
Abstract
It is well established that the loss of muscle mass (i.e. sarcopenia) is the primary factor contributing to the reduction in muscle force with ageing. Based on the observation that force declines at a faster rate than muscle mass, neural alterations are also thought to contribute to muscle weakness by reducing central drive to the agonist muscles and by increasing coactivation of the antagonist muscles. Researchers have attempted to quantify the contribution of impaired voluntary drive to the decline in muscle force using superimposed electrical stimulation during maximal voluntary contractions (MVCs) and by recording surface electromyographic (EMG) activity. Although reduced voluntary activation of agonist muscles and increased coactivation of antagonist muscles during a MVC have been reported with advancing age, such changes are not supported by all studies. These discrepancies may be explained by differences in sensitivity between the methods used to assess voluntary activation, as well as differences between the characteristics of the study population, the muscle group that is tested, and the type of contraction that is performed. The objective of this review is to summarize current knowledge regarding the activation of agonist and antagonist muscles during MVC in elderly and to try to clarify the disparities in literature concerning the influence of a possible deficit in voluntary activation on the maximal force capacity of muscles in elderly adults.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The decline in maximal voluntary force in the elderly is related to a number of alterations affecting the musculoskeletal and nervous systems. Ageing is associated with reduced muscle mass (i.e. sarcopenia) due to the loss of muscle fibres (Frontera et al. 1991; Lexell 1993) and atrophy of type II fibres (Lexell 1993). A concomitant slowing of muscle contractile properties has also been observed with advancing age (Baudry et al. 2005; Vandervoort and McComas 1986; Winegard et al. 1997). The slower contractile kinetics are primarily caused by a reduced rate of cross-bridge cycling (D’Antona et al. 2003; Hook et al. 2001) and alterations in excitation–contraction coupling (Hunter et al. 1999; Kent-Braun and Ng 1999; Payne and Delbono 2004), in addition to enhanced tendon compliance which can also reduce the rate of force development (Narici and Maganaris 2006). Age-related adaptations recorded at the whole muscle level are also associated with a profound remodelling of the motor unit (MU) structure (Roos et al. 1997), which consists of a motor neurone, its axon, and the muscle fibres that the axon innervates. The number of MUs is reduced with ageing due to the progressive death of motor neurones. However, MU size (Doherty and Brown 1993; McNeil et al. 2005) and innervation ratio (Campbell et al. 1973) are greater in elderly compared with young adults due to the reinnervation of some denervated muscle fibres by surviving motor neurones.
In addition to changes within the muscle, alterations in the central neural command that result in impaired agonist activation and/or increased antagonist coactivation (Bilodeau et al. 2001; Izquierdo et al. 1999; Macaluso et al. 2002; Morse et al. 2004) might contribute to the decline in maximal force capacity commonly observed in older adults. Whereas a consensus exists in the literature regarding alterations within the muscle of elderly adults, results related to the ability of the central nervous system to fully activate a muscle during a maximal voluntary contraction (MVC) are conflicting (Bilodeau et al. 2001; De Serres and Enoka 1998; Kent-Braun and Ng 1999; Klass et al. 2005a; Macaluso and De Vito 2004; Morse et al. 2004; Pousson et al. 2001; Roos et al. 1999; Simoneau et al. 2005; Stevens et al. 2003). The aim of this brief review is to summarize current knowledge regarding voluntary activation of agonist muscles and coactivation of antagonist muscles during MVCs in elderly adults, including some recent results collected within the framework of the "Better-Ageing" project (Baudry et al. 2005; Klass et al. 2005a, 2005b; Morse et al. 2005; Ochala et al. 2004; Simoneau et al. 2005). Our primary objective was to clarify disparities in literature regarding the contribution of neural mechanisms to force deficits in the elderly.
Voluntary activation
Maximal activation of muscle by the nervous system is influenced by the excitability of cortical neurones and motor neurones at the spinal cord. Using single transcranial magnetic stimulation, Eisen et al. (1991) observed a reduced motor evoked potential and Pitcher et al. (2003) reported that higher intensities are required to achieve the same maximal motor output in elderly subjects compared with young adults. Although both these studies suggest changes in the excitability of the cortico-spinal pathway, the results do not necessarily reflect submaximal activation during a MVC in elderly adults.
Voluntary activation, commonly defined as the level of neural drive to muscles during a maximal contraction (Allen et al. 1998), has been assessed by different methods. However, no definitive answer can be drawn from the existing literature as to whether voluntary activation during MVC is modified with ageing. Part of the discrepancy may be ascribed to differences in the age and physical condition of the elderly and young groups that were compared. Other factors that make it difficult to compare the results of existing studies include differences in the sensitivity of the method used to assess voluntary activation, the muscle group that is tested, and the type of contraction that is performed.
Methods and testing procedures
Stimulation methods
A widely used technique to test the ability of an individual to achieve complete activation of a muscle during an isometric MVC is the interpolated torque (IT), introduced by Merton (1954). This technique involves delivering a single (Belanger and McComas 1981; Vandervoort and McComas 1986), paired (Roos et al. 1999) or train (Kent-Braun and Ng 1999) of supramaximal stimuli to the motor axons of the contracting muscle(s) during MVC. The superimposed stimulation is assumed to recruit muscles fibres that are not activated by the voluntary effort. If the electrical stimulation does not evoke any additional torque, the muscle is considered to be fully activated, whereas voluntary activation is considered to be sub-maximal when torque is increased by the stimulation. The magnitude of voluntary activation is usually quantified by the ratio of the superimposed torque during the MVC to the evoked torque measured at rest either before or after the MVC (IT ratio). Voluntary activation is typically expressed as a percentage and is calculated as follows: (1−superimposed torque/control torque)×100 (Allen et al. 1998; Bigland-Ritchie et al. 1983). Another technique involves calculating the “central activation ratio” (CAR; see Kent-Braun and Le Blanc 1996). The CAR is defined as the proportion of the total muscle torque that is due to voluntary torque production, and is calculated as follows: CAR = MVC/(MVC + superimposed torque). A CAR of 1.0 indicates complete activation, whereas a value of less than 1.0 indicates a deficit in central activation.
Some studies (Herbert and Gandevia 1999; Kent-Braun and Le Blanc 1996; Miller et al. 1999) have suggested that the use of single or paired stimuli may overestimate the magnitude of voluntary activation and may not be sensitive enough to detect activation failure during contractions above 90% MVC. The argument is that the torque produced by a single stimulus represents only a small fraction of the MVC and does not allow for the summation of forces that occurs during repetitive stimulation (Kent-Braun and Le Blanc 1996). In addition, the amplitude of the evoked force may be reduced by collisions of the antidromic volley with the efferent voluntary drive, or reflex effects induced by the electrical stimulation (see Herbert and Gandevia 1999). Some researchers have used trains of stimuli in order to minimize these limitations (Kent-Braun and Le Blanc 1996; Stevens et al. 2003). In contrast, others did not observe any significant difference in the estimated level of voluntary activation when comparing the use of single, paired or trains of stimuli (Allen et al. 1998; Behm et al. 1996).
The use of different approaches (IT ratio or CAR) to quantify voluntary activation may also lead to divergent conclusions when comparing different subject populations. Unfortunately, only very few studies have compared voluntary activation calculated by the IT ratio and the CAR methods on the same group of subjects. Behm et al. (2001) observed that the IT ratio revealed a greater activation deficit than the CAR method for the leg extensor muscles. However, in a recent study comparing voluntary activation of the ankle plantarflexor muscles in elderly and young adults, Morse et al. (2005) reported a significant difference between the IT ratio and CAR methods only when the muscle was tested in a lengthened position. Voluntary activation was greater when estimated by the CAR compared with the IT ratio method only for the elderly group when tested with the ankle in a dorsiflexed position. These results are in agreement with our recent publication (Klass et al. 2005a) showing a small tendency toward greater voluntary activation (∼1–2%) of the ankle dorsiflexors when calculated by the CAR method compared with the IT ratio.
Single or paired stimulation is the most frequently used approach in studies of motor function with advancing age. This is mainly because single and paired stimuli are less painful and more easily tolerated by subjects who are not familiar with electrical stimulation. Conclusions regarding the ability of elderly subjects to achieve maximal voluntary activation appear to depend partly on whether the studies used single, paired or trains of stimuli (Table 1). For example, in the quadriceps and biceps brachii muscle groups, a superimposed train of stimuli revealed a greater difference in voluntary activation between elderly and young subjects (Bilodeau et al. 2001; De Serres and Enoka 1998; Stackhouse et al. 2001; Stevens et al. 2003) compared with single or paired stimuli (Klein et al. 2001; Roos et al. 1999). However, differences between these stimulation methods are usually very small. Furthermore, most studies that did not detect a significant difference in voluntary activation between elderly and young adults using paired stimuli were able to demonstrate sub-maximal activation for both age groups (Klein et al. 2001; Roos et al. 1999; Simoneau et al. 2005). Some authors, however, argue that, because the relation between force and activation is often curvilinear, even a small failure in activation may induce a substantial reduction in force during maximal or near-maximal contractions (Stackhouse et al. 2001; Stevens et al. 2003; see also Herbert and Gandevia 1999). These differing views cannot be exclusively related to the testing procedure because some studies have reported divergent results for the same muscle group when tested with the same methods (Morse et al. 2004; Simoneau et al. 2005). Conversely, even when different stimulation methods are used (Connelly et al. 1999; Kent-Braun and Ng 1999; Kent-Braun et al. 2002; Klass et al. 2005a; Lanza et al. 2004; Simoneau et al. 2005; Vandervoort and McComas 1986), elderly and young healthy subjects appear to be able to fully activate their ankle dorsiflexor muscles. However, clear deficits in voluntary activation have been observed in elderly adults who are less physically active (Harridge et al. 1999) or affected by disease (e.g. osteoarthritis; Hurley and Newham 1993).
The previously discussed approaches use a single target torque (MVC) to estimate the magnitude of voluntary activation by assuming a linear relation between the extra torque produced by electrical stimulation and the level of voluntary activation. In contrast, the extrapolation method uses the evoked torque produced by electrical stimulation during voluntary contractions performed over the range of 0–100% MVC to estimate an expected MVC. As the voluntary torque increases, the superimposed torque progressively decreases to 0 as the muscle becomes fully activated (Philipps et al. 1992). Due to the curvilinear relation between the evoked torque and voluntary torque in many muscles (Behm et al. 1996; De Serres and Enoka 1996), the regression strategy involves a non-linear function (second- or third-order polynomial) or linearization of the data by plotting the normalized evoked torque as a function of the percentage of MVC (Philipps et al. 1992). This technique appears to provide a more accurate estimate of voluntary activation compared with an interpolated twitch applied during a single MVC due to the greater signal-to-noise ratio (Behm et al. 1996; De Serres and Enoka 1998; Philipps et al. 1992).
Results from extrapolation procedures suggest that young and elderly subjects are able to fully activate their upper limb muscles (De Serres and Enoka 1998; Philipps et al. 1992). For example, De Serres and Enoka (1998) compared the magnitude of voluntary activation assessed by IT-train and extrapolated MVC procedures in the biceps brachii. These authors observed an age-related effect on voluntary activation using the IT-train method, but did not observe a difference in the ability to exert the expected MVC force. Due to the higher signal-to-noise ratio of the extrapolation method and the small difference in voluntary activation evidenced by the IT-train method, the authors concluded that elders were able to achieve a similar level of voluntary activation of the biceps brachii muscle as the young adults.
In conclusion, some of the discrepancies that appear in the literature regarding the level of voluntary activation that an individual can achieve may result from differences in the technique used (IT ratio, CAR or extrapolated MVC) and the number of stimuli that are applied (single, paired or train). Muscle length is also an important factor that must be considered when using stimulation methods to assess voluntary activation. Indeed, tendon compliance and muscle length can alter the amplitude of the superimposed and resting torque, therefore, differences in limb position may affect estimates of voluntary activation (Morse et al. 2005). These length-dependent effects are especially important to consider when testing elderly subjects because of their greater tendinous compliance (Morse et al. 2005; Narici and Maganaris 2006). Subjects’ level of familiarization with the task is an additional factor that can influence the comparison of young and elderly subjects, as demonstrated by Jakobi and Rice (2002) who reported that lower initial levels of activation in elderly subjects can be reduced if sufficient attempts are provided.
Surface electromyogram recording
Another technique often used to quantify changes in voluntary activation of the agonist or antagonist muscles is surface electromyographic (EMG). This technique measures the electrical activity of MUs located beneath recording electrodes that are placed on the skin overlying the muscle belly. The amplitude and the power spectrum of the surface EMG depend on the propagation of action potentials along the muscle fibres (Farina et al. 2004). The advantage of this technique is that it is non-invasive and provides a global estimate of muscle activation without the need to apply electrical stimulation. However, there are several limitations: (1) surface EMG is influenced by both central and peripheral factors which are difficult to differentiate; (2) surface EMG underestimates the activation signal sent from the spinal cord to muscle due to cancellation of the positive and negative phases of MU action potentials (Farina et al. 2004; Keenan et al. 2005); and (3) comparisons of surface EMG between subjects are limited by a variety of factors including differences in the thickness of subcutaneous tissues and the distribution of MU territories in the muscle (Farina et al. 2004; Keenan et al. 2005).
Due to changes in fat accumulation with ageing, the comparison of raw EMG signals between young and elderly subjects is not recommended. However, the decrease in average EMG amplitude (Esposito et al. 1996; Macaluso et al. 2002) and mean frequency of the power density spectrum (Esposito et al. 1996) observed during isometric contractions in older adults has been sometimes associated with possible change in voluntary activation. In addition to a reduction in the number and maximal discharge rate of MUs (McNeil et al. 2005) that is often reported with ageing (Connelly et al. 1999; Kamen et al. 1995), these authors nevertheless suggested that these age-related changes were partly due to greater skinfold thickness in the older adults. In contrast, we did not observe any statistical difference in the mean absolute EMG activity between elderly and young subjects for isometric MVCs in the ankle dorsiflexors (Klass et al. 2005a). The same conclusion was reached when EMGs were normalized to the M-wave amplitude obtained in response to supramaximal electrical stimulation of the motor nerve (Klass et al. 2005a). This normalization procedure controls for age-related differences in muscle membrane ionic processes and, therefore, provides an indirect measure of the subject’s ability to maximally activate the muscle group. These results are consistent with those previously reported using the superimposed stimulation technique (Klass et al. 2005a) and support the idea that elderly and young subjects achieve similar levels of voluntary activation for the ankle dorsiflexor muscles.
In conclusion, results obtained using surface EMG appear to be as variable as those using stimulation techniques to assess voluntary activation. Although the use of voluntary EMG as an index of voluntary activation can be misleading, results appear to depend on the muscle group that is tested.
Additional experimental sources of divergence
Muscle group
As discussed above, the various methods used to quantify voluntary activation during MVC may have contributed to differences reported between elderly and young adults. However, a review of the literature suggests that difference in the muscle group investigated is a prevalent factor in the discrepancy between studies (Table 1). With increasing age, most studies have observed reduced voluntary activation of proximal muscles in the upper and lower limbs during MVC (Bilodeau et al. 2001; Stackhouse et al. 2001; Stevens et al. 2001, 2003), whereas voluntary activation in more distal muscles appeared to be better preserved (Kent-Braun and Ng 1999; Kent-Braun et al. 2002; Klass et al. 2005a; Philipps et al. 1992). The observation that sub-optimal activation of larger proximal muscles reported for young subjects (Behm et al. 2001) may suggest that this effect is amplified with ageing.
Dynamic contractions and velocity
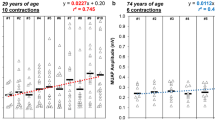
Most studies investigating age-related effects on voluntary activation have been performed during isometric contractions. Dynamic contractions are performed frequently during daily activities, therefore, a few recent studies have investigated adaptations that are specific to dynamic contractions (Klass et al. 2005a; Porter et al. 1997; Pousson et al. 2001; Vandervoort et al. 1990). Most of these studies reported greater torque preservation during maximal eccentric contractions as compared with maximal isometric and concentric torque (see Fig. 1; Klass et al. 2005a; Porter et al. 1997; Pousson et al. 2001; Vandervoort et al. 1990). In addition to changes within the muscle, the extent to which deficits in voluntary activation contribute to torque decrements that are specific to the contraction modality appears functionally relevant.

Comparison of voluntary activation (in percentage) of the ankle dorsiflexors, assessed by the superimposed stimulation method, in elderly and young subjects, and torque–velocity relation of the ankle dorsiflexors in 19 elderly and 17 young subjects. Torque is expressed in Nm, and concentric and eccentric contractions are indicated by positive and negative velocities, respectively. All values are mean ± SE. Significant difference between elderly and young subjects:*P<0.05, †P<0.01, ‡P<0.001
During dynamic contractions performed on an isokinetic dynamometer, Pousson et al. (2001) investigated the relation between muscle activity and torque produced by the biceps brachii. They found that during concentric and eccentric muscle contractions, elderly adults exhibited lower levels of EMG root mean square (RMS) compared with young adults. In addition, the RMS values obtained at high angular velocities (up to 240°/s) were lower than those at 60°/s for the elderly subjects, but higher for the young subjects. This observation suggests a different neural control strategy for the two age groups during rapid contractions. In contrast, two studies (Table 2) that have used stimulation methods to investigate possible age-related changes in voluntary activation during dynamic contractions did not observe significant activation deficits across the different velocities tested (Klass et al. 2005a; White and Harridge 1990). By comparing the force produced by each subject during maximal voluntary and electrically induced contractions (Thomas et al. 1987) at different movement speeds, White and Harridge (1990) suggested that activation of the triceps surae during concentric movements at angular velocities up to 240°/s did not differ between young and elderly men. This conclusion was based on the absence of differences in the ratio between voluntary and electrically evoked torques. Similarly, Klass et al. (2005a) showed that voluntary activation of the ankle dorsiflexors, quantified by the superimposed paired stimulation technique, was maximal or near maximal during concentric and eccentric contractions up to a velocity of 100°/s (Fig. 1). Submaximal activation was observed in very few trials during eccentric contractions in a similar proportion for elderly and young adults. Consistent with these results, the average voluntary EMG amplitude-to-M wave ratio for the tibialis anterior appeared to be similar in elderly and young adults, regardless of the type and velocity of contraction.
In conclusion, although one investigation using EMG recordings in an upper limb muscle suggested lower levels of muscle activation in the elderly (Pousson et al. 2001), studies using stimulation methods support the conclusion that both elderly and young subjects are able to fully activate their distal lower limb muscles during concentric and eccentric contractions performed at angular velocities up to 240°/s. However, these findings do not exclude the possibility that voluntary activation may be a limiting factor at very high velocities (Aagaard et al. 2002; Kent-Braun and Ng 1999). In this context, Hakkinen et al. (1998) reported lower EMG activity in elderly compared with young subjects when performing fast bilateral isometric contractions of the leg extensors. This observation indicates possible deficits in the rapid recruitment and high instantaneous discharge rate of MUs that is needed to perform very fast contractions (Van Cutsem and Duchateau 2005).
Motor unit discharge frequency
Although invasive and technically difficult to analyse during MVC, another way to assess the degree of voluntary activation is to record the recruitment and discharge frequency of single MUs. Briefly, this method involves recording the action potential of a single MU using a selective electrode that consists of two 25–100 μm diameter wires inserted into the belly of a muscle. This method cannot be used to verify that all MUs are recruited during MVC, however, it does permit the recording of maximal discharge frequencies for individual MUs. Maximal voluntary activation is reached when MU recruitment is complete and all recruited units are discharging at their maximal frequency. Thus, a submaximal discharge rate is thought to indicate sub-optimal activation (Herbert and Gandevia 1999).
Age-related changes in MU contractile properties have been studied by percutaneous nerve stimulation (Doherty and Brown 1997) and spike-triggered averaging methods (Galganski et al. 1993; Semmler et al. 2000). Increases in MU twitch torque (Galganski et al. 1993; Klass et al. 2005b) and in the amplitude of its action potential (Doherty and Brown 1993; Masakado et al. 1994) have been reported with ageing, supporting the concept of enhanced MU size due to the reinnervation phenomenon discussed previously. This remodelling is associated with a slowing of the MU contractile kinetics (Doherty and Brown 1997) and conduction velocity (Wang et al. 1999). Adjustments in the discharge pattern of MUs during maximal and submaximal contractions may help older adults adapt to these changes in MU structure and contractile properties (Chan et al. 2001; Roos et al. 1997). Accordingly, although studies have reported no difference in the minimum discharge frequency of single MUs at recruitment or at low torque levels between elderly and young adults (Galganski et al. 1993; Kamen et al. 1995), most studies have observed lower discharge frequencies at maximal or near-maximal contraction intensities in elderly adults (Connelly et al. 1999; Kamen et al. 1995). The major question is whether this decline in maximal discharge frequency in elderly subjects indicates a reduction in voluntary activation, as is the case for young subjects (Herbert and Gandevia 1999). In fact, due to the slowing of MUs contractile properties with ageing, elderly adults may achieve tetanic fusion at a lower discharge frequency compared with young adults. Thus, the decline in maximal discharge frequency observed in older adults may reflect a neural adaptation rather than an impairment of central drive to the motor neurones because higher discharge frequencies would not increase the torque developed by the muscle. The findings of Connelly et al. (1999) support the hypothesis that MU discharge patterns are adapted to changes in their contractile properties with advancing age. These authors observed that lower MU discharge frequencies matched the prolonged muscle twitch contraction time in elderly subjects, and the relatively higher MU discharge frequencies matched the shorter twitch contraction time in young adults. This observation has been confirmed by a recent investigation of MU behaviour in which prolonged MU contraction times were associated with lower maximal discharge rates in older adults (M. Klass et al., unpublished data).
Coactivation
Greater coactivation can reduce the performance of agonist muscles both through the opposing mechanical action of the antagonist muscles (Carolan and Cafarelli 1992), and also by reciprocal inhibition (Crone and Nielsen 1989). Nevertheless, a small level of coactivation is usually considered to be useful in the stabilization of the joint (Baratta et al. 1988). The magnitude of coactivation during MVCs is typically assessed by expressing EMG activity in the antagonist muscle as a percentage of its activity when acting as an agonist during a maximal contraction (Kellis 1998). Similar to the conflicting reports of changes in voluntary activation with ageing, the literature regarding alterations in coactivation is highly variable.
Some of the studies that have measured antagonist activity showed a higher level of coactivation during maximal isometric (Table 3; Izquierdo et al. 1999; Klein et al. 2001; Valkeinen et al. 2002) and concentric (Izquierdo et al. 1999) contractions in elderly compared with young adults (Table 4). In contrast, some authors did not observe any difference between age-groups during dynamic (Table 4; Klass et al. 2005a; Ochala et al. 2004; Pousson et al. 2001) or isometric (Table 3; Klass et al. 2005a; Morse et al. 2004; Pousson et al. 2001; Simoneau et al. 2005) contractions either for upper or lower limb muscles. As discussed by Macaluso et al. (2002), these contrasting results seem to be partly related to the muscle group investigated because increased coactivation was observed in elders during maximal knee extension, but not during knee flexion. Simoneau et al. (2005) have also reported conflicting results for the ankle plantar- and dorsi-flexor muscles. Interestingly, these authors reported lower coactivation in elderly compared with young subjects during maximal plantar flexion, and similar levels of coactivation during dorsiflexion. In both age-groups, the level of coactivation appeared to be positively related to the torque produced. Another factor that could explain part of the discrepancy between results is the contraction modality. Burnett et al. (2000) reported greater coactivation of intrinsic hand muscles during submaximal concentric and eccentric contractions in the elderly, with no corresponding differences in coactivation during isometric contractions. In contrast, comparable levels of coactivation were observed in elderly and young adults during maximal contraction of the ankle dorsiflexors, regardless of the contraction modality and velocity (Klass et al. 2005a).
Although possible that greater coactivation might contribute to reduced force production by some agonist muscles in older adults, small increases in coactivation do not appear to be correlated with a reduction in net joint torque (Klein et al. 2001; Valkeinen et al. 2002). This finding indicates that modest fluctuations in coactivation do not seem to have a large effect on the torque produced by agonist muscles, at least during MVC of an isolated muscle group. Additional studies are needed to fully understand the functional implications of increased coactivation of some muscle groups reported in elderly adults.
Conclusions
The primary conclusions of this review are:
-
Although there appear to be small differences in the sensitivity of various techniques used to assess voluntary activation, differences in the muscle group that is tested represent the main source of divergent findings regarding the ability of older adults to fully activate their muscles. Clearly, some muscles (ankle dorsiflexors) are more easily activated during MVC than others (quadriceps, biceps brachii). The latter muscle groups are often sub-maximally activated by the central nervous system even in young subjects. When an impaired ability to achieve maximal voluntary activation is present in healthy older adults, the extent of this impairment is only slightly greater than young adults. Therefore, the decline in maximal discharge frequency that has been observed with advancing age may reflect a neural adaptation to slowing of the MU contractile properties, rather than impaired central drive to the muscle. In contrast, a clear deficit in voluntary activation has been observed in elderly adults who are less physically active (Harridge et al. 1999) or affected by disease (Hurley and Newham 1993).
-
Despite similar experimental approaches, results comparing the coactivation of agonist and antagonist muscles in elderly and young subjects are as divergent as findings regarding voluntary activation. Coactivation appears to be higher in elderly adults during knee extension (Macaluso et al. 2002) and sometimes during elbow flexion (Klein et al. 2001). However, modest fluctuations in coactivation do not seem to have a large effect on voluntary activation or torque production by the agonist muscle during MVC.
In conclusion, the age-related decline in force results mainly from profound alterations within the muscle, whereas the contribution of voluntary activation deficits seem to be modest during MVC of a single muscle group in healthy and active elderly adults. However, further experiments are needed to investigate potential impairments in voluntary activation during multi-joint movements and very fast contractions.
References
Aagaard P, Simonsen EB, Andersen JL, Magnusson P, Dyhre-Poulsen P (2002) Increased rate of force development and neural drive of human skeletal muscle following resistance training. J Appl Physiol 93:1318–1326
Allen GM, McKenzie DK, Gandevia SC (1998) Twitch interpolation of the elbow flexor muscles at high forces. Muscle Nerve 21:318–328
Baratta R, Solomonow M, Zhou M, Letson D, D’Ambrosia R (1988) Muscular coactivation. The role of antagonist musculature in maintaining knee joint stability. Am J Sports Med 16:113–122
Baudry S, Klass M, Duchateau J (2005) Post-activation potentiation influences differently the nonlinear summation of contractions in young and elderly adults. J Appl Physiol 98:1243–1250
Behm DG, St-Pierre DMM, Perez D (1996) Muscle inactivation: assessment of interpolated twitch technique. J Appl Physiol 81:2267–2273
Behm D, Power K, Drinkwater E (2001) Comparison of interpolation and central activation ratios as measures of muscle inactivation. Muscle Nerve 24:925–934
Belanger AY, McComas AJ (1981) Extent of motor unit activation during effort. J Appl Physiol 51:1131–1135
Bigland-Ritchie B, Johansson R, Lippold OC, Woods JJ (1983) Contractile speed and EMG changes during fatigue of sustained maximal voluntary contractions. J Neurophysiol 50:313–324
Bilodeau M, Erb MD, Nichols JM, Joiner KL, Weeks J (2001) Fatigue of elbow flexor muscles in younger and older adults. Muscle Nerve 24:98–106
Burnett RA, Laidlaw DH, Enoka RM (2000) Coactivation of the antagonist muscle does not covary with steadiness in old adults. J Appl Physiol 89:61–71
Campbell MJ, McComas AJ, Petito F (1973) Physiological changes in ageing muscles. J Neurol Neurosurg Psychiatry 36:174–182
Carolan B, Cafarelli E (1992) Adaptations in coactivation after isometric resistance training. J Appl Physiol 73:911–917
Chan KM, Doherty TJ, Brown WF (2001) Contractile properties of human motor units in health, aging, and disease. Muscle Nerve 24:1113–1133
Connelly DM, Rice CL, Roos MR, Vandervoort AA (1999) Motor unit firing rate and contractile properties in tibialis anterior of young and old men. J Appl Physiol 87:843–852
Crone C, Nielsen J (1989) Spinal mechanisms in man contributing to reciprocal inhibition during voluntary dorsiflexion of the foot. J Physiol 416:255–272
D’Antona G, Pellegrino MA, Adami R, Rossi R, Carlizzi CN, Canepari M, Saltin B, Bottinelli R (2003) The effect of ageing and immobilization on structure and function of human skeletal muscle fibres. J Physiol 552:499–511
De Serres SJ, Enoka RM (1998) Older adults can maximally activate the biceps brachii muscle by voluntary command. J Appl Physiol 84:284–291
Doherty TJ, Brown WF (1993) The estimated numbers and relative sizes of thenar motor units as selected by multiple point stimulation in young and older adults. Muscle Nerve 16:355–366
Doherty TJ, Brown WF (1997) Age-related changes in the twitch contractile properties of human thenar motor units. J Appl Physiol 82:93–101
Eisen A, Siejka S, Schulzer M, Calne D (1991) Age-dependent decline in motor evoked potential (MEP) amplitude: with a comment on changes in Parkinson’s disease. Electroencephalogr Clin Neurophysiol 81:209–215
Esposito F, Malgrati D, Veicsteinas A, Orizio C (1996) Time and frequency domain analysis of electromyogram and sound myogram in the elderly. Eur J Appl Physiol 73:503–510
Farina D, Merletti R, Enoka R (2004) The extraction of neural strategies from the surface EMG. J Appl Physiol 96:1486–1495
Frontera WR, Hughes VA, Lutz KJ, Evans WJ (1991) A cross-sectional study of muscle strength and mass in 45- to 78-yr-old men and women. J Appl Physiol 71:644–650
Galganski ME, Fuglevand AJ, Enoka RM (1993) Reduced control of motor output in a human hand muscle of elderly subjects during submaximal contractions. J Neurophysiol 69:2108–2115
Hakkinen K, Alen M, Kallinen M, Izquierdo M, Jokelainen K, Lassila H, Mälkiä E, Kraemer WJ, Newton RU (1998) Muscle CSA, force production, and activation of leg extensors during isometric and dynamic actions in middle-aged and elderly men and women. J Aging Phys Act 6:232–247
Harridge SDR, White MJ (1993) A comparison of voluntary and electrically evoked isokinetic plantar flexor torque in males. Eur J Appl Physiol 66:343–348
Harridge SDR, Kryger A, Stensgaard A (1999) Knee extensor strength, activation, and size in very elderly people following strength training. Muscle Nerve 22:831–839
Herbert RD, Gandevia SC (1999) Twitch interpolation in human muscles: mechanisms and implications for measurement of voluntary activation. J Neurophysiol 82:2271–2283
Höök P, Sriramoju V, Larsson L (2001) Effects of aging on actin sliding speed on myosin from single skeletal muscle cells of mice, rats, and humans. Am J Physiol 280:C782–C788
Hunter SK, Thompson MW, Ruell PA, Harmer AR, Thom JM, Gwinn TH, Adams RD (1999) Human skeletal sarcoplasmic reticulum Ca²+ uptake and muscle function with aging and strength training. J Appl Physiol 86:1858–1865
Hurley MV, Newham DJ (1993) The influence of arthrogenous muscle inhibition on quadriceps rehabilitation of patients with early, unilateral osteoarthritic knees. Br J Rheumatol 32:127–131
Izquierdo M, Ibanez J, Gorostiaga E, Garrues M, Zuniga A, Anton A, Larrion JL, Hakkinen K (1999) Maximal strength and power characteristics in isometric and dynamic actions of the upper and lower extremities in middle-aged and older men. Acta Physiol Scand 167:57–68
Jakobi JM, Rice CL (2002) Voluntary muscle activation varies with age and muscle group. J Appl Physiol 93:457–462
Kamen G, Sison SV, Du CC, Patten C (1995) Motor unit discharge behavior in older adults during maximal-effort contractions. J Appl Physiol 79:1908–1913
Keenan KG, Farina D, Maluf KS, Merletti R, Enoka RM (2005) Influence of amplitude cancellation on the simulated surface electromyogram. J Appl Physiol 98:120–131
Kellis E (1998) Quantification of quadriceps and hamstring antagonist activity. Sports Med 25:37–62
Kent-Braun JA, Le Blanc R (1996) Quantitation of central activation failure during maximal voluntary contractions in humans. Muscle Nerve 19:861–869
Kent-Braun JA, Ng AV (1999) Specific strength and voluntary muscle activation in young and elderly women and men. J Appl Physiol 87:22–29
Kent-Braun JA, Ng AV, Doyle JW, Towse TF (2002) Human skeletal muscle responses vary with age and gender during fatigue due to incremental isometric exercise. J Appl Physiol 93:1813–1823
Klass M, Baudry S, Duchateau J (2005a) Aging does not affect voluntary activation of the ankle dorsiflexors during isometric, concentric, and eccentric contractions. J Appl Physiol 99:31–38
Klass M, Baudry S, Duchateau J (2005b) Contractile properties of single motor units in elderly. Comput Methods Biomech Biomed Engin (Suppl. 1):167–168
Klein CS, Rice CL, Marsh GD (2001) Normalized force, activation, and coactivation in the arm muscles of young and old men. J Appl Physiol 91:1341–1349
Lanza IR, Russ DW, Kent-Braun JA (2004) Age-related enhancement of fatigue resistance is evident in men during both isometric and dynamic tasks. J Appl Physiol 97:967–975
Lexell J (1993) Ageing and human muscle: observations from Sweden. Can J Appl Physiol 18:2–18
Macaluso A, De Vito G (2004) Muscle strength, power and adaptations to resistant training in older people. Eur J Appl Physiol 91:450–472
Macaluso A, Nimmo MA, Foster JE, Cockburn M, McMillan NC, De Vito G (2002) Contractile muscle volume and agonist-antagonist coactivation account for differences in torque between young and older women. Muscle Nerve 25:858–863
Masakado Y, Noda Y, Nagata MA, Kimura A, Chino N, Akaboshi K (1994) Macro-EMG and motor unit recruitment threshold: differences between the young and the aged. Neurosci Lett 179:1–4
McNeil CJ, Doherty TJ, Stashuk DW, Rice CL (2005) Motor unit number estimates in the tibialis anterior muscle of young, old, and very old men. Muscle Nerve 31:461–467
Merton PA (1954) Voluntary strength and muscle fatigue. J Physiol 123:553–564
Miller M, Downham D, Lexell J (1999) Superimposed single impulse and pulse train electrical stimulation: a quantitative assessment during submaximal isometric knee extension in young, healthy men. Muscle Nerve 22:1038–1046
Morse CI, Thom JM, Davis MG, Fox KR, Birch KM, Narici MV (2004) Reduced plantarflexor specific torque in the elderly is associated with a lower activation capacity. Eur J Appl Physiol 92:219–226
Morse CI, Thom JM, Birch KM, Narici MV (2005) Tendon elongation influences the amplitude of interpolated doublets in the assessment of activation in elderly men. J Appl Physiol 98:221–226
Narici MV, Maganaris CN (2006) Adaptability of elderly human muscles and tendons to increased loading. J Anat 208:433–443
Narici MV, Maganaris CN, Reeves N (2002) Muscle and tendon adaptations to ageing and spaceflight. J Gravit Physiol 9:137–138
Ochala J, Lambertz D, Pousson M, Goubel F, Van Hoecke J (2004) Changes in mechanical properties of human flexor muscles in ageing. Exp Gerontol 39:349–358
Payne AM, Delbono O (2004) Neurogenesis of excitation–contraction uncoupling in aging skeletal muscle. Exerc Sport Sci Rev 32:36–40
Philipps SK, Bruce SA, Newton D, Woledge RC (1992) The weakness of old age is not due to failure of muscle activation. J Gerontol 47A:M45–M49
Pitcher JB, Ogston KM, Miles TS (2003) Age and sex differences in human motor cortex input–output characteristics. J Physiol 546:605–613
Porter MM, Vandervoort AA, Kramer JF (1997) Eccentric peak torque of the plantar and dorsiflexors is maintained in older women. J Gerontol 52:B125–B131
Pousson M, Lepers R, Van Hoeck J (2001) Changes in isokinetic torque and muscular activity of elbow flexors muscles with age. Exp Gerontol 36:1687–1698
Roos MR, Rice CL, Vandervoort AA (1997) Age-related changes in motor unit function. Muscle Nerve 20:679–690
Roos MR, Rice CL, Connelly DM, Vandervoort AA (1999) Quadriceps muscle strength, contractile properties, and motor units firing rates in young and old men. Muscle Nerve 22:1094–1103
Semmler JG, Steege JW, Kornatz KW, Enoka RM (2000) Motor-unit synchronization is not responsible for lager motor-unit forces in old adults. J Neurophysiol 84:358–366
Simoneau E, Martin A, Van Hoecke J (2005) Muscular performances at the ankle joint in young and elderly men. J Gerontol 60A:439–447
Stackhouse SK, Stevens JE, Lee SCK, Pearce KM, Snyder-Mackler L, Binder-Macleod SA (2001) Maximum voluntary activation in nonfatigued and fatigued muscle of young and elderly individuals. Phys Ther 81:1102–1109
Stevens JE, Binder-Masleod S, Snyder-Mackler L (2001) Characterization of the human quadriceps muscle in active elders. Arch Phys Med Rehabil 82:973–978
Stevens JE, Stackhouse SK, Binder-Macleod SA, Snyder-Mackler L (2003) Are voluntary muscle activation deficits in older adults meaningful? Muscle Nerve 27:99–101
Thomas DO, White MJ, Sagar G, Davies CT (1987) Electrically evoked isokinetic plantar flexor torque in males. J Appl Physiol 63:1499–1503
Valkeinen H, Ylinen J, Malkia E, Alen M, Hakkinen K (2002) Maximal force, force/time and activation/coactivation characteristics of the neck muscles in extension and flexion in healthy men and women at different ages. Eur J Appl Physiol 88:247–254
Van Cutsem M, Duchateau J (2005) Preceding muscle activity influences motor unit discharge and rate of torque development during ballistic contractions in humans. J Physiol 15:635–644
Vandervoort AA, McComas AJ (1986) Contractile changes in opposing muscles of the human ankle joint with aging. J Appl Physiol 61:361–367
Vandervoort AA, Kramer JF, Wharram ER (1990) Eccentric knee strength of elderly females. J Gerontol 45:B125–B128
Wang F-C, De Pasqua V, Delwaide PJ (1999) Age-related changes in fastest and slowest conducting axons of thenar motor units. Muscle Nerve 22:1022–1029
White MJ, Harridge SDR (1990) At high angular velocities voluntary activation limits maximal isokinetic torque generation in elderly and young human triceps surae. J Physiol 429:52P
Winegard KJ, Hicks AL, Vandervoort AA (1997) An evaluation of the length–tension relationship in elderly human plantarflexor muscles. J Gerontol A Biol Sci Med Sci 52:B337–B343
Yue GH, Ranganathan VK, Siemionov V, Liu JZ, Sahgal V (1999) Older adults exhibit a reduced ability to fully activate their biceps brachii muscle. J Gerontol 54A:249–253
Acknowledgments
The authors are particularly grateful to Dr K. Maluf for useful comments on the paper and to A. Desseir for assistance in the preparation of the manuscript. Some experiments described in this review were performed with support from a grant of the European Community (contract QLK6-CT-2001-00323) and the Fonds National de la Recherche Scientifique of Belgium.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Klass, M., Baudry, S. & Duchateau, J. Voluntary activation during maximal contraction with advancing age: a brief review. Eur J Appl Physiol 100, 543–551 (2007). https://doi.org/10.1007/s00421-006-0205-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-006-0205-x