
Abstract
Pain elicits complex adaptations of motor strategy, leading to impairments in the generation and control of steady forces, which depend on muscle architecture. The present study used a cross-over design to assess the effects of muscle pain on the stability of multidirectional (task-related and tangential) forces during sustained dorsiflexions, elbow flexions, knee extensions, and plantarflexions. Fifteen healthy subjects performed series of isometric contractions (13-s duration, 2.5, 20, 50, 70% of maximal voluntary force) before, during, and after experimental muscle pain. Three-dimensional force magnitude, angle and variability were measured while the task-related force was provided as feedback to the subjects. Surface electromyography was recorded from agonist and antagonist muscles. Pain was induced in agonist muscles by intramuscular injections of hypertonic (6%) saline with isotonic (0.9%) saline injections as control. The pain intensity was assessed on an electronic visual analogue scale. Experimental muscle pain elicited larger ranges of force angle during knee extensions and plantarflexions (P < 0.03) and higher normalized fluctuations of task-related (P < 0.02) and tangential forces (P < 0.03) compared with control assessments across force levels, while the mean force magnitudes, mean force angle and the level of muscle activity were non-significantly affected by pain. Increased multidirectional force fluctuations probably resulted from multiple mechanisms that, acting together, balanced the mean surface electromyography. Although pain adaptations are believed to aim at the protection of the painful site, the current results show that they result in impairments in steadiness of force.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Force variability is an inherent characteristic of human motor control (Stein et al. 2005) which is mainly influenced by the excitation and discharge behaviour of the motoneuron pool (Tracy et al. 2007). Increased force variability has been associated with muscle fatigue (Missenard et al. 2009), ageing (Tracy 2007), increased risk of falls (Carville et al. 2007), and in particular, higher force fluctuations were observed in patients with chronic musculoskeletal pain disorders such as knee osteoarthritis and subacromial impingement syndrome compared with healthy controls (Hortobágyi et al. 2004; Bandholm et al. 2006). Although it has been shown that pain may cause changes in muscle coordination (Graven-Nielsen et al. 1997), it is still unclear how these changes affect the three-directional distribution of force variability.
It has been suggested that, during painful contractions, the central nervous system is able to maintain a constant submaximal force level by reducing motor unit firing rates (Farina et al. 2004), in addition to a spatial redistribution of activity within and between muscles (Madeleine et al. 2006; Falla et al. 2007; Tucker and Hodges 2010). Because different muscle compartments have distinct directional alignments of force production (Herrmann and Flanders 1998), the redistribution of muscle activity is likely to elicit directional changes in the resultant force vector (Kutch et al. 2008; Tucker and Hodges 2010).
Using experimental pain models consisting of intramuscular injections of algesic substances, it is possible to temporarily induce pain in healthy individuals while avoiding other confounder factors associated with chronic pathologies. However, very few studies have employed such models to investigate force variability, showing that even acute pain elicits significant impairments in the control of static forces of finger, arm, and shoulder muscles (Del Santo et al. 2007; Bandholm et al. 2008). While previous investigations were limited to unidirectional force assessments during contractions of the upper limbs at moderate force levels (20–35% of maximal voluntary force, MVC), force fluctuations are known to depend on muscle architecture and on the level of exerted force (Tracy et al. 2007), and studies using exercise-induced delayed onset muscle soreness as pain model for the elbow flexors reported greater impairments during force levels under 10% MVC (Semmler et al. 2007). The assessment of thee-dimensional force fluctuations has been so far limited to baseline and fatiguing contractions, showing similar modulation of task-related and tangential force components (Hong et al. 2007; Svendsen and Madeleine 2010; Salomoni and Graven-Nielsen 2012), but it is unclear if the three components of force fluctuations are similarly affected by pain. This investigation may provide new insight on how pain-related changes in muscle activity affect the stability of three-dimensional forces during daily life activities.
The current study assessed the effects of experimental muscle pain on the distribution and steadiness of multidirectional (task-related and tangential) forces during submaximal isometric contractions at low, moderate, and high force levels. Based on the evidence from previous studies, the hypotheses investigated were (1) experimental muscle pain will alter the angle of the resultant force compared with non-painful contractions, (2) similar increases in task-related and tangential force variability will be observed during pain compared with baseline assessments, and (3) the effects of experimental muscle pain will be larger during low compared with high force levels.
Methods
Subjects
Fifteen subjects (12 males, age 28.3 ± 6.5 years; height 175 ± 10 cm; weight 72.8 ± 12.7 kg; mean ± SD) with no known musculoskeletal disorder participated in this study after receiving detailed written and verbal explanation and signing an informed consent. The study was conducted in accordance with the Declaration of Helsinki and approved by the Local Ethics Committee (N-20090036).
Protocol
This study used a randomized, blinded, placebo controlled, crossover-design including two sessions with at least 1 week interval in between. During each session, subjects performed isometric contractions of two distinct muscle groups, randomly assigned between dorsiflexors, elbow flexors, knee extensors and plantarflexors. All contractions were performed in the dominant side. One subject was excluded from performing knee extensions due to signs of muscle soreness not related to the protocol.
For each muscle group, agonist maximal voluntary contraction (MVC) force was assessed during three consecutive isometric trials (5 s), followed by three antagonist MVC trials, with at least 30 s of rest after each trial. This was followed by six series of force-matched tasks, each comprised of isometric contractions (13 s) performed at 2.5, 20, 50, and 70% of MVC force, in random order, each followed by at least 15 s of rest. Additional time was provided if subjects felt tired, particularly after high force levels. This rest period avoided the effects of fatigue, while ensuring that all contractions following the painful injection were performed within the period of high pain sensation, which usually lasts only for a few minutes (Graven-Nielsen 2006). Subjects received two intramuscular injections of saline, and for each injection the series of isometric contractions were performed under three conditions, with at least 1 min interval: before, immediately after the injection, and after the cessation of any painful effects due to the injection, hereafter designated as pre, during, and post conditions respectively.
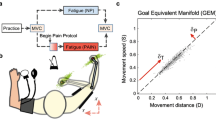
Subjects were given practice trials for familiarization with the experimental protocol. During all contractions, three-dimensional forces were recorded (Fig. 1) while a computer screen provided a ramp-and-hold target force feedback corresponding to 2 s of ramp phase and 11 s of hold phase. The visual scales of the feedback remained constant across all target forces and muscle groups. After three preparatory beeps, the current task-related force was shown in a time line on the screen, and subjects were required to match the ramp-and-hold feedback.

Force magnitude and angle (left side) were assessed using a high-resolution six-axis sensor while subjects used custom-built setups to perform isometric dorsiflexions (a), elbow flexions (b), knee extensions (c), and plantarflexions (d)
Experimental muscle pain
Muscle pain was induced by intramuscular injections of sterile hypertonic saline (1.0 ml, 6%) into one agonist muscle of each muscle group: m. tibialis anterior for dorsiflexors, m. brachioradialis for elbow flexors, m. vastus medialis for knee extensors, and m. gastrocnemius medialis for plantarflexors. Injections of isotonic saline (1.0 ml, 0.9%) were used as control. Injections were performed using a 2 ml plastic syringe with a disposable needle (27G, 13 mm), and the order of the injections was randomized and balanced between subjects and between muscle groups.
The experimental pain intensity was assessed on a 10-cm electronic visual analogue scale (VAS), where 0 cm indicated “no pain” and 10 cm “maximal pain”. The signal from the VAS was recorded continuously (sampling frequency of 0.5 Hz), allowing the subjects to update the values whenever needed by adjusting an external handheld slider with the contralateral hand (not involved in the exercise). Subjects were asked to focus on the VAS in the intervals between individual trials, and after completing the series of submaximal trials.
Force recordings
A six-axis force sensor (MC3A 250, AMTI, USA) with high sensitivity (0.054, 0.054, 0.0134 V/N for Fx, Fy, Fz; and 2.744, 2.744, 2.124 V/Nm for Mx, My, Mz) was used during all experiments, yielding three force components (Fig. 1) and three moment components. Providing recordings of normal force (Fz, against the surface of the sensor) and tangential forces (Fx, Fy), this sensor allows the assessment of three-dimensional changes in the angle of force production (i.e. deviations from a purely normal orientation) by calculating the angles between the resultant force and each of the tangential directions [Fig. 1; angle θ ZX = atan(Fx/Fz); angle θ ZY = atan(Fy/Fz)]. Centre of pressure (CoP) was extracted based on the three-dimensional force and torque signals (AMTI, USA). The sensor was mounted in different custom-built setups, as shown in Fig. 1a–d, allowing isometric contractions of the different muscle groups. The analogue output of the sensor was low-pass filtered at 1 kHz, amplified (MSA-6, AMTI, USA), sampled at 2 kHz, and stored after 12 bits A/D conversion.
Dorsiflexion
Subjects were seated in a heavy chair and placed the dominant foot on a custom pedal, with the sensor secured above the metatarsal phalangeal joints. The pedal could be adjusted for different foot lengths, and was connected to a metal frame with a rotating arm, allowing changes of the lower leg angle. The angle between the foot and the tibia was 90°, the knee was extended at 120° (180° = straight leg), and the hip flexed at 90°. The dominant thigh was strapped and the arms were crossed in front of the chest (Fig. 1a).
Elbow flexion
Subjects were seated in a heavy chair and rested the dominant elbow and the forearm on a padded support, with the sensor secured above the wrist. The dominant upper arm was vertical and slightly abducted, the elbow flexed at 90°, and the hand was kept vertically aligned to the sagittal plane with closed fist, while the non-dominant arm was held in front of the chest, and subjects were instructed not to move the legs (Fig. 1b).
Knee extension
Subjects were seated in a heavy chair. A pair of L-shaped bars was fixed vertically to the chair and horizontally to a metal plate. The sensor was secured to this metal plate and adjusted to 5 cm above the medial malleolus of the dominant leg of each subject. The hip was flexed at 90° and the knee extended at 120° (180° = straight leg). The dominant thigh was strapped and the arms were crossed in front of the chest (Fig. 1c).
Plantarflexion
Subjects were seated in a chair and placed the dominant foot on a custom pedal, with the metatarsal phalangeal joints on the sensor. The sensor was mounted under, and protruded through, a pedal which allowed adjustments for different foot lengths, and the pedal was fixed to the ground. The hip and the knee were flexed at 90°, and the angle between the foot and the tibia was 90°. The dominant thigh was strapped, preventing the heel from lifting off the pedal, and the arms were crossed in front of the chest (Fig. 1d).
Surface electromyography
The electromyography (EMG) signals of the relevant agonist and antagonist muscles were recorded: m. gastrocnemius medialis (GM), m. gastrocnemius lateralis (GL), m. soleus (SO), and m. tibialis anterior (TA) during both dorsi- and plantarflexions; m. biceps brachii (BB), m. brachioradialis (BRR), and m. triceps brachii (TRB) during elbow flexions; m. rectus femoris (RF), m. vastus lateralis (VL), m. vastus medialis (VM), m. biceps femoris (BF), and m. semitendinosus (ST) during knee extensions. All EMG signals were measured by a pair of disposable Ag/AgCl surface electrodes (Ambu Neuroline 720, length × width 4.5 × 2 cm, Denmark) in bipolar configuration, placed 2 cm apart and positioned according to standard recommendations (Hermens et al. 2000). Signals were amplified (Counterpoint MK2, Dantec, Denmark), band-pass filtered (10–1,000 Hz), sampled at 2 kHz, and stored after 12 bits A/D conversion.
Data analysis
The force and moment signals were low-pass filtered using a Butterworth filter of second order with a cut-off frequency of 20 Hz. The EMG signals were digitally band-pass filtered at 20–400 Hz using a Butterworth filter of second order, and the integrated EMG (iEMG) was calculated over epochs of 1 s by the integral of the full-wave rectified, low-pass filtered (50 Hz, second order Butterworth) EMG signal (Ervilha et al. 2005).
From the MVC task, the peak iEMG of each muscle was extracted and used to normalize the iEMG during submaximal target force contractions. For each submaximal contraction, the absolute mean forces in all directions, the mean absolute force angles and total range of force angles, the standard deviation (SD) of the three force components, the coefficient of variation (CV) of force (SD/mean force), the total excursion of the CoP, and the mean normalized iEMG were assessed using a time window of 6 s (3 s after end of ramp, Fig. 2), which avoided excessive fluctuations due to slow force development and anticipation of trial termination in the beginning and end of contractions, respectively. The CV of force was not used to assess the variability of tangential force components because the magnitude of the tangential forces approached zero during some trials, leading to inconsistently high values of the CV. Alternatively, the use of miniature multi-axis force and torque sensors allows the assessment of CoP variability of individual body segments during static contractions, e.g. fingers during grasp tasks (Zhang et al. 2010, 2011). Corroborating this approach, a strong correlation has been shown between muscle lateral displacements and force fluctuations during isometric contractions (Yoshitake et al. 2008). Hence, the current study indirectly assessed the variability of tangential forces by the total excursion of CoP, which represents the total length of the CoP path during a given time interval (Prieto et al. 1996), thus assessing the lateral displacements of quasi-static forces. VAS scores were recorded during all contractions and the mean VAS score was extracted from the same time window used for the force parameters.

Representative task-related (Fz) and tangential (Fx, Fy) force signals, and EMG signals (m. biceps brachii) recorded during isometric elbow flexions at 50% MVC force following injections of isotonic (non-painful) and hypertonic (painful) saline into the m. brachioradialis. The shaded area represents the time window used for data analysis
Statistical analysis
For all force-matched tasks, mean VAS scores, mean iEMG, and all force parameters were assessed using a three-way repeated measures analysis of variance (RM-ANOVA) with injection (isotonic, hypertonic), condition (pre, during, post), and force (2.5, 20, 50, 70% MVC force) as within-subject factors. Because of their opposing functional actions, RM-ANOVAs were applied independently to the iEMG of agonist and antagonist muscles. Statistical significance was considered for P values lower than 0.05 and Newman–Keuls (NK) post hoc test was applied when appropriate. All results are reported as mean ± standard error of the mean (SEM).
Results
Experimental muscle pain
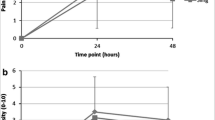
Hypertonic saline injection induced significantly higher mean VAS scores than isotonic saline injection during isometric contractions of all muscle groups (Fig. 3; RM-ANOVA: F 1,13–14 > 42.6, P < 0.001; NK: P < 0.001). VAS scores were zero during pre and post conditions.

Mean (±SEM, shaded area) VAS scores after intramuscular injection of hypertonic (HYP) and isotonic (ISO) saline. Submaximal isometric contractions were restricted to the initial 3 min following injection, during which hypertonic injections elicited higher pain than isotonic injections. Injections were performed into the m. tibialis anterior for dorsiflexors, m. brachioradialis for elbow flexors, m. vastus medialis for knee extensors, and m. gastrocnemius medialis for plantarflexors
Force magnitude and angle
Pain had no significant effect in the absolute mean force in task-related and tangential directions or in the absolute mean θZX and θZY angles (Fig. 4; RM-ANOVA: F 2,26–28 < 2.81, P > 0.077). Further analysis using the absolute difference with respect to baseline trials also showed no significant effects of pain on the mean force magnitude and mean force angle (data not shown). Although multiple injection × condition interactions in the RM-ANOVA of the range of force angles suggested consistent increases in the painful compared with non-painful conditions, post hoc analysis revealed significant differences only in the range of θZX during plantarflexions and θZY during knee extensions (Fig. 4; RM-ANOVA: F 2,26–28 > 3.92, P < 0.033; NK: P < 0.017).

Mean (+SEM) of basic force parameters: mean absolute force (Fx, Fy, Fz), mean absolute angle (θzx and θzy), and range of angle (θzx and θzy) during isometric dorsiflexions (DF), elbow flexions (EF), knee extensions (KE), and plantarflexions (PF). Each bar represents the average across all target forces as no interaction effects were detected between injection type, pain condition and the target force. The ranges of the θzx angle during plantarflexions and the θzy angle during knee extensions were increased during pain compared with all other injection conditions (asterisk, NK: P < 0.033)
Force steadiness
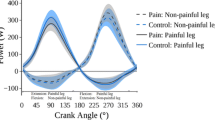
A main effect of force in the RM-ANOVA of the SD of force in the three directions revealed a general increase with higher target forces (Fig. 5, RM-ANOVA: F 3,39–42 > 13.378, P < 0.0001; NK P < 0.0038). Moreover, the SD of force was not significantly affected by pain, except for an increase in the SD of task-related force during painful compared with non-painful knee extensions at 70% MVC (F 6,78 = 2.4428, P = 0.0323; NK P = 0.0001, not shown). CV of force (Fig. 6b; RM-ANOVA: F 2,26–28 > 4.82, P < 0.015; NK: P < 0.03) and total excursions of CoP (Fig. 6d; RM-ANOVA: F 2,26–28 > 4.16, P < 0.027; NK: P < 0.002) were higher following painful compared with control injections for all muscle groups and, except for dorsiflexors, also higher than pre and post injection conditions (NK: P < 0.03). During plantarflexions, an Injection × Condition × Force interaction revealed increased total excursions of CoP during pain compared with other conditions only at 2.5% MVC (RM-ANOVA: F 6,84 = 2.37, P = 0.036; NK: P < 0.001).

Mean (±SEM) standard deviation (SD) of task-related (Fz) and tangential (Fx, Fy) forces and integrated electromyography (iEMG) of agonist and antagonist muscles. The parameters increased monotonically with higher target forces for all muscle groups (NK: P < 0.001). Each symbol represents the average across all injection conditions (hypertonic and isotonic injections, pre, during and post conditions) as these were not significantly different

Mean (±SEM) coefficient of variation (CV) of force and total excursion of the CoP during isometric dorsiflexions (DF), elbow flexions (EF), knee extensions (KE), and plantarflexions (PF). Experimental muscle pain consistently increased the variability of task-related and tangential forces compared with control injection for all muscle groups (a, c each bar represents the average across all target forces). A cubic polynomial shape was observed for both parameters with increasing target forces (b, d comparing trials performed immediately following injections of isotonic (ISO) and hypertonic (HYP) saline). *Significantly higher than control injection, NK: P < 0.03, **significantly higher than control injection and both pre and post injection conditions, NK: P < 0.03, †significantly higher than control injection and both pre and post injection conditions only at 2.5% of MVC force, NK: P < 0.001
Muscle activity
A main effect of force in the RM-ANOVA of the mean iEMG of all muscle groups revealed a monotonic increase in muscle activity with higher target forces for agonist (Fig. 5, RM-ANOVA: F 3,39–42 > 183.73, P < 0.0001, NK: P < 0.0015) and antagonist muscles (Fig. 5, RM-ANOVA: F 3,39–42 > 27.225, P < 0.0001, NK: P < 0.044), although the increase in antagonist muscle activity was not significant between 2.5 and 20% MVC during dorsi- and plantarflexions. There were no significant differences in the level of activation of any of the observed muscles between painful and non-painful conditions.
Discussion
Experimental muscle pain elicited task-specific increase in the ranges of force angle compared with control assessments, although changes in mean force magnitude and direction were not statistically significant. The present data show for the first time that experimental muscle pain elicits higher fluctuations of task-related and tangential force components, i.e. higher CV of force and total excursions of CoP, during sustained contractions of different muscle groups. No changes were detected in the iEMG of any of the assessed muscles during painful contractions.
Multidirectional force fluctuations and pain
An unanimous finding among previous studies assessing three-dimensional steadiness of static forces is a monotonic increase in the SD of the three force components when increasing target forces (Hong et al. 2007; Svendsen and Madeleine 2010; Salomoni and Graven-Nielsen 2012), which is further supported by the present data. This increase in SD with target force is related to the orderly recruitment of motor units: to increase muscle force, larger motor units are recruited (Henneman et al. 1965), which produce larger and unfused twitches, resulting in increased force fluctuations (Jones et al. 2002). Because the resultant force represents the spatial summation of activity from different muscles, each contributing to fluctuations on its own direction of action (Kutch et al. 2008), an overall increase in muscle activity modulates task-related and tangential forces similarly (Hong et al. 2007; Svendsen and Madeleine 2010), as observed in Fig. 5. In fact, the orientation of forces produced by individual motor units within each muscle is slightly different according to muscle fibre angle and attachments (Herrmann and Flanders 1998) and, even in the case of a single active muscle, the exerted force is not kept purely mono-directional during the contraction. Consistent with these arguments, previous studies reported: (1) varying degrees of coordination of index finger muscles in relation to different directions and magnitudes of endpoint forces (Kutch et al. 2008); and (2) heterogeneity of activation within the triceps surae muscle in relation to force directions, with subject-specific variations in the degree of heterogeneity (Staudenmann et al. 2009).
Increased variability of force and movement has been associated with the development of musculoskeletal disorders and pain (Madeleine 2010), such as knee osteoarthritis and subacromial impingement syndrome (Hortobágyi et al. 2004; Bandholm et al. 2006). However, in patients with chronic conditions it is impossible to distinguish whether changes in motor function are caused by pain, inflammatory or structural changes, or disuse of the affected joint or muscles. Previous investigations on force fluctuations using experimental pain models have focused on the assessment of a single force component, showing increases of fluctuations during moderate level (20–35% MVC) contractions of the finger, arm, and shoulder muscles (Del Santo et al. 2007; Bandholm et al. 2008). The present results extend these findings by demonstrating that acute pain evoked by intramuscular injections of hypertonic saline elicits an increase of force fluctuations in task-related and tangential forces during static contractions of the ankle, elbow, and knee muscles over a wide range of force levels.
Multiple neuromuscular mechanisms could be responsible for the pain-induced increase in force fluctuations. First, experimental muscle pain reduces motor unit firing rates and elicits a spatial reorganization of muscle activity during sustained contractions, with no changes in muscle fibre membrane properties (Farina et al. 2004; Madeleine et al. 2006). Hence, the observed changes may reflect an adaptation of the motor strategy within and between muscles in an attempt to maintain a constant force output during pain. The increased range of force angle observed during painful knee extensions and plantarflexions (Fig. 4) reflects higher changes in the direction of force, suggesting that the reorganization of muscle activity can occur during the course of the required task. Second, it has been shown that hypertonic saline excites groups III and IV afferent fibres (Kumazawa and Mizumura 1977), which converge on common interneurons in pathways from group Ia and Ib afferents (muscle spindles and Golgi tendon organs) (Schomburg et al. 1999). Inhibitory pathways converging into group Ia afferents decrease excitatory input to alpha-motoneurons, hence modulating force fluctuations (Yoshitake et al. 2004; Shinohara et al. 2005). In addition, spatial facilitation between groups III and IV muscle afferents and Ib afferents may modulate the sensitivity of muscle tension control by decreased reflex sensitivity in agonist muscles and increased reflex sensitivity in antagonist muscles (Graven-Nielsen et al. 2002), modifying the ability of the central nervous system to interpret proprioceptive information needed to precisely control force or position of the limbs (Wessberg and Vallbo 1995). Third, increased synchronization of motor units may have contributed to higher force fluctuations (Yao et al. 2000).
The SD of force is mainly influenced by the intensity of muscle contraction (Jones et al. 2002), and the absence of significant changes in iEMG during pain could explain why no differences in the SD of force were observed across different pain conditions. On the other hand, normalized measures of motor output variability (e.g. CV of force) are sensitive to motor unit recruitment and discharge behaviour (Taylor et al. 2003; Moritz et al. 2005), and the increased CV of force support the involvement of changes in the motor unit population during pain. Since the CoP time series is inversely proportional to the task-related force, the total excursion calculated over the CoP time series can also be considered a normalized parameter. Furthermore, supporting the idea that fluctuations in task-related and tangential forces are governed by similar, or synergistic, mechanisms (Hong et al. 2007; Svendsen and Madeleine 2010; Salomoni and Graven-Nielsen 2012), the present results show increased total excursions of the CoP and the CV of force during pain compared to baseline for all the assessed muscle groups (Fig. 6b, d), as predicted by the second hypothesis.
It has been shown that delayed onset muscle soreness elicited by eccentric exercises increases force variability, particularly at low (<10% MVC) compared with high forces due to greater increase in muscle activity and larger relative effect of changes in single motor unit behaviour (Lavender and Nosaka 2006; Semmler et al. 2007). In contrast, although in the present study high levels of force variability were observed at 2.5% MVC force (Fig. 6a, c), experimental muscle pain consistently increased force fluctuations regardless of force level, illustrating that distinct mechanisms are evoked by the different pain models. Although not supporting the third hypothesis, the current results are consistent with the previous findings showing that experimental muscle pain also attenuates the kinematics of dynamic arm movements regardless of load level (Ervilha et al. 2004).
Pain-adaptation strategy
In contrast to the first hypothesis, the orientation of the resultant force vector was not significantly changed during pain, probably because no substantial changes occurred in the mean level of muscle activity, as assessed by surface EMG. As a result, subjects were still able to sustain the same mean level of motor output in both conditions despite significant increases in fluctuations of task-related and tangential forces during painful when compared with non-painful conditions. Although inconsistent with the homogeneous inhibition of agonist muscles predicted by the pain-adaptation model (Lund et al. 1991), these results are supported by a number of studies that have also reported no pain-induced changes in EMG during static contractions (Graven-Nielsen et al. 1997; Birch et al. 2000; Hodges et al. 2008). Nevertheless, the increased variability in three-dimensional force output observed in the present study must ultimately result from changes in the activity or coordination of the involved muscles. Thus, it is likely that multiple mechanisms, such as recruitment of additional motor units (Graven-Nielsen et al. 1997), reduced motor unit firing rates (Farina et al. 2004), and increased motor unit synchronization (Hodges et al. 2008), acted simultaneously and balanced the magnitude of the detected surface EMG, overcoming potential inhibitory effects associated with pain. This is in line with the recent findings by Tucker and Hodges (2009), who reported non-uniform changes in the motoneuron pool detected using fine-wire intramuscular electrodes during painful knee extensions, while the amplitude of bipolar surface EMG was not affected.
The absence of changes in the mean force direction contrast with previous findings (Tucker and Hodges 2010) and could reflect a methodological limitation of the present study. Due to the wide range of motor strategies that may be used to sustain a submaximal target force, a long acquisition time is required to account for variations over time and provide a reliable baseline reference for the mean force angle (Tucker and Hodges 2010). However, this was not possible in the case of the high target forces assessed in the current study (50 and 70% MVC), and the time window used for analysis (6 s) was probably too small to estimate a stable reference. Nevertheless, in agreement with the aforementioned study, an increased range of force angle was observed during pain when compared with baseline (Tucker and Hodges 2010), but only during knee extensions and plantarflexions, suggesting task-dependent pain adaptations. Because stronger muscles require a larger motor unit population to develop the same relative force level compared with weaker muscles, it is likely that pain-induced reorganization of muscle activity was greater in the stronger PF and KE as compared to the weaker DF and EF. The substitution of a larger number of motor units may lead to greater misalignments of the resultant force vector (Kutch et al. 2008), which could explain the higher changes in force angle in stronger muscles.
Furthermore, computer model simulations have confirmed that force fluctuations are very sensitive to changes in motor unit recruitment strategy and spatial reorganization of active motor units (particularly at low force levels) (Fuglevand et al. 1993; Taylor et al. 2003), which are commonly reported by experimental pain studies using intramuscular and multi-channel surface EMG electrodes (Madeleine et al. 2006; Falla et al. 2007; Tucker and Hodges 2010). Although it has been suggested that pain adaptations in muscle function typically aim at the protection of the painful site against further pain or injury (Hodges and Tucker 2011), the present data show that they may also result in impairments in the steadiness of force.
Conclusions
Experimental muscle pain increased the range of angle in the resultant force as well as the normalized fluctuations of task-related and tangential forces during isometric contractions of different muscle groups across all the target forces assessed (2.5–70% MVC), with no changes in the absolute mean force level or the mean force angle. The decreased force steadiness probably resulted from dynamic and subject-specific spatial redistribution of activity within and between muscles, which could not be detected by surface electromyography. The present data show that pain-induced adaptations in muscle function lead to impairments in the steadiness of task-related and tangential force components.
References
Bandholm T, Rasmussen L, Aagaard P, Jensen BR, Diederichsen L (2006) Force steadiness, muscle activity, and maximal muscle strength in subjects with subacromial impingement syndrome. Muscle Nerve 34:631–639
Bandholm T, Rasmussen L, Aagaard P, Diederichsen L, Jensen BR (2008) Effects of experimental muscle pain on shoulder-abduction force steadiness and muscle activity in healthy subjects. Eur J Appl Physiol 102:643–650
Birch L, Christensen H, Arendt-Nielsen L, Graven-Nielsen T, Søgaard K (2000) The influence of experimental muscle pain on motor unit activity during low-level contraction. Eur J Appl Physiol 83:200–206
Carville SF, Perry MC, Rutherford OM, Smith ICH, Newham DJ (2007) Steadiness of quadriceps contractions in young and older adults with and without a history of falling. Eur J Appl Physiol 100:527–533
Del Santo F, Gelli F, Spidalieri R, Rossi A (2007) Corticospinal drive during painful voluntary contractions at constant force output. Brain Res 1128:91–98
Ervilha UF, Arendt-Nielsen L, Duarte M, Graven-Nielsen T (2004) Effect of load level and muscle pain intensity on the motor control of elbow-flexion movements. Eur J Appl Physiol 92:168–175
Ervilha UF, Farina D, Arendt-Nielsen L, Graven-Nielsen T (2005) Experimental muscle pain changes motor control strategies in dynamic contractions. Exp Brain Res 164:215–224
Falla D, Farina D, Graven-Nielsen T (2007) Experimental muscle pain results in reorganization of coordination among trapezius muscle subdivisions during repetitive shoulder flexion. Exp Brain Res 178:385–393
Farina D, Arendt-Nielsen L, Merletti R, Graven-Nielsen T (2004) Effect of experimental muscle pain on motor unit firing rate and conduction velocity. J Neurophysiol 91:1250–1259
Fuglevand AJ, Winter DA, Patla AE (1993) Models of recruitment and rate coding organization in motor-unit pools. J Neurophysiol 70:2470–2488
Graven-Nielsen T (2006) Fundamentals of muscle pain, referred pain, and deep tissue hyperalgesia. Scand J Rheumatol 35:1–43
Graven-Nielsen T, Svensson P, Arendt-Nielsen L (1997) Effects of experimental muscle pain on muscle activity and co-ordination during static and dynamic motor function. Electroencephalogr Clin Neurophysiol 105:156–164
Graven-Nielsen T, Lund H, Arendt-Nielsen L, Danneskiold Samsøe B, Bliddal H (2002) Inhibition of maximal voluntary contraction force by experimental muscle pain: a centrally mediated mechanism. Muscle Nerve 26:708–712
Henneman E, Somjen G, Carpenter DO (1965) Functional significance of cell size in spinal motoneurons. J Neurophysiol 28:560–580
Hermens HJ, Freriks B, Disselhorst-Klug C, Rau G (2000) Development of recommendations for SEMG sensors and sensor placement procedures. J Electromyogr Kinesiol 10:361–374
Herrmann U, Flanders M (1998) Directional tuning of single motor units. J Neurosci Methods 18:8402–8416
Hodges PW, Tucker K (2011) Moving differently in pain: a new theory to explain the adaptation to pain. Pain 152:S90–S98
Hodges PW, Ervilha UF, Graven-Nielsen T (2008) Changes in motor unit firing rate in synergist muscles cannot explain the maintenance of force during constant force painful contractions. J Pain 9:1169–1174
Hong SL, Lee MH, Newell KM (2007) Magnitude and structure of isometric force variability: mechanical and neurophysiological influences. Mot Control 11:119–135
Hortobágyi T, Garry J, Holbert D, Devita P (2004) Aberrations in the control of quadriceps muscle force in patients with knee osteoarthritis. Arthritis Rheum 51:562–569
Jones KE, Hamilton AFC, Wolpert DM (2002) Sources of signal-dependent noise during isometric force production. J Neurophysiol 88:1533–1544
Kumazawa T, Mizumura K (1977) Thin-fibre receptors responding to mechanical, chemical, and thermal stimulation in the skeletal muscle of the dog. J Physiol 273:179–194
Kutch JJ, Kuo AD, Bloch AM, Rymer WZ (2008) Endpoint force fluctuations reveal flexible rather than synergistic patterns of muscle cooperation. J Neurophysiol 100:2455–2471
Lavender AP, Nosaka K (2006) Changes in fluctuation of isometric force following eccentric and concentric exercise of the elbow flexors. Eur J Appl Physiol 96:235–240
Lund JP, Donga R, Widmer CG, Stohler CS (1991) The pain-adaptation model: a discussion of the relationship between chronic musculoskeletal pain and motor activity. Can J Physiol Pharm 69:683–694
Madeleine P (2010) On functional motor adaptations: from the quantification of motor strategies to the prevention of musculoskeletal disorders in the neck-shoulder region. Acta Physiol 199:1–46
Madeleine P, Leclerc F, Arendt-Nielsen L, Ravier P, Farina D (2006) Experimental muscle pain changes the spatial distribution of upper trapezius muscle activity during sustained contraction. Clin Neurophysiol 117:2436–2445
Missenard O, Mottet D, Perrey S (2009) Factors responsible for force steadiness impairment with fatigue. Muscle Nerve 40:1019–1032
Moritz CT, Barry BK, Pascoe MA, Enoka RM (2005) Discharge rate variability influences the variation in force fluctuations across the working range of a hand muscle. J Neurophysiol 93:2449–2459
Prieto TE, Myklebust JB, Hoffmann RG, Lovett EG, Myklebust BM (1996) Measures of postural steadiness: differences between healthy young and elderly adults. IEEE Trans Biomed Eng 43:956–966
Salomoni SE, Graven-Nielsen T (2012) Muscle fatigue increases the amplitude of fluctuations of tangential forces during isometric contractions. Hum Mov Sci (in press). http://dx.doi.org/10.1016/j.humov.2011.08.012
Schomburg ED, Steffens H, Kniffki KD (1999) Contribution of group III and IV muscle afferents to multisensorial spinal motor control in cats. Neurosci Res 33:195–206
Semmler JG, Tucker KJ, Allen TJ, Proske U (2007) Eccentric exercise increases EMG amplitude and force fluctuations during submaximal contractions of elbow flexor muscles. J Appl Physiol 103:979–989
Shinohara M, Moritz CT, Pascoe MA, Enoka RM (2005) Prolonged muscle vibration increases stretch reflex amplitude, motor unit discharge rate, and force fluctuations in a hand muscle. J Appl Physiol 99:1835–1842
Staudenmann D, Kingma I, Daffertshofer A, Stegeman DF, van Dieën JH (2009) Heterogeneity of muscle activation in relation to force direction: a multi-channel surface electromyography study on the triceps surae muscle. J Electromyogr Kinesiol 19:882–895
Stein RB, Gossen ER, Jones KE (2005) Neuronal variability: noise or part of the signal? Nat Rev Neurosci 6:389–397
Svendsen JH, Madeleine P (2010) Amount and structure of force variability during short, ramp and sustained contractions in males and females. Hum Mov Sci 29:35–47
Taylor AM, Christou EA, Enoka RM (2003) Multiple features of motor-unit activity influence force fluctuations during isometric contractions. J Neurophysiol 90:1350–1361
Tracy BL (2007) Force control is impaired in the ankle plantarflexors of elderly adults. Eur J Appl Physiol 101:629–636
Tracy BL, Mehoudar PD, Ortega JD (2007) The amplitude of force variability is correlated in the knee extensor and elbow flexor muscles. Exp Brain Res 176:448–464
Tucker KJ, Hodges PW (2009) Motoneurone recruitment is altered with pain induced in non-muscular tissue. Pain 141:151–155
Tucker KJ, Hodges PW (2010) Changes in motor unit recruitment strategy during pain alters force direction. Eur J Pain 14:932–938
Wessberg J, Vallbo AB (1995) Coding of pulsatile motor output by human muscle afferents during slow finger movements. J Physiol 485:271–282
Yao W, Fuglevand RJ, Enoka RM (2000) Motor-unit synchronization increases EMG amplitude and decreases force steadiness of simulated contractions. J Neurophysiol 83:441–452
Yoshitake Y, Shinohara M, Kouzaki M, Fukunaga T (2004) Fluctuations in plantar flexion force are reduced after prolonged tendon vibration. J Appl Physiol 97:2090–2097
Yoshitake Y, Masani K, Shinohara M (2008) Laser-detected lateral muscle displacement is correlated with force fluctuations during voluntary contractions in humans. J Neurosci Methods 173:271–278
Zhang W, Gordon AM, Fu Q, Santello M (2010) Manipulation after object rotation reveals independent sensorimotor memory representations of digit positions and forces. J Neurophysiol 103:2953–2964
Zhang W, Gordon AM, McIsaac TL, Santello M (2011) Within-trial modulation of multi-digit forces to friction. Exp Brain Res 211:17–26
Acknowledgments
The study has been financed by Svend Andersen Fonden (Aalborg, Denmark). Dr. Hong-You Ge, Center for Sensory-Motor Interaction (Aalborg University, Denmark), is acknowledged for his help with the experimental procedure.
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Additional information
Communicated by Toshio Moritani.
Rights and permissions
About this article
Cite this article
Salomoni, S.E., Graven-Nielsen, T. Experimental muscle pain increases normalized variability of multidirectional forces during isometric contractions. Eur J Appl Physiol 112, 3607–3617 (2012). https://doi.org/10.1007/s00421-012-2343-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-012-2343-7