y, Kawagoe R, Shibuya S, Iwano T, Kitazawa S (2011) Influence of skin blood flow on near-infrared spectroscopy signals measured on the forehead during a verbal fluency task. Neuroimage 57(3):991–1002. doi:10.1016/j.neuroimage.2011.05.012
Tobias JD, Johnson GA, Rehman S, Fisher R, Caron N (2008) Cerebral oxygenation monitoring using near infrared spectroscopy during one-lung ventilation in adults. J Minim Access Surg 4(4):104–107
Tsai CL, Wang CH, Pan CY, Chen FC, Huang TH, Chou FY (2014) Executive function and endocrinological responses to acute resistance exercise. Front Behav Neurosci 8:262. doi:10.3389/fnbeh.2014.00262
Tsukamoto H, Suga T, Takenaka S, Tanaka D, Takeuchi T, Hamaoka T, Isaka T, Ogoh S, Hashimoto T (2016) Repeated high-intensity interval exercise shortens the positive effect on executive function during post-exercise recovery in healthy young males. Physiol Behav 160:26–34. doi:10.1016/j.physbeh.2016.03.029
van Hall G (2010) Lactate kinetics in human tissues at rest and during exercise. Acta Physiol (Oxf) 199(4):499–508. doi:10.1111/j.1748-1716.2010.02122.x
Voss MW, Vivar C, Kramer AF, van Praag H (2013) Bridging animal and human models of exercise-induced brain plasticity. Trends Cogn Sci 17(10):525–544. doi:10.1016/j.tics.2013.08.001
Winter B, Breitenstein C, Mooren FC, Voelker K, Fobker M, Lechtermann A, Krueger K, Fromme A, Korsukewitz C, Floel A, Knecht S (2007) High impact running improves learning. Neurobiol Learn Mem 87(4):597–609. doi:10.1016/j.nlm.2006.11.003
Yucel MA, Aasted CM, Petkov MP, Borsook D, Boas DA, Becerra L (2015) Specificity of hemodynamic brain responses to painful stimuli: a functional near-infrared spectroscopy study. Sci Rep 5:9469. doi:10.1038/srep09469
Acknowledgements
We are grateful to Dr. Kisou Kubota for providing software to evaluate cognitive function.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
This study was funded by the Japan Society for the Promotion of Science KAKENHI (Grant Number: 25702039).
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Additional information
Communicated by Westerterp/Westerblad.
Rights and permissions
About this article

Cite this article
Sudo, M., Komiyama, T., Aoyagi, R. et al. Executive function after exhaustive exercise. Eur J Appl Physiol 117, 2029–2038 (2017). https://doi.org/10.1007/s00421-017-3692-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-017-3692-z