
Abstract
A melatonin-mediated reduction in body temperature could be useful as a “pre-cooling” intervention for athletes, as long as the melatonin dose is optimised so that substantial soporific effects are not induced. However, the melatonin-temperature dose–response relationship is unclear in humans. Individual studies have involved small samples of different sexes and temperature measurement sites. Therefore, we meta-analysed the effects of exogenous melatonin on body core temperature to quantify the dose–response relationship and to explore the influence of moderating variables such as sex and measurement site. Following a literature search, we meta-analysed 30 data-sets involving 193 participants and 405 ingestions of melatonin. The outcome was the mean difference (95 % confidence limits) in core temperature between the melatonin and placebo-controlled conditions in each study, weighted by the reciprocal of each standard error of the difference. The mean (95 % confidence interval) pooled reduction in core temperature was found to be 0.21 °C (0.18–0.24 °C). The dose–response relationship was found to be logarithmic (P < 0.0001). Doses of 0–5 mg reduced temperature by ~0.00–0.22 °C. Any further reductions in temperature were negligible with doses >5 mg. The pooled mean reduction was 0.13 °C (0.05–0.20 °C) for oral temperature vs 0.26 °C (0.20–0.32 °C) for tympanic and 0.22 °C (0.19–0.25 °C) for rectal temperature. In conclusion, our meta-regression revealed a logarithmic dose–response relationship between melatonin and its temperature lowering effects. A 5-mg dose of melatonin lowered core temperature by ~0.2 °C. Higher doses do not substantially increase this hypothermic effect and may induce greater soporific effects.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
The pineal secretory product, melatonin, plays an important role in the human circadian system and has soporific and hypothermic actions (Hughes and Badia 1997). Body temperature is known to vary with time of day due to the circadian rhythms of heat production and dissipation (Krauchi and Wirz-Justice 1994). Core temperature declines during the night (Krauchi 2007) and in nychthemeral conditions, the nocturnal peak in melatonin levels corresponds to the nadir in core temperature (Luboshizsky and Lavie 1998).
It is well-documented that exogenous melatonin has hypothermic properties (Arendt and Skene 2005; Cagnacci et al. 1994; Cagnacci et al. 1995; Cagnacci 1996; Gilbert et al. 1999), but the mechanisms for this phenomenon have yet to be fully elucidated. The ingestion of melatonin is believed to facilitate peripheral vasodilation (Aoki et al. 2008; Cagnacci et al. 1997; Krauchi et al. 1997). Van der Helm-Van Mil et al. (2003) reported that melatonin increased peripheral vasodilation without altering cerebral blood flow or heart rate, implicating that melatonin acts via receptors in the peripheral vasculature. Similarly, Cook et al. (2011) reported that melatonin decreased renal blood flow and increased forearm blood flow, with no change in cerebral blood flow. These effects on vascular blood flow suggest that the hypothermic effects of melatonin are mediated mainly by enhanced heat loss mechanisms.
The exact dose–response relationship between exogenous melatonin and core temperature is not yet well described. The reductions in core temperature reported in the literature appear to be variable, ranging from 0.1 to 0.4 °C (Atkinson et al. 2003; Macchi and Bruce 2004). The relatively small sample sizes of the studies render the statistical precision (i.e. confidence intervals, CI) of individual change in core temperature rather poor. Moreover, studies are heterogeneous in terms of many important factors that may influence core temperature responses, including study population and core temperature site.
The hypothermic properties of melatonin could be beneficial in certain circumstances. For example, a high ambient temperature increases thermal strain during exercise and occupational work. Core temperature may thus be a limiting factor during such activities (Gonzalez-Alonso et al. 1999). Therefore, a number of so-called “pre-cooling” methods have been developed to reduce core temperature and thereby enhance exercise performance in hot conditions (Booth et al. 1997; Marino 2002). The pre-cooling method of taking a cold shower may not always be practical and the effects of such a strategy may only last for 20–25 min (Lee and Haymes 1995). Melatonin has also been considered in this context of pre-cooling (Atkinson et al. 2003). Nevertheless, it is important to identify the lowest dose of melatonin which mediates a practically significant reduction in temperature, so that any soporific effects associated with higher doses of melatonin are minimised.
A meta-analysis can help improve the precision of effect size estimation and be useful for exploring the influence of various moderating factors on that effect size. Although meta-analyses have been undertaken on the effects of melatonin on sleep quality (Brzezinski et al. 2005), a meta-analysis has not been applied to the context of exogenous melatonin and thermoregulation. Therefore, the purpose of the present study was to meta-analyse the hypothermic properties of exogenous melatonin and quantify the dose–response relationship.
Methods
Search strategy and criteria
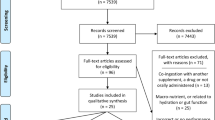
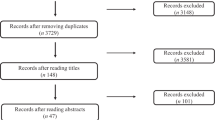
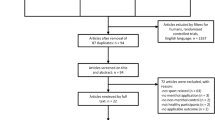
We completed an extensive literature search and review for all peer-reviewed studies that examined acute effects of melatonin administration on human body core temperature in humans. The search databases were Academic Search Complete, Medline and PubMed. The keywords and phrases employed in the search included “melatonin”, “Pineal”, “hypothermic effect of melatonin”, “melatonin and temperature”, and “human thermoregulation and melatonin levels”. Reference lists from published papers were also scrutinised for other relevant studies not cited in the online databases. For inclusion into the present meta-analysis, studies had to comprise placebo-controlled crossover-type trials, involve administration of an acute dose of exogenous melatonin, provide information regarding melatonin dose, have no other simultaneous pharmacological intervention or infusion technique and include the measurement of core temperature.
Review process
The initial search process resulted in the identification of 168 studies, of which 94 comprised human data that could potentially be included in the analyses. Of these studies, 76 did not conform to the inclusion criteria or provide relevant data and were subsequently removed. Inadequate reporting of results in some of the papers presented difficulties. These studies were excluded as they did not provide either the pre- and post-mean or standard deviation data necessary for the analysis. Eighteen studies remained relevant for meta-analysis. Two further studies (McLellan et al. 1999, 2000) were removed due to the uncompensable nature of heat loss in the experimental protocols, resulting in a total of 16 studies. Although the studies (McLellan et al. 1999, 2000) originally met the inclusion criteria, the fact that participants wore nuclear, biological, and chemical protective clothing had a subsequent effect on heat loss and thus they were not deemed suitable for inclusion within the analysis. Six of the sixteen studies provided multiple data-sets because different doses or conditions were included in these individual studies. This resulted in a total of 30 data-sets for analysis, comprising a total of 405 melatonin ingestions by a total of 193 participants.
Statistical analyses
Statistical analyses were conducted using Comprehensive Meta-Analysis (V2) and Stata (Statcorp, Texas) software. A random-effects meta-analysis of the mean difference in core temperature (melatonin compared to placebo) was conducted (Thompson and Higgins 2002). All of the studies included in the analyses comprised a single-group repeated measures design with control and experimental condition, therefore the standard error calculated from the standard error of the differences was meta-analysed. The fully adjusted estimates from individual studies were calculated using the inverse variance method (Higgins and Green 2008). Relative weights were assigned to the mean change within each study on the basis of sample size and between-subjects standard error. Publication bias was assessed using Eggers regression intercept. This determines whether the study estimate is related to the size of the study. Heterogeneity was assessed using the I 2 statistic and the Q test (Deeks et al. 2003). This examination was followed-up by subgroup analyses based on sex, time of day of ingestion and temperature measurement site.
The various moderators were also entered into a multivariate meta-regression model, which was undertaken using Stata (Harbord and Higgins 2008). Studies were coded for sex with ‘1’ referring to studies containing only men, ‘2’ referring to studies containing only women and ‘3’ equating to mixed sex studies involving both men and women. Melatonin dose was retained as a continuous variable and analysed in raw units as well as after natural logarithmic transformation. Time of day was categorised as morning (before 12:00 h) and afternoon (12:00 h and later). Temperature measurement sites comprised tympanic, rectal, oesophageal, intravaginal, and oral. Differences between levels of moderators were examined using the 95 % CI of each summary mean difference, with α set at 0.05.
Results
A summary of studies on the acute hypothermic effect of exogenous melatonin is shown in Table 1. The overall weighted mean reduction in body core temperature was 0.21 °C (0.18–0.24 °C) (P < 0.0005) as presented in the forest plot (Fig. 1). Publication bias was assessed using Eggers regression intercept and no statistically significant publication bias was evident (P = 0.39). Nevertheless, the study associated with the largest standard error (Atkinson et al. 2005b) was found to also report the greatest reduction in temperature. This study was removed in a sensitivity analysis, but the pooled mean reduction remained as 0.21 °C (0.18–0.24 °C), and there was again little evidence of publication bias (P = 0.46).

Forest plot showing the individual mean (95 % CI) change in core temperature following an acute dose of melatonin in each data-set. The final row of this figure shows the pooled mean reduction in core temperature
A statistically significant relationship was found between dose of melatonin and the magnitude of temperature reduction (P = 0.016, adjusted r 2 = 20 %). However, there was evidence of a logarithmic dose–response relationship, whereby relatively high doses did not seem to mediate substantially larger hypothermic effects than relatively low doses. Therefore, the dose variable was logarithmically transformed (natural logarithm) and re-analysed. A statistically significant logarithmic relationship between melatonin and temperature reduction was observed (P < 0.0001) and the adjusted r 2 increased to 39 % (Fig. 2). Doses of 0–5 mg reduced temperature by ~0.00–0.22 °C. Any further reductions in temperature were negligible with doses >5 mg.

Meta-regression of melatonin dose (logarithmically transformed) and the mean reduction in core temperature in each data-set. The size of each x–y symbol is proportional to the precision of each estimate of reduction in temperature
The results of the multivariate meta-regression (overall adjusted r 2 = 71 %) indicated that the reduction in body temperature was not substantially influenced by sex, although the effect approached statistical significance (P = 0.089). The weighted mean reductions in body core temperature were 0.21 °C (0.16–0.25 °C) for data-sets comprising only men (n = 16), 0.23 °C (0.07–0.38 °C) for studies comprising only women (n = 2) and 0.22 °C (0.18–0.26 °C) for mixed sex studies (n = 12). Fifty percent of the male only data-sets comprised high doses (≥5 mg) whilst all the female only data-sets utilised low doses (<5 mg). The mixed sex data-sets comprised 75 % low doses and 25 % high doses.
The multivariate meta-regression indicated that the reduction in body temperature was effected by temperature measurement site (P = 0.005). A decrease in core temperature of 0.3 °C (0.22–0.38 °C) was identified in the data-set involving intravaginal measurements (n = 1; low dose) compared with 0.16 °C (0.10–0.25 °C) for oesophageal (n = 1; low dose), 0.13 °C (0.05–0.20 °C) for oral measurements (n = 4; 75 % low dose, 25 % high dose); 0.26 °C (0.20–0.32 °C) for tympanic measurements (n = 5; 40 % low dose, 60 % high dose), and 0.22 °C (0.19–0.25 °C) for rectal measurements (n = 19; 63 % low dose, 37 % low dose).
The mean weighted reduction in body core temperature was 0.19 °C (0.15–0.24 °C) for data-sets in which melatonin was administered before 12:00 h (n = 17; 35 % high) and 0.23 °C (0.19–0.27 °C) for studies carried out after 12:00 h (n = 13). This difference was, however, not statistically significant (P = 0.26).
Discussion
We have completed the first meta-analysis of the hypothermic properties of melatonin to provide a more precise estimate of induced temperature change, the dose–response relationship, as well as an exploration of any between-study moderators of this change. Meta-analyses serve a useful purpose of quantifying the overall effect size from a number of different studies that may have small sample sizes. However, it is recognised that the analysis is dependent on the quality of the published data in peer-reviewed journals. It has been reported that there may be tendency for “negative” outcome studies to remain unpublished and thus influence the efficacy of the meta-analysis. Nevertheless, no statistically significant publication bias was evident within the current study; however, we cannot rule out that publication bias for “positive” findings only could have occurred in the present context, nor indeed most other fields of research.
We found that the pooled estimate of the reduction in body core temperature following melatonin administration was 0.21 °C (0.18–0.24 °C). The present meta-analysis, which weighted larger and more precise studies higher in the estimation of the pooled effect, has thus clarified that melatonin ingestion mediates a reduction of core temperature which is large enough to be useful in a number of ‘real world’ and clinical contexts. For example, various pre-cooling methods have been devised to reduce body core temperature prior to an endurance-based sporting event (Booth et al. 1997; Marino 2002). Arngrimsson et al. (2004) reported a similar drop of 0.2 °C in rectal temperature following the use of a cooling vest. This reduction resulted in a mean reduction in 5-km run time of 1.1 %.
The rationale behind a pre-cooling strategy is to reduce body temperature, before exercise, thereby increasing the margin for metabolic heat production and increasing the time to reach exhaustion due to elevated core temperature (Marino 2002). It has been reported that rectal temperature can be reduced by 0.2–0.3 °C following 30 min of pre-cooling induced by interventions like cold showers or baths (Hasegawa et al. 2006). Nevertheless, such interventions can be difficult for some people to tolerate. Therefore, the ingestion of melatonin may be a more tolerable pre-cooling approach for exercise in the heat.
Aoki et al. (2006) reported that daytime ingestion of melatonin stimulates the cutaneous active vasodilator system’s response to body heating by altering the threshold for activation to a lower core temperature. Atkinson et al. (2005a) reported that a 2.5-mg dose of melatonin prior to a bout of intermittent exercise in a moderately hot environment attenuated the rise in core temperature and magnified the increase in skin blood flow without any influences on subjective alertness and sleepiness. However, performance was not measured in this study. Consequently, further studies are required to determine whether the hypothermic effect of melatonin established in the current meta-analysis actually has an impact on exercise performance in compensable conditions. Furthermore, it may be that a small dose of melatonin, that in principle would reduce the potential soporific effects of melatonin compared with higher doses, may be used in combination with other established pre-cooling strategies, e.g. cold water immersion, ice jacket, cold fluid ingestion, to determine whether there is potential additive effect of multiple interventions.
The time-course of the effect of melatonin on core temperature also warrants further investigation. The timing of the peak suppression of core temperature varied between 60 and 229 min in the studies, but there was insufficient data to explore time-course as a moderator. Cagnacci et al. (1992) reported that a daytime administration of melatonin was accompanied by a rapid rise (within 20 min) in endogenous melatonin and a parallel decrease in core temperature. Van den Heuvel et al. (1999) reported that melatonin has a suppressive effect on daytime core temperature for at least 1–2 h after plasma melatonin levels return to normal daytime values. However, these researchers noted that an injection of melatonin at very-low doses suppresses the normal daytime increase in core temperature for only ~30–90 min. Satoh and Mishima (2001) reported that the hypothermic action of exogenous melatonin lasts approximately 3 h. The magnitude of suppression was positively correlated with endogenous levels of melatonin. Similarly, Dawson et al. (1996) demonstrated that melatonin can display hypothermic effects for at least 4 h post administration in a dose-dependent manner.
Our meta-regression revealed a logarithmic dose–response relationship between melatonin and its temperature lowering effects. A 5-mg dose of melatonin lowered core temperature by ~0.2 °C. Higher doses did not substantially increase this hypothermic effect and may induce detrimental soporific effects. The logarithmic dose–response relationship supports the notion that a dose–response relationship between melatonin and core temperature may exist, and a threshold prevails whereby raising melatonin levels to a detectable physiological level can result in a hypothermic effect (Cagnacci et al. 1994). Studies have reported considerable variability in plasma melatonin profiles following administration, particularly in the lower doses. Previous research (Burgess and Fogg 2008) has reported a large individual variability in endogenous salivary melatonin profiles with peak values ranging from 2 to 84 pg/ml. These combined findings provide further weight to the argument that a physiological threshold in endogenous melatonin may be linked to the maximum hypothermic effect.
Time of day of melatonin ingestion was not found to moderate the temperature reduction. It is well established that time of day has an impact on endogenous melatonin (Arendt 1998, 2005; Dawson and van den Heuvel 1998; Lewy 1999). Typically, melatonin levels begin to increase before sleep, peak in the early hours of the morning and decrease to daytime levels after waking (Burgess and Fogg 2008). This relationship is inverse to that of core temperature (Arendt and Skene 2005). Diurnal-living humans are in a state of heat gain in the morning and heat loss in the evening (Morris et al. 2009). The endogenous origin of the circadian variation in body temperature is the suprachiasmatic nuclei, which also influences the diurnal variation in melatonin secretion from the pineal gland (Hofman and Swaab 1993). It has been proposed that a role of melatonin is to regulate the diurnal variation in core temperature and that hypothermic effects of melatonin may explain at least half of the diurnal variation in core temperature observed in constant routine conditions (Cagnacci et al. 1992; Dawson et al. 1996).
Melatonin mediated a hypothermic effect at all temperature measurement sites studied, but the magnitude of effect differed between sites. It is recognised that measurement of “core” temperature does not necessarily refer to one specific anatomical location (Byrne and Lim 2007). Oesophageal temperature is deemed a gold standard site, since it provides the closest agreement with central blood temperature, and is sensitive to rapid changes in temperature (Moran and Mendal 2002). Yet, within the current meta-analysis only one study, involved oesophageal temperature measurement, probably because of the invasive nature of this method (Morris et al. 2009). There was little difference in hypothermic response between tympanic and rectal temperature sites, but the hypothermic effect was smaller for oral temperature, probably due to the variability and proneness to masking influences with this site (Lim et al. 2008). For example, it may take at least 5 min to gain a stable reading for this measurement site, which is even influenced by breathing rate (Lim et al. 2008).
Conclusions
We have undertaken the first meta-analysis of studies on the hypothermic effects of melatonin ingestion in humans. The overall weighted mean reduction (95 % CI) in body core temperature following melatonin ingestion was found to be 0.21 °C (0.18–0.24 °C). We found that a logarithmic rather than a linear relationship best described the dose-responses of melatonin on temperature lowering. A 5-mg dose of melatonin lowered core temperature by ~0.2 °C. Higher doses do not substantially increase this hypothermic effect and could induce soporific and anti-ergogenic effects.
References
Aizawa S, Tokura H, Morita T (2002) The administration of exogenous melatonin during the daytime lowers the thermoregulatory setpoint. J Therm Biol 27:115–199
Aoki K, Stephens DP, Zhao K, Kosiba WA, Johnson JM (2006) Modification of cutaneous vasodilator response to heat stress by daytime exogenous melatonin administration. Am J Physiol Regul Integr Comp Physiol 291:R619–R624
Aoki K, Zhao K, Yamazaki F, Sone R, Alvarez GA, Kosiba WA, Johnson JA (2008) Exogenous melatonin administration modifies cutaneous vasoconstrictor response to whole body skin cooling in humans. J Pineal Res 44:141–148
Arendt J (1998) Complex effects of melatonin. Therapie 53:479–488
Arendt J (2005) Melatonin: characteristics, concerns, and prospects. J Biol Rhythm 20:291–303
Arendt J, Skene DJ (2005) Melatonin as a chronobiotic. Sleep Med Rev 9:25–39
Arngrimsson SA, Petitt DS, Stueck MG, Jorgensen DK, Cureton KJ (2004) Cooling vest worn during active warm-up improves 5-km run performance in the heat. J Appl Physiol 96:1867–1874
Atkinson G, Drust B, Reilly T, Waterhouse J (2003) The relevance of melatonin to sports medicine and science. Sports Med 33:809–831
Atkinson G, Holder A, Robertson C, Gant N, Drust B, Reilly T, Waterhouse J (2005a) Effects of melatonin on the thermoregulatory responses to intermittent exercise. J Pineal Res 39:353–359
Atkinson G, Jones H, Edwards BJ, Waterhouse JM (2005b) Effects of daytime ingestion of melatonin on short-term athletic performance. Ergonomics 48:1512–1522
Booth J, Marino F, Ward JJ (1997) Improved running performance in hot humid conditions following whole body precooling. Med Sci Sports Exerc 29:943–949
Brzezinski A, Vangel MG, Wurtman RJ, Norrie G, Zhdanova I, Ben-Shushan A, Ford I (2005) Effects of exogenous melatonin on sleep: a meta-analysis. Sleep Med Rev 9:41–50
Burgess HJ, Fogg LF (2008) Individual differences in the amount and timing of salivary melatonin secretion. PLoS One 3:e3055
Burgess HJ, Sletten T, Savic N, Gilbert SS, Dawson D (2001) Effects of bright light and melatonin on sleep propensity, temperature, and cardiac activity at night. J Appl Physiol 91:1214–1222
Byrne C, Lim CL (2007) The ingestible telemetric body core temperature sensor: a review of validity and exercise applications. Br J Sports Med 41:126–133
Cagnacci A (1996) Melatonin in relation to physiology in adult humans. J Pineal Res 21:200–213
Cagnacci A, Elliott JA, Yen SS (1992) Melatonin: a major regulator of the circadian rhythm of core temperature in humans. J Clin Endocrinol Metab 75:447–452
Cagnacci A, Soldani R, Romagnolo C, Yen SS (1994) Melatonin-induced decrease of body temperature in women: a threshold event. Neuroendocrinology 60:549–552
Cagnacci A, Soldani R, Yen SS (1995) Hypothermic effect of melatonin and nocturnal core body temperature decline are reduced in aged women. J Appl Physiol 78:314–317
Cagnacci A, Krauchi K, Wirz-Justice A, Volpe A (1997) Homeostatic versus circadian effects of melatonin on core body temperature in humans. J Biol Rhythm 12:509–517
Cook JS, Charity LS, Ray CA (2011) Melatonin differentially affects vascular blood flow in humans. Am J Physiol Heart Circ Physiol 300:H670–H674
Dawson D, van den Heuvel CJ (1998) Integrating the actions of melatonin on human physiology. Ann Med 30:95–102
Dawson D, Gibbon S, Singh P (1996) The hypothermic effect of melatonin on core body temperature: is more better? J Pineal Res 20:192–197
Deacon S, Arendt J (1995) Melatonin-induced temperature suppression and its acute phase-shifting effects correlate in a dose-dependent manner in humans. Brain Res 688:77–85
Deacon S, English J, Arendt J (1994) Acute phase-shifting effects of melatonin associated with suppression of core body temperature in humans. Neurosci Lett 178:32–34
Deeks JJ, Altman DG, Bradburn MJ (2003) Statistical methods for examining heterogeneity and combining results from several studies in meta-analysis. In: Egger M, Davey Smith G, Altman DG (eds) Systematic reviews in health care: meta analysis in context. BMJ Publishing Group, London
Dollins AB, Zhdanova IV, Wurtman RJ, Lynch HJ, Deng MH (1994) Effect of inducing nocturnal serum melatonin concentrations in daytime on sleep, mood, body temperature, and performance. Proc Natl Acad Sci USA 91:1824–1828
Gilbert SS, van den Heuvel CJ, Kennaway DJ, Dawson D (1999) Peripheral heat loss: a predictor of the hypothermic response to melatonin administration in young and older women. Physiol Behav 66:365–370
Gonzalez-Alonso J, Teller C, Andersen SL, Jensen FB, Hyldig T, Nielsen B (1999) Influence of body temperature on the development of fatigue during prolonged exercise in the heat. J Appl Physiol 86:1032–1039
Harbord RM, Higgins JPT (2008) Meta-regression in Stata. Stata J 8:493–519
Hasegawa H, Takatori T, Komura T, Yamasaki M (2006) Combined effects of pre-cooling and water ingestion on thermoregulation and physical capacity during exercise in a hot environment. J Sports Sci 24:3–9
Higgins JPT, Green S (2008) Cochrane handbook for systematic reviews. Wiley-Blackwell, Chichester
Hofman MA, Swaab DF (1993) Diurnal and seasonal rhythms of neuronal activity in the suprachiasmatic nucleus of humans. J Biol Rhythm 8:283–295
Hughes RJ, Badia P (1997) Sleep-promoting and hypothermic effects of daytime melatonin administration in humans. Sleep 20:124–131
Krauchi K (2007) The human sleep-wake cycle reconsidered from a thermoregulatory point of view. Physiol Behav 90:236–245
Krauchi K, Wirz-Justice A (1994) Circadian rhythm of heat production, heart rate, and skin and core temperature under unmasking conditions in men. Am J Physiol 267:R819–R829
Krauchi K, Cajochen C, Wirz-Justice A (1997) A relationship between heat loss and sleepiness: effects of postural change and melatonin administration. J Appl Physiol 83:134–139
Lee DT, Haymes EM (1995) Exercise duration and thermoregulatory responses after whole body precooling. J Appl Physiol 79:1971–1976
Lewy AJ (1999) Melatonin as a marker and phase-resetter of circadian rhythms in humans. Adv Exp Med Biol 460:425–434
Lim CL, Byrne C, Lee JK (2008) Human thermoregulation and measurement of body temperature in exercise and clinical settings. Ann Acad Med Singap 37:347–353
Luboshizsky R, Lavie P (1998) Sleep-inducing effects of exogenous melatonin administration. Sleep Med Rev 2:191–202
Macchi MM, Bruce JN (2004) Human pineal physiology and functional significance of melatonin. Front Neuroendocrinol 25:177–195
Marino FE (2002) Methods, advantages, and limitations of body cooling for exercise performance. Br J Sports Med 36:89–94
McLellan TM, Gannon GA, Zamecnik J, Gil V, Brown GM (1999) Low doses of melatonin and diurnal effects on thermoregulation and tolerance to uncompensable heat stress. J Appl Physiol 87:308–316
McLellan TM, Smith IF, Gannon GA, Zamecnik J (2000) Melatonin has no effect on tolerance to uncompensable heat stress in man. Eur J Appl Physiol 83:336–343
Moran DS, Mendal L (2002) Core temperature measurement: methods and current insights. Sports Med 32:879–885
Morris C, Atkinson G, Drust B, Marrin K, Gregson W (2009) Human core temperature responses during exercise and subsequent recovery: an important interaction between diurnal variation and measurement site. Chronobiol Int 26:560–575
Reid K, Van den Heuvel C, Dawson D (1996) Day-time melatonin administration: effects on core temperature and sleep onset latency. J Sleep Res 5:150–154
Satoh K, Mishima K (2001) Hypothermic action of exogenously administered melatonin is dose-dependent in humans. Clin Neuropharmacol 24:334–340
Thompson SG, Higgins JPT (2002) How should meta-regression analyses be undertaken and interpreted? Stat Med 21:1559–1573
Van den Heuvel CJ, Kennaway DJ, Dawson D (1999) Thermoregulatory and soporific effects of very low dose melatonin. Am J Physiol 276:E249–E254
van der Helm-Van Mil AHM, van Someren EJW, van den Boom R, van Buchem MA, de Craen AJM, Blauw GJ (2003) No Influence of melatonin on cerebral blood flow in humans. J Clin Endocrinol Metab 88:5989–5994
Author information
Authors and Affiliations
Corresponding author
Additional information
Communicated by George Havenith.
Rights and permissions
About this article
Cite this article
Marrin, K., Drust, B., Gregson, W. et al. A meta-analytic approach to quantify the dose–response relationship between melatonin and core temperature. Eur J Appl Physiol 113, 2323–2329 (2013). https://doi.org/10.1007/s00421-013-2668-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-013-2668-x