
Abstract
Based on studies using maximal isometric contractions, it is suggested that fatigue may be elicited due to hyperthermia-induced impairments in central neuromuscular activation. We investigated the effects of passive hyperthermia on isokinetic maximal force production. Twenty young healthy males [peak oxygen uptake 52.9 (6.8) ml kg−1 min−1, body fat 11 (5)%] were passively warmed in a hot (42°C) water bath to rectal temperature (T re) of 39.5°C and then cooled back to 38.0°C. At 0.5°C intervals, they performed two maximal voluntary knee extensions each at 60, 120, and 240 s−1. Peak torques at 37.5°C were 168 (34), 145 (29), and 112 (17) N m for 60, 120, and 240 s−1 contraction speeds, respectively, and 166 (38), 150 (31), and 119 (17) N m at T re of 39.5°C. No significant differences in peak torque at any of the three contraction speeds were observed over the range 37.5–39.5°C. Skin cooling, even with a warm core of 39.5°C, immediately decreased peak torque [159 (42), 133 (34), 107 (22) N m at 60, 120, and 240 s−1, respectively). We conclude that lowered skin temperature can impair isokinetic force production independent of core temperature.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Hyperthermia, or elevated body temperature, may arise through a combination of endogenous heat generated through exercise and/or exogenous heat through exposure to hot environments. Hyperthermia increases the physiological strain on the body, and recent research has demonstrated a consistent core temperature at the point of voluntary fatigue during whole-body exercise in animals (Walters et al. 2000) and both fit (Gonzalez-Alonso et al. 1999) and non-fit (Cheung and McLellan 1998) humans, leading to the proposal of elevated central temperatures per se as a mechanism for eliciting fatigue (Nielsen and Nybo 2003). One potential contributor to hyperthermia-induced fatigue may be an impaired central neuromuscular activation, based on decreased maximal isometric voluntary contractions of both exercised (leg) and non-exercised (hand) muscles at esophageal temperatures of ~40°C following exercise-induced hyperthermia in a hot environment (Nybo and Nielsen 2001a) and also a gradual reduction in motor unit activation with passive hyperthermia (Morrison et al. 2004). The idea of decreased central activation at hyperthermic fatigue is further supported by evidence of decreased mental arousal (Nielsen et al. 2001) along with decreased cerebral blood flow (Nybo and Nielsen 2001b) during hyperthermia.
Recent work on isolating the mechanisms of hyperthermia-induced fatigue has focused on peak torque and motor unit activation during brief or sustained maximal isometric contractions (Morrison et al. 2004; Nybo and Nielsen 2001a). However, the effect of core and skin temperature on dynamic muscle contractions and different speeds of contraction remain less explored. With brief bursts of high intensity exercise, elevated muscle temperature appear to result in increases in both peak and mean power outputs during cycling sprints in both free-cadence (Ball et al. 1999; Falk et al. 1998) and isokinetic cycling modes (Sargeant 1987), while cooling of the musculature results in impaired high intensity performance (Comeau et al. 2003; Sleivert et al. 2001). The potentiation in power with muscle warming is greater at higher isokinetic pedaling cadences (Sargeant 1987) suggesting a velocity dependence with muscle warming. This is supported by higher power outputs during cycling sprinting following 30 min passive exposure to a warm (30°C) environment due to a higher pedaling cadence (Ball et al. 1999).
The relative contribution of elevations in core versus skin temperatures on isokinetic force production and hyperthermia-induced fatigue remains unclear. Force production may be impaired by changes in local arm muscle temperature without any concomitant changes in core temperature (Giesbrecht et al. 1995), and may explain why individuals suddenly exposed to cold environments, such as shipwreck survivors, are unable to perform survival tasks and greatly increase their risk of drowning and death well before the onset of core temperature cooling and hypothermia (Giesbrecht 2000). The use of active exercise in a hot environment in most protocols to elicit hyperthermia raises skin temperature at the same time, making it difficult to control one variable while manipulating the other. Convertino et al. (1980) attempted to isolate the effects of exercise and thermal factors on the hypervolemic response by matching heat stress from exercise and passive heating, and the latter method, when combined with the use of a cooling garment to alter skin temperature, may present a better modality for understanding any direct effect of hyperthermia on neuromuscular function.
The purpose of the present study was to investigate the effects of passive hyperthermia and also to isolate the effects of core versus skin temperature on force production with isokinetic maximal voluntary contractions of the quadriceps. At 0.5°C core temperature intervals during heating from 37.5 to 39.5°C and then during cooling from 39.5°C back down to 38.0°C, subjects performed maximal knee extensions at three contractions speeds on an isokinetic dynamometer. We hypothesized the following: (1) that peak torques at the highest core temperatures would be lower than at cooler temperatures, and (2) that peak torques would be lower with cool skin than with warm skin.
Methods
Subjects
Twenty healthy male subjects between the ages of 18 and 34 years [74.7 (9.0) kg, 52.9 (6.8) ml kg−1 min−1 peak oxygen uptake (V̇O2peak), 11 (5)% body fat; mean (SD)] were recruited from the university population. Subjects were screened using the Physical Activity Readiness Questionnaire developed by the Canadian Society for Exercise Physiology (2002). They were then informed of all the experimental procedures and the associated risks and discomforts before providing written consent for their participation. The Health Sciences Research Ethics Board of Dalhousie University approved the experimental protocol and instrumentation used in the present study.
Research design
An initial control condition consisting of six sets of isokinetic maximal knee extensions over 1 h was included to account for changes in performance due to learning, boredom, or fatigue from repeated exercise. Passive heating was employed to minimize the possible confounding effects of exercise in comparing heating and cooling phases. Both heating and subsequent cooling back to baseline were employed to isolate the effects of central core temperature versus skin temperature (i.e., same core temperatures but hot skin during heating phase versus cool skin during cooling phase) on force production.
Control protocol
In session 1, basic anthropometric measures were obtained, consisting of height, body mass, and body fatness estimation using skinfold measurements and calculated using the Jackson and Pollack method (1978). Subjects then performed a graded maximal exercise test on a cycle ergometer (Monark 818, Sweden) beginning at 60 W and increasing at 30 W each minute until exhaustion for the determination of V̇O2peak from measurement of expired gases (Aerosport VO2000, Aerosport, Ann Arbour, Mich.).
Following aerobic testing, subjects rested for 30 min and then performed a session on the isokinetic dynamometer (Kin-Com, Chattanooga Group, Hixson, Tenn.) to familiarize themselves with performing isokinetic contractions and also to determine the possible effects of boredom or fatigue on performance. At 15 min intervals, subjects performed two maximal voluntary contractions (MVCs) consisting of knee extensions of the right leg at speeds of 60, 120, and 240 s−1. The order of presentation of the speeds was always 120 s−1 first, followed by 60 or 240 s−1 in a counter-balanced pattern. Recovery time was approximately 10 s between MVCs at each speed and 1 min between speeds.
Experimental protocol
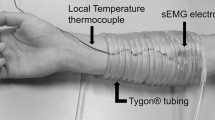
The experimental trial consisted of one single session where subjects performed maximal isokinetic contractions while first being passively heated from resting temperature of 37.5°C up to 39.5°C and then passively cooled back to 38.0°C. Upon arrival at the laboratory, subjects changed into a bathing suit and inserted the rectal thermocouple (Mon-A-Therm Core, Mallinkrodt Medical, St. Louis, Mo.) 15 cm beyond the anal sphincter for measurement of rectal temperature (T re). T re is a valid and reliable index of body heat storage during hyperthermia that tracks ~0.3–0.4°C below esophageal temperature (Moran and Mendal 2002), which in turn tracks ~0.2°C below predicted brain temperature (Nybo et al. 2002). They were then instrumented for heart rate (Polar Vantage XL, Polar Electro Oy, Finland) and skin temperature (T sk: Mon-A-Therm Skin, Mallinkrodt Medical) at four sites (chest, upper arm, thigh, calf) for calculation of mean skin temperature (T̄ sk) (Ramanathan 1964). Mean body temperature (T̄ body) was calculated using a core and T sk weighting value of T̄ body=0.65(T re)+0.35(T̄ sk%) (Ramanathan 1964). T re and T sk were recorded every 30 s on an IBM-compatible laptop using a customized data acquisition system software written with Labview (Labview 5.1, National Instruments, Austin, Tex.) software.
Following instrumentation, subjects performed two MVCs at speeds of 60, 120, and 240 s−1. Recovery time was approximately 10 s between MVCs at each speed and 1 min between speeds. The order of presentation of the speeds was always 120 s−1, followed by 60 or 240 s−1 in a counter-balanced pattern. Subjects were then immersed to the neck in a hot (42°C) water bath and warmed passively. At 37.5, 38.0, 38.5, 39.0, and 39.5°C T re, subjects were removed from the tub and performed the isokinetic test battery. Heart rate (HR), blood pressure, and subjective thermal sensation using a 21-point thermal comfort vote (TCV) scale ranging from +10 being unbearably hot, 0 being neutral, and −10 being unbearably cold (Mekjavic et al. 1994) were recorded once the subjects were seated on the Kin-Com device. Total out-of-water time for each test battery was approximately 5 min. Upon finishing the test battery at 39.5°C or upon voluntary exhaustion, subjects were dressed in a liquid conditioning garment (LCG) (Core-Tech Tubesuit, Delta-Temax, Pembroke, Canada) consisting of 3.2 mm diameter Tygon tubing closely sewn over a tightly fitting hood, pants, and shirt covering the torso and arms. The face, hands, and feet were left uncovered. Cold (8°C) fluid was circulated through the suit at approximately 1 l min−1, and subjects were cooled until T re returned to 38.0°C, performing the isokinetic test battery at 39.5, 39.0, 38.5, and 38.0°C.
Hydration
Subjects were encouraged to drink a carbohydrate–electrolyte drink (Gatorade) throughout the heating and cooling protocol. Body weight was measured at each testing point using a digital strain gauge scale (HL120, Avery Berkel, LaPorte, Ind.), and subjects were requested to consume an amount of fluid equal to any weight lost during that interval.
Data analysis
Peak torque (newton meters) for the MVC at each contraction speed was recorded on the Kin-Com, and the higher of the two values were plotted at each time point for the control session and temperature point for the testing session. Peak torque was compared during the heating phase (T re from 37.5°C up to 39.5°C) and cooling phase (T re from 39.5°C down to 38.0°C) using a three-factor (phase × temperature × speed) repeated measures analysis of variance (ANOVA) with Bonferroni adjustment for multiple comparisons. Statistical significance was set at P<0.05 unless otherwise stated.
Results
Temperature
The heating and cooling protocol was able to successfully elevate core body temperature from normothermic resting values up to 39.5°C and then return subjects to 38.0°C, with the total experimental session, including isokinetic testing, requiring 183 (38) min. Fluid consumption was ~1.5 l over the ~90 min of the heating phase. The hydration protocol was able to maintain euhydration in subjects throughout both the heating and cooling phases. Body mass was 76.7 (8.8) kg at the start of the experimental session at T re=37.5°C, and was similar at 77.0 (8.8) kg upon completion of the heating phase at T re=39.5°C.
Three subjects reached 39.0°C T re but were unable to voluntarily reach the initial target of 39.5°C. These subjects were however able to perform the cooling phase back down to 38.0°C. These three have been included in the mean data, but have been dropped (listwise comparison) in the ANOVA analyses, which include the highest core temperature (39.5°C). All subjects reported being at or very near the point of hyperthermia-induced exhaustion, supported by near-maximal subjective scores on the TCV at the end of the heating phase (Fig. 1). The T sk and TCV gradually increased over the course of the heating phase, from 32.5 (1.9)°C and 1 (1), respectively, at the starting T re of 37.5°C, to 35.6 (1.5)°C and 8 (2), respectively, at the final heating T re of 39.5°C (Fig. 1). Immediately upon donning of the LCG and the initiation of the cooling phase, T sk and TCV rapidly decreased to 31.8 (1.9)°C and −2 (2) while T re remained at 39.5°C. T̄ sk and TCV then gradually decreased to 27.6 (1.8)°C and −6 (2) when T re dropped to 38.0°C.

Mean skin temperature (T̄ sk ■), mean body temperature (T̄ body ▲), and subjective thermal comfort vote (TCV ○) during passive heating from rectal temperature 37.5°C to 39.5°C and then passive cooling from 39.5°C to 38.0°C. Values are given in means (SD). Matching letters indicate significant differences for T̄ sk, T̄ body, and TCV (P<0.001)
The passive immersion and warming of the skin resulted in an elevation in HR from an initial value of 83 (20) beats min−1 at T re of 37.5°C to 125 (17) beats min−1 at 39.5°C (P<0.001) (Fig. 2). Mean arterial pressure (MAP) also decreased significantly from initial values of 86 (8) mmHg to 68 (6) mmHg at 39.5°C T re (P<0.001) (Fig. 2). Immediately upon cooling, MAP returned to near initial values [89 (6) mmHg], remaining at a plateau for the remainder of the cooling phase. HR also decreased back to initial values immediately upon the initiation of cooling, dropping to 85 (16) beats min−1 at the start of cooling (T re=39.5°C, P<0.001) and remaining stable for the remainder of the cooling phase.

Heart rate (●) and mean arterial pressure (MAP Δ) response during passive heating from rectal temperature 37.5°C to 39.5°C and then passive cooling from 39.5°C to 38.0°C. Values are given in means (SD). Matching letters indicate significant differences for heart rate and MAP (P<0.001)
Isokinetic strength
During the control session consisting of six sets of isokinetic maximal voluntary knee extensions over 1 h (data not shown), peak torques were inversely related to the contraction speed, with significant differences (P<0.001) in peak torques between 60, 120, and 240 s−1 contraction speeds. No differences were observed in peak torques over the course of the six control tests at any of the contraction speeds.
Peak torques at 60, 120, and 240 s−1 contraction speeds did not change over the heating phase from T re 37.5–39.5°C (P=0.47, Fig. 3). Peak torque at 60 s−1 was 167 (34) N m at 37.5°C and 166 (38) N m at 39.5°C. Peak torque was again inversely related to contraction speed, with significantly lower peak torque values at the 120 and 240 s−1 speeds (P<0.001). Peak torque at 240 s−1 was 111 (17) N m at 37.5°C and 119 (17) N m at 39.5°C. Immediately upon skin cooling and with T re remaining elevated at 39.5°C, peak torque at all contraction speeds decreased significantly, with peak torque at 60 and 240 s−1 speeds of 159 (42) and 107 (22) N m respectively (P<0.001). Peak torques during the rest of the whole-body cooling phase remained stable and lower than those observed during whole-body heating, with the same pattern of higher peak torques with lower contraction speeds.

Peak torques generated with maximal 60 (■), 120 (○), and 240 (▲) s−1 isokinetic knee extensions during passive heating from rectal temperature 37.5°C to 39.5°C and then passive cooling from 39.5°C to 38.0°C. Values are given in means (SD). No significant changes in peak torque were observed at any of the contractions speeds during the heating phase (37.5–39.5°C) or the cooling phase (39.5–38.0°C) separately. a A significant main effect of heating versus cooling phases on peak torque. b A significant main effect of contraction speed on peak torque across all temperature conditions (P<0.001)
Discussion
The primary finding of the present study was that passive heating from 37.5°C up to 39.5°C T re did not significantly impair torque outputs during isokinetic maximal voluntary knee extensions at three different contraction speeds. This is in contrast to other reports that isokinetic strength or dynamic force output were increased with heat exposure or local muscle heating (Ball et al. 1999; Falk et al. 1998; Sargeant 1987). In addition, we observed that decreases in local T sk during the cooling phase, despite an elevated core temperature, elicited a lower peak torque at all contraction speeds and core temperatures than the peak torques generated at the equivalent core temperature during the heating phase (warm skin).
By performing passive heating over the course of a single exposure while maintaining euhydration, we were able to provide a profile of isokinetic strength over the course of heat exposure from normothermia to very high levels of hyperthermia near or at the point of voluntary exhaustion previously reported for prolonged submaximal exercise (Gonzalez-Alonso et al. 1999). Our observations of no potentiation of peak isokinetic torque over the course of whole-body hyperthermia supports a previous report of no potentiation with local leg heating (Stanley et al. 1994). This differs from other reports of enhancement with heat exposure (Ball et al. 1999; Falk et al. 1998; Sargeant 1987), possibly due to the different protocols employed. These protocols employed a single and relatively brief hot air exposure or partial water immersion at different temperatures to warm up the body. However, core temperatures were either not recorded (Ball et al. 1999; Sargeant 1987) or else the heat exposure resulted in minimal changes in body temperature (Falk et al. 1998), making the level of thermal strain either unknown or likely much lower than with the present protocol. Other studies using exercise-induced hyperthermia have also not accounted for the effects of dehydration or exercise-induced fatigue (Ftaiti et al. 2001).
The effects of hyperthermia on force production may be dependent on the mode of exercise. Major decrements in force production were reported with sustained isometric contraction of both leg and arm muscles following high levels of exercise-induced hyperthermia (Nybo and Nielsen 2001a) and also in the legs following passive hyperthermia (Morrison et al. 2004). However, an alternate explanation is that hyperthermia may only attenuate the ability to sustain maximal muscle activation rather than the ability to mobilize maximal muscle force for a short period of time (Thornley et al. 2003), as the maximal duration of the isokinetic contractions (2–3 s for 60 s−1) is much shorter than the typical use of 10–30 s isometric contractions. Ftaiti et al. (2001) found that exercise-induced hyperthermia resulted in decrements in isometric knee extension and at isokinetic speeds of 60 s−1 but not at the faster isokinetic speed of 240 s−1. They also reported less electromyographic activity at these speeds and suggested activation deficits were specific to isometric or low velocity isokinetic contractions. We observed neither a potentiation of isokinetic peak torque with mild hyperthermia nor the sudden decrease in isometric peak force observed at high (39.5–40°C) core temperatures. This is in contrast to recent research suggesting a critical internal temperature at which fatigue is elicited through changes in cerebral activity or central neuromuscular activation (Nielsen et al. 2001; Nybo and Nielsen 2001a). The exercise protocol of Ftaiti et al. (2001) also elicited high levels of cardiovascular and physiological exhaustion, and this physiological strain may have contributed to the difference in impairment with hyperthermia at slow isokinetic speeds between their study and the present one.
While core temperature had no impact on isokinetic strength, a rapid decrease in skin temperature with the initiation of cooling significantly decreased peak torque throughout the entire cooling phase, despite elevated core temperatures, suggesting a significant contribution of local skin temperature on isokinetic strength. Handgrip strength decreased significantly with only brief (2 min) immersion of the hand or forearm in cold (5°C) water (Vincent and Tipton 1988), while impairments in manual dexterity and grip strength were primarily driven by local arm temperature rather than core temperatures (Giesbrecht et al. 1995). The second isokinetic test at 39.5°C T re occurred approximately 10–15 min after the initial test at 39.5°C, coming after the donning of the cooling garment and the peaking of T re following immersion. The rapid and significant drop in skin temperature upon the initiation of cooling suggests that changes in muscle temperature were likely to be negligible. In addition, over the course of the cooling phase, our use of a cooling garment likely decreased skin temperature without significant muscular effects, as direct ice-pack application for 30 min resulted in no changes in thigh muscle temperature below 2 cm (Enwemeka et al. 2002). The decrease in peak torque with skin cooling supports the decrease reported in isokinetic peak torque following 40 min of passive exposure to 10°C and 5°C air (Comeau et al. 2003) and also the decrease in peak force observed following leg immersion in cold water (Sargeant 1987). Overall, the present results support the idea that muscle function and force production may be rapidly impaired by skin cooling even with an elevated core temperature, emphasizing the importance of thermal protection of both the core and the peripheries during both sudden and sustained exposure to cold environments.
In conclusion, no effects on the peak torque generated during isokinetic maximal voluntary knee extensions were observed during passive elevation of core body temperature from normothermia to 39.5°C, suggesting that whole-body hyperthermia both does not facilitate high-intensity exercise and also that no critical central body temperature threshold for impairment of isokinetic force production exists over the range of core temperature tested. However, local skin cooling rapidly decreased peak torque compared to equivalent core temperatures, suggesting a strong role of skin temperature in force production and supporting observations of rapid impairment of muscular function upon exposure to cold environments. Future research should focus upon isolating the respective roles of central versus peripheral temperatures on force production during dynamic exercise and also on clarifying the mechanisms and linkages between thermal manipulations, cerebral responses, and neuromuscular function.
References
Ball D, Burrows C, Sargeant AJ (1999) Human power output during repeated sprint cycle exercise: the influence of thermal stress. Eur J Appl Physiol 79:360–366
Cheung SS, McLellan TM (1998) Influence of heat acclimation, aerobic fitness, and hydration effects on tolerance during uncompensable heat stress. J Appl Physiol 84:1731–1739
Comeau MJ, Potteiger JA, Brown LE (2003) Effects of environmental cooling on force production in the quadriceps and hamstrings. J Strength Cond Res 17:279–284
Convertino VA, Greenleaf JE, Bernauer EM (1980) Role of thermal and exercise factors in the mechanism of hypervolemia. J Appl Physiol 48:657–664
Canadian Society for Exercise Physiology (2002) Physical Activity Readiness Questionnaire. Ottawa, Canada
Enwemeka CS, Allen C, Avila P, Bina J, Konrade J, Munns S (2002) Soft tissue thermodynamics before, during, and after cold pack therapy. Med Sci Sports Exerc 34:45–50
Falk B, Radom-Isaac S, Hoffmann JR, Wang Y, Yarom Y, Magazanik A, Weinstein Y (1998) The effect of heat exposure on performance of and recovery from high- intensity, intermittent exercise. Int J Sports Med 19:1–6
Ftaiti F, Grelot L, Coudreuse JM, Nicol C (2001) Combined effect of heat stress, dehydration and exercise on neuromuscular function in humans. Eur J Appl Physiol 84:87–94
Giesbrecht GG (2000) Cold stress, near drowning and accidental hypothermia: a review. Aviat Space Environ Med 71:733–752
Giesbrecht GG, Wu MP, White MD, Johnston CE, Bristow GK (1995) Isolated effects of peripheral arm and central body cooling on arm performance. Aviat Space Environ Med 66:968–975
Gonzalez-Alonso J, Teller C, Andersen SL, Jensen FB, Hyldig T, Nielsen B (1999) Influence of body temperature on the development of fatigue during prolonged exercise in the heat. J Appl Physiol 86:1032–1039
Jackson AS, Pollack ML (1978) Generalized equations for predicting body density of men. Br J Nutr 40:497–504
Mekjavic IB, Passias T, Sundberg CJ, Eiken O (1994) Perception of thermal comfort during narcosis. Undersea Hyperb Med 21:9–19
Moran DS, Mendal L (2002) Core temperature measurement: methods and current insights. Sports Med 32:879–885
Morrison SA, Sleivert GG, Cheung SS (2004) Passive hyperthermia reduces voluntary activation and isometric force production. DOI 10.1007/s00421-004-1063-z
Nielsen B, Nybo L (2003) Cerebral changes during exercise in the heat. Sports Med 33:1–11
Nielsen B, Hyldig T, Bidstrup F, Gonzalez-Alonso J, Christoffersen GR (2001) Brain activity and fatigue during prolonged exercise in the heat. Pflugers Arch 442:41–48
Nybo L, Nielsen B (2001a) Hyperthermia and central fatigue during prolonged exercise in humans. J Appl Physiol 91:1055–1060
Nybo L, Nielsen B (2001b) Middle cerebral artery blood velocity is reduced with hyperthermia during prolonged exercise in humans. J Physiol (Lond) 534:279–286
Nybo L, Secher NH, Nielsen B (2002) Inadequate heat release from the human brain during prolonged exercise with hyperthermia. J Physiol (Lond) 545:697–704
Ramanathan NL (1964) A new weighting system for mean surface temperature of the human body. J Appl Physiol 19:531–533
Sargeant AJ (1987) Effect of muscle temperature on leg extension force and short-term power output in humans. Eur J Appl Physiol 56:693–698
Sleivert GG, Cotter JD, Roberts WS, Febbraio MA (2001) The influence of whole-body vs torso pre-cooling on physiological strain and performance of high-intensity exercise in the heat. Comp Biochem Physiol A Mol Integr Physiol 128:657–666
Stanley DC, Kraemer WJ, Howard RL, Armstrong LE, Maresh CM (1994) The effects of hot water immersion on muscle strength. J Strength Cond Res 8:134–138
Thornley LJ, Maxwell NS, Cheung SS (2003) Local tissue temperature effects on peak torque and muscular endurance during isometric knee extension. Eur J Appl Physiol 90:588–594
Vincent MJ, Tipton MJ (1988) The effects of cold immersion and hand protection on grip strength. Aviat Space Environ Med 59:738–741
Walters TJ, Ryan KL, Tate LM, Mason PA (2000) Exercise in the heat is limited by a critical internal temperature. J Appl Physiol 89:799–806
Acknowledgements
The authors wish to express their gratitude to the subjects who participated in the experiments. Technical assistance throughout this study was provided by L.J. Thornley. The infrastructure was supported by Canada Foundation for Innovation (New Opportunities), and the project was supported by a Discovery Grant (S. Cheung and G. Sleivert) from the Natural Sciences and Engineering Research Council.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Cheung, S.S., Sleivert, G.G. Lowering of skin temperature decreases isokinetic maximal force production independent of core temperature. Eur J Appl Physiol 91, 723–728 (2004). https://doi.org/10.1007/s00421-004-1062-0
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-004-1062-0