
Abstract
Previous studies have reported a decrease in muscle torque per cross-sectional area in old age. This investigation aimed at determining the influence of agonists muscle activation and antagonists co-activation on the specific torque of the plantarflexors (PF) in recreationally active elderly males (EM) and, for comparison, in young men (YM). Twenty-one EM, aged 70–82 years, and 14 YM, aged 19–35 years, performed isometric maximum voluntary contractions (MVC). Activation was assessed by comparing the amplitude of interpolated supramaximal twitch doublets at MVC, with post-tetanic doublet peak torque. Co-activation of the tibialis anterior (TA) was evaluated as the ratio of TA-integrated EMG (IEMG) activity during PF MVC compared to TA IEMG during maximal voluntary dorsiflexion. Triceps surae muscle volume (VOL) was assessed using magnetic resonance imaging (MRI), and PF peak torque was normalised to VOL (PT/VOL) since the later approximates physiological cross-sectional area (CSA) more closely than anatomical CSA. Also, physical activity level, assessed by accelerometry, was significantly lower (21%) in the elderly males. In comparison to the YM group, a greater difference in PT (39%) than VOL (19%) was found in the EM group. PT/VOL and activation capacity were respectively lower by 25% and 21% in EM compared to YM, whereas co-activation was not significantly different. In EM PT/VOL correlated with activation (R 2=0.31, P<0.01). In conclusion, a reduction in activation capacity may contribute significantly to the decline in specific torque in the plantar flexors of elderly males. The hypothesis is put forward that reduced physical activity is partialy responsible for the reduced activation capacity in the elderly.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
A decline in muscle mass and strength with age starts at about the 5th decade of life (Lindle et al. 1997). Although largely attributed to a decline in muscle mass, the decrease in strength occurs at a faster rate than the loss of muscle mass. Several investigators have attributed this phenomenon to changes in muscle quality of the elderly (Bruce et al. 1989; Jubrias et al. 1997; Klein et al. 2001; Macaluso et al. 2002; Vandervoort and McComas 1986; Young et al. 1985). The factors associated with this disproportionate loss of muscle strength compared to that of muscle size, include reduced agonist activation (Yue et al. 1999), increased antagonist co-activation (Klein et al. 2001), a decrease in fibre-specific tension (Frontera et al. 2000), alterations in muscle architecture (Kubo et al. 2003; Narici 2003) and increased proportion of non-contractile material (Kent-Braun et al. 2000).
Although alterations in muscle quality have been frequently reported in muscles of elderly individuals (Bruce et al. 1989; Jubrias et al. 1997; Klein et al. 2001; Macaluso et al. 2002; Vandervoort and McComas 1986; Young et al. 1985), the presence of an activation deficit in elderly muscle remains controversial. Indeed, whereas some authors reported a reduced activation capacity (Scaglioni et al. 2002; Stevens et al. 2001; Yue et al. 1999), others found complete activation in elderly individuals (Connelly et al. 1999; Klein et al. 2001; Roos et al. 1999; Vandervoort and McComas 1986). Although activation failure seems to be present in elderly muscle when superimposed electrically stimulated twitch trains were used (Stevens et al. 2001; Yue et al. 1999), complete activation has been found when single-twitch and double-twitch interpolation were used (Connelly et al. 1999; Klein et al. 2001; Roos et al. 1999; Vandervoort and McComas 1986). Interestingly, even in young subjects the use of single twitches has been shown to overestimate activation capacity when compared to twitch trains (Behm et al. 2001; Kent-Braun and Le Blanc 1996).
Despite the fact that both normalised strength and activation are reduced in the same muscle groups with ageing (albeit in separate studies), neither have been shown to be reduced in the same subjects nor have they been shown to be associated in the elderly. Additionally, although no link has been previously reported between activation and specific torque, co-activation has been shown to be increased in elderly subjects in the presence of a reduced specific torque (Klein et al. 2001; Macaluso et al. 2002). Hence, the aim of the present investigation was to determine whether the reduction in specific torque in the elderly is associated with a reduced agonist activation and/or an increased antagonist co-activation. Although torque is typically normalised for cross-sectional area (CSA), it has recently been shown that volume approximates physiological CSA more closely than anatomical CSA (Fukunaga et al. 2001); hence in this study maximum isometric torque (Nm) was normalised for muscle volume (m3) to yield specific torque expressed in kN m−2. Considering that physical activity is a modulator of neural activation (Duchateau and Enoka 2002), we hypothesised that elderly males would have reduced PF activation and that this would contribute towards a reduced specific torque in voluntary contractions. In addition a decrease in specific torque may also arise from an increased antagonist coactivation.
Methods
Subjects
Fourteen healthy young men [YM; age: 24.7 (4.7) years (range 19–35 years); height: 179.3 (7.8) cm; mass: 76.9 (12.4) kg; mean (SD)] and 21 healthy elderly men [EM; age: 73.7 (3.6) years (range 70–82 years); height: 170.4 (4.5) cm; mass: 77.5 (8.1) kg] volunteered to participate in this study. Elderly subjects were all medically screened prior to inclusion to exclude known cardiovascular, myopathic, neurological, neoplastic, inflammatory diseases, and the subjects were all community dwelling and lived independently. Both young and elderly individuals were physically active, but not engaged in sports at a competitive level. All procedures were approved by the Ethics Committee of Manchester Metropolitan University, and prior informed consent was obtained from each subject. Subjects were familiarised with all proceedings on a separate session prior to data collection.
Strength measurements
Isometric plantarflexion (PF) peak torque (PT) was recorded with the subjects laying prone, the left foot attached to the foot adapter of an isokinetic dynamometer (Cybex Norm; Cybex International, N.Y., USA), and strapped securely about the hip to prevent forward displacement of the body during maximal plantarflexions. Subjects were positioned with the knee in full extension and the lateral malleoli aligned with the axis of rotation identified on the dynamometer. The foot was tightly secured to the footplate to minimise heel displacement, and the subjects performed three submaximal isokinetic plantar and dorsiflexion contractions as a warm up. Two isometric maximal voluntary plantarflexion contractions (MVC) were performed at −20° dorsiflexion interspersed with at least 1 min restperiods. Maximal dorsiflexion was performed after PF MVC at −20° to obtain maximal DF EMG data for calculation of co-activation in the tibialis anterior (TA).
Twitch interpolation
To evaluate the ability of subjects to fully activate the plantarflexors during static contractions three supramaximal doublets were applied percutaneously (DSV Digitimer Stimulator; Digitimer, Herts., UK) using rubber stimulation pads (76 mm×127 mm, and 38 mm ×89 mm; Versastim; Conmed, N.Y., USA). The anode was placed distal to the popliteal crease and the cathode over the distal myotendinous junction of the soleus.
The supramaximal doublet amplitude was determined prior to interpolation by administering twitches of progressively increasing current intensity. Twitches were administered with the subjects in a relaxed state starting from 100 mA, and increasing by 50- to 1000-mA increments until no further increase in twitch force was observed with a further 50-mA increase in stimulation strength. Three doublets (pulse width of 50 μs, interpulse interval 10 ms) were applied to assess activation capacity, the first two doublets were applied during MVC and a further doublet applied on relaxation, each separated by 1.5 s. The first doublet was delivered manually during the plateau phase of the second MVC attempt and the subjects were encouraged to continue contracting maximally until the second doublet was delivered.
A ratio of interpolated and post-tetanic doublets was used to provide an index of activation, the interpolated doublet on the highest contractile force was used in the calculation of activation level (Allen et al. 1995; Harridge et al. 1999; Klein et al. 2001) as follows: percentage activation=[1−(superimposed doublet torque/post-MVC doublet torque)]×100.
Muscle volume and cross-sectional area
Serial axial plane scans were performed using a fixed 0.2-T magnetic resonance imaging (MRI) scanner (E-Scan; ESAOTE Biomedica, Genova, Italy) along the lower portion of the left leg. The first scan was centred at the lower edge of the patella to include the origin of both the lateral and medial head of the gastrocnemius (GL and GM, respectively), with subsequent scans carried out in contiguous 7-cm sections distally. Axial plane scans were performed using T1 weighted 3D isotropic profile with the following scanning parameters: time to echo: 16 ms; repetition time: 38 ms; field of view: 180 mm×180 mm; matrix: 256×192. Subjects were supine for 15 min prior to and throughout the scan process. In total, four scans of contiguous axial images (slice thickness 8 mm and gap 2 mm) were performed on the calf of each participant. Each scan contained 7 axial images and depending on the length of the gastrocnemius between 28 and 35 contiguous images were obtained. The triceps surae anatomical cross-sectional area (ACSA) of each slice was calculated as the sum of the ACSA of GL, GM and soleus (Sol) muscles using imaging software (NIH image version 1.61/ppc; National Institutes of Health, Bethesda, USA), and multiplied by the slice thickness (inclusive of gap) to give an estimate of muscle volume (VOL). Due to limitations on the positioning of subjects and coil size it was necessary to estimate the distal portion of the Sol using third order polynomial regression from the recorded slices. The accuracy of this technique has been reported previously (Kubo et al. 2003; Narici et al. 1992). Intraclass correlation coefficients for the calculation of VOL from day to day and analysis of the same scan were high [0.98 and 0.99, respectively, n=11 males (5 EM, 6 YM); C.I. Morse et al., unpublished results]. All scans were analysed by the same investigator.
Although muscle volume is the primary focus of the present investigation ACSA is reported as a means of comparison with previous studies. ACSA of the triceps surae (TS) was calculated by summing the maximal ACSA of each of the constituent muscles of the TS (GL, GM and Sol) as described previously (Fukunaga et al. 1996).
Specific torque
The specific torque of the TS muscles was estimated as the ratio between peak torque (PT) and VOL (PT/VOL), as described previously (Fukunaga et al. 2001). According to this method, muscle volume closely approximates physiological cross-sectional area (PCSA) (Fukunaga et al. 2001) and by dividing torque (Nm) by volume (m3), values of specific torque in kN m−2 are obtained.
EMG activity
Surface EMG activity of the TA was recorded while performing maximal isometric contractions using pre-gelled two 10-mm Ag-AgCl unipolar electrodes (Medicotest, Denmark). Muscle boundaries were identified using ultrasonography to reduce the influence of cross-talk, and the electrodes placed along the mid sagittal axis of the muscle. Prior to placement of the electrodes, the skin was shaved to remove hair and the recording sites were gently rubbed using abrasive gel and cleansed using alcohol swabs to reduce inter-electrode impedance below 5 KΩ. Electrodes were placed over the TA at one-third tibia length, with the reference electrodes placed over the lateral epicondyle of the femur. The raw EMG activity was acquired with a sampling frequency of 2,000 Hz and processed with a multi channel analogue-digital converter (Biopac Systems, USA). The raw EMG signal was filtered with low and high-band band pass filters, respectively, set at 500 Hz and 10 Hz, and amplified with a gain of 2,000. The level of co-activation of the TA was assessed using the root mean square (RMS) of the raw EMG signal, calculated over 1.2 s about the peak MVC torque during PF, this was then expressed as the percentage of activity recorded from the TA during maximal dorsiflexion (Klein et al. 2001; Macaluso et al. 2000, 2002).
Physical activity measurements
Physical activity was measured in subgroups of the subjects (7 YM and 21 EM) using a uniaxial accelerometer (Actigraph Model 7164; Manufacturing Technology, Fla., USA). The actigraph is a single channel accelerometer designed to measure and record time varying accelerations ranging in magnitude from approximately 0.05 to 2.0 g. The accelerometer is band limited with a frequency response from 0.25 to 2.5 Hz. These parameters have been carefully chosen to detect normal human motion and to reject motion from other sources. Each actigraph was intitialised via a reader interface unit (RIU) using in house developed software and pre-programmed to record, in “cycle mode”, activity counts and number of steps walked at 1-min epochs. Subjects were briefed on how, and when, to wear the actigraph. An information sheet and a log, to record when the actigraph was worn, were given to each subject. The actigraph was supplied in a pouch, secured to the subject’s belt by a Velcro fastening, and positioned just anterior to the iliac crest. Subjects were asked to wear the actigraph during their waking day for at least a full week (168 h).
Files were downloaded and were viewed and checked for signs of malfunction (unusually low counts—no moderate activity with all counts <1,952; or unusually high counts—all activity vigorous with all counts >5,724; and continuous data with the same value). Files were summarised using Caloric.Bas (CSA 1999) software (option 3) to derive daily totals of: counts, steps, and estimate of kilocalorie expenditure in physical activity. Daily summaries were further derived for the number of minutes spent in each of the following physical activity categories: light <1,952 counts min−1 (<3.00 METS), moderate 1,952–5,724 counts min−1 (3.00–5.99 METS), hard 5,725–9,498 counts min−1 (6.00–8.99 METS), very hard >9,498 counts min−1 (>8.99 METS) (Freedson et al. 1998). Summary files were checked for missing or incomplete days of monitoring (less than 10 h) and further checked against the subject’s log. Incomplete days of data were excluded from calculation of daily means for, counts, steps and kilocalories.
Statistics
Independent t-tests were used to assess differences between young and elderly independent variables. Level of significance was set at the 5% level. Linear regression (Pearson product-moment correlation) was used to compare the degree of association between VOL and PF MVC. Results are given as mean (SEM) unless otherwise stated.
Results
Peak torque
PF MVC was 39% lower in the EM group compared to the YM [105.6 (4.3) Nm and 173.4 (8.1) Nm, respectively; P<0.001, Table 1].
Muscle VOL and CSA
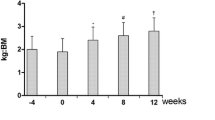
Triceps surae VOL of the EM was 19% smaller than in the YM [7.4×10−4 (0.2×10−4) m3 and 9.2×10−4 (0.5×10−4) m3, respectively; P<0.0001, Fig. 1]. A significant correlation was found between VOL and PT in the YM (R 2=0.800, P<0.0001) but not in the EM (R 2=0.056, Fig. 2).

To estimate tricep surae muscle volume approximately 30 transverse scans were obtained along the length of the tibia. The cross-sectional area of the triceps surae was then calculated and summed to obtain muscle volume. Elderly males (EM) were found to have significantly smaller triceps surae (TS) muscle volume (VOL) than young males (YM) [7.5 (0.2×10−4) m3 and 9.4 (0.5×10−4) m3, P<0.05]. The two examples are taken at one-third tibia length from a YM (A) and an EM (B)

Relationship between TS VOL and plantarflexion (PF) torque. A significant relationship is seen in YM (triangles, solid line; R 2=0.8, P<0.0001) but not EM (squares, dashed line; R 2=0.06)
Triceps surae ACSA was significantly smaller in EM than in YM (Table 1, P<0.001). In YM ACSA was correlated to PF torque (R 2=0.547, P<0.01). However, the ACSA of EM was not correlated to PF torque.
Specific torque
PF torque normalised to triceps surae volume (PT/VOL) was 19% lower in EM than in YM [140.9 (6.4) kN m−2 in EM and 190.5 (6.5) kN m−2 in YM, P<0.001]. PF torque normalised to ACSA (PT/ACSA) was also significantly lower in the EM (P<0.001), as shown in Table 1.
Activation
The EM displayed a reduced activation capacity of the PF compared to the YM [78.1 (3.1)% in the EM compared to 98.7 (0.22)% in the YM; P<0.0001]. The YM showed full activation of the PF with no difference from 100% activation. A weaker, though significant, correlation was found between PT/VOL and activation capacity in the EM (R 2=0.336, P<0.005), whereas no significant correlation was observed in the YM (R 2=0.081). When activation capacity was entered as a covariate with muscle volume, a significant correlation was found between VOL and PF torque in EM (when activation was inserted as a covariate the R 2 increased from 0.05 to R 2=0.412, P<0.01); therefore, about 40% of the variability in torque between YM and EM was explained by the variability in VOL.
Co-activation
There was no significant difference in the co-activation level of the dorsiflexors during plantarflexion between the two age groups. In the EM, TA coactivation during PF MVC was 11.5 (1.9)% and in the YM was 12.9 (1.8)%.
Physical activity
In the subset of subjects (EM group, n=22 and YM group n=10) for whom activity data was available, the EM group performed significantly fewer minutes of hard activity (6.00–8.99 METS) than the YM group [EM 0.14 (0.31) versus YM 2.40 (1.92) min day−1; P<0.01; mean difference 2.26 min day−1, 95% CI of difference 0.88–3.64]. There were no significant differences between EM and YM groups for minutes of light activity (<3 METS) per day [EM 1,406.39 (21.07) versus YM 1,411.97 (61.52) min day−1), minutes of moderate activity (3–5.99 METS) per day [EM 33.47 (21.07) versus YM 41.56 (15.10 min day−1) and the number of steps performed each day. There was a non-significant trend for estimates of daily physical activity energy expenditure (PA kcal day−1) to be lower in the EM group [EM 459.4 (196.4) versus YM 581.6 (154.6) PA kcal day−1; P=0.071]. Similarly there was a non-significant trend for activity counts per day to be lower in the EM group [EM 275,948.9 (99,202.9) versus YM 345,752.5 (89,891.7) counts day−1; P=0.068].
Discussion
The primary finding of this investigation is that PF PT/VOL of EM was significantly lower (25%) than that of YM. This seemed largely attributable to a reduced activation capacity (19%). In fact, absolute torque generation capacity of the PF was 40% lower in EM, half of which could be attributed to a reduction in activation capacity, whilst the other half could be accounted for by a decline in muscle volume. In accordance with this reduction in specific torque, indices of muscle size used in the present investigation (VOL and ACSA) were found to be weak predictors of torque in elderly males (R 2=0.05 and R 2=0.01, respectively).
In agreement with previous studies, both activation and specific torque were reduced in the present elderly by −19% and −25%, respectively, compared to YM, thus indicating that the remaining 6% of the specific torque deficit in EM could be attributed to decreased fibre-specific force or alterations in muscle architecture. However, in the present study regression analysis indicated that variability in activation capacity may account for about 30% of the variability in specific torque of elderly individuals. This suggests that in addition to the decreased activation capacity, other factors such as decreased fibre specific tension (Frontera et al. 2000) the loss of active motor units (Galea 1996; Urbanchek et al. 2001), a decrease in excitation contraction coupling (Delbono et al. 1997), alterations in tendon compliance (Narici et al. 2002), and infiltration of muscle with fat and connective tissue (Kent-Braun et al. 2000) with age, are likely to contribute to the observed decrease in specific torque.
In contrast to the results in the present study in which activation and specific torque were reduced in the elderly, Klein et al. (2001) reported a decrease in specific torque in the presence of complete activation of the elbow flexors of elderly males. As in the present study, Klein et al. (2001) adopted a modified double twitch technique to assess activation; however, the biceps brachi was placed in a shortened (albeit optimal) muscle length. Increased tendon compliance previously observed in the elderly (Narici et al. 2002), is known to reduce resting twitch torque (Loring and Hershenson 1992). It is possible that the combined effects of increased compliance and system slack introduced by the shortened muscle length in the biceps brachii, could have resulted in an over estimation of activation capacity in the elderly due to damping of the baseline twitch. Indeed, where tetanic stimulation has been used in the calculation of activation capacity an age-induced deficit is commonly reported (De Serres and Enoka 1998; Stevens et al. 2001, 2003; Yue et al. 1999), whereas when single or double twitches were used in the same muscle group no deficit in activation was reported (De Serres and Enoka 1998; Doherty et al. 1993; Klein et al. 2001; Roos et al. 1999).
In agreement with the present results, Scaglioni et al. (2002) reported in elderly males incomplete plantarflexor activation. However, the activation levels presented by Scaglioni et al. (2002) at the same joint angle were much higher than in the present study (94.8% against the present 78.1%). A likely explanation for the discrepancy is that in the present investigation double twitches rather than single twitches were used to assess activation. Previously, the use of doublets has been shown to be a more sensitive means of assessing activation compared to single twitches (Behm et al. 2001). In addition, the younger age of the subjects studied by Scaglioni et al. (2002) may account for the observed difference between the results of these authors and those of the present study (68 years compared to 74 years in the present study). Indeed, the authors commented on the lower activation levels of the oldest subject in their study, with activation as low as 71%, whereas complete activation was recorded from their youngest elderly subject.
Although the elderly population included in this study were purposefully recruited for being physically active, their level of physical activity, as judged from accelerometry, was about 21% lower than in young males, with the greatest differences seen in the amount of time spent performing hard physical activity. There is evidence that reduced physical activity leads to a decrease in neural drive (Berg et al. 1991; Duchateau and Hainaut 1987; Thom et al. 2001), probably due to a reduction in motor unit recruitment as well as firing frequency associated with a decrease in afferent input (Gandevia et al. 1990).
Hence, it is likely that disuse, in addition to ageing, contributed to the reduction in activation capacity found in the present study, and the associated reduction in specific torque. The fact that some of the reduction in activation capacity in old age may be partly explained by disuse emphasises the importance of physical activity in old age as well as during prolonged bed rest that has been found to mitigate the reduction in neural drive associated with these conditions (Kawakami et al. 2001; Milesi et al. 2000).
To our knowledge no previous data have been presented on the coactivation of the TA during PF in the elderly. In agreement with previous research on coactivation during knee flexion (Macaluso et al. 2002), knee extension (Pearson et al. 2002) and index finger abduction (Burnett et al. 2000), we found that coactivation of the TA during PF was not significantly different between YM and EM. However, during knee extension (Izquierdo et al. 1999; Macaluso et al. 2002) and elbow flexion (Klein et al. 2001) coactivation of the antagonist muscles has been shown to be greater in the elderly compared to young subjects. In both knee extension and elbow flexion increased coactivation has previously been shown to contribute to a reduced specific torque in the elderly (Klein et al. 2001; Macaluso et al. 2002). This was not shown in the present study, with most of the decrease in PF PT/VOL attributable to a decreased activation capacity. Interestingly, the coactivation of the hamstring group is reduced when the quadriceps are trained, whereas the reverse is not seen during knee flexion (Carolan and Cafarelli 1992). It is likely, therefore, that depending on the function and location of the muscle group, the changes in coactivation with ageing is variable. Compared to previous data the coactivation values observed during PF in YM (13%) were similar to those previously reported by (Maganaris et al. 1998, 2001; Magnusson et al. 2001) which changed from 15% to 20%.
The presence of a significant (albeit weak) correlation between specific torque and activation in the PF of EM in the present study, may be limited in its application to other muscles where factors such as variable muscle architecture and activation may alter specific tension. However, it is clear that both a reduced muscle mass and activation capacity contributed to the decline in the torque-generating capacity of the PF in EM.
Hence, this study showed that a deficit in muscle activation may account for a significant fraction of the differences in specific torque between YM and EM. This suggests that in the elderly a considerable increase in muscle strength with training may just be obtained by increasing activation capacity. In conclusion, this study has shown that a reduction in muscle activation capacity associated with a reduction in physical activity levels almost completely accounted for differences in specific torque between YM and EM. These findings are likely to be specific to the plantarflexors since differences may exist in activation of other muscles. No difference in antagonist muscle coactivation was found between the young and elderly groups.
References
Allen GM, Gandevia SC, McKenzie DK (1995) Reliability of measurements of muscle strength and voluntary activation using twitch interpolation. Muscle Nerve 18:593–600
Behm D, Power K, Drinkwater E (2001) Comparison of interpolation and central activation ratios as measures of muscle inactivation. Muscle Nerve 24:925–934
Berg HE, Dudley GA, Haggmark T, Ohlsen H, Tesch PAIDGA (1991) Effects of lower limb unloading on skeletal muscle mass and function in humans. J Appl Physiol 70:1882–1885
Bruce SA, Newton D, Woledge RC (1989) Effect of age on voluntary force and cross-sectional area of human adductor pollicis muscle. Q J Exp Physiol 74:359–362
Burnett RA, Laidlaw DH, Enoka RM (2000) Coactivation of the antagonist muscle does not covary with steadiness in old adults. J Appl Physiol 89:61–71
Carolan B, Cafarelli E (1992) Adaptations in coactivation after isometric resistance training. J Appl Physiol 73:911–917
Connelly DM, Rice CL, Roos MR, Vandervoort AA (1999) Motor unit firing rates and contractile properties in tibialis anterior of young and old men. J Appl Physiol 87:843–852
De Serres SJ, Enoka RM (1998) Older adults can maximally activate the biceps brachii muscle by voluntary command. J Appl Physiol 84:284–291
Delbono O, Renganathan M, Messi ML (1997) Excitation-Ca2+ release-contraction coupling in single aged human skeletal muscle fiber. Muscle Nerve [Suppl] 5: S88–92
Doherty TJ, Vandervoort AA, Taylor AW, Brown WF (1993) Effects of motor unit losses on strength in older men and women. J Appl Physiol 74:868–874
Duchateau J, Enoka RM (2002) Neural adaptations with chronic activity patterns in able-bodied humans. Am J Physiol Med Rehabil 81:S17–27
Duchateau J, Hainaut K (1987) Electrical and mechanical changes in immobilized human muscle. J Appl Physiol 62:2168–2173
Freedson PS, Melanson E. Sirard J (1998) Calibration of the Computer Science and Applications’ accelerometer. Med Sci Sports Exerc 30:777–781
Frontera WR, Suh D, Krivickas LS, Hughes VA, Goldstein R, Roubenoff R (2000) Skeletal muscle fiber quality in older men and women. Am J Physiol 279:C611–C618
Fukunaga T, Roy RR, Shellock FG, Hodgson JA, Edgerton VR (1996) Specific tension of human plantar flexors and dorsiflexors. J Appl Physiol 80:158–165
Fukunaga T, Miyatani M, Tachi M, Kouzaki M, Kawakami Y, Kanehisa H (2001) Muscle volume is a major determinant of joint torque in humans. Acta Physiol Scand 172:249–255
Galea V (1996) Changes in motor unit estimates with aging. J Clin Neurophysiol 13:253–260
Gandevia SC, Macefield G, Burke D, McKenzie DK (1990) Voluntary activation of human motor axons in the absence of muscle afferent feedback. The control of the deafferented hand. Brain 113:1563–1581
Harridge SD, Kryger A, Stensgaard A (1999) Knee extensor strength, activation, and size in very elderly people following strength training. Muscle Nerve 22:831–839
Izquierdo M, Ibanez J, Gorostiaga E, Garrues M, Zuniga A, Anton A, Larrion JL, Hakkinen K (1999) Maximal strength and power characteristics in isometric and dynamic actions of the upper and lower extremities in middle-aged and older men. Acta Physiol Scand 167:57–68
Jubrias SA, Odderson IR, Esselman PC, Conley KE (1997) Decline in isokinetic force with age: muscle cross-sectional area and specific force. Pflugers Arch 434:246–253
Kawakami Y, Akima H, Kubo K, Muraoka Y, Hasegawa H, Kouzaki M, Imai M, Suzuki Y, Gunji A, Kanehisa H, Fukunaga T (2001) Changes in muscle size, architecture, and neural activation after 20 days of bed rest with and without resistance exercise. Eur J Appl Physiol 84:7–12
Kent-Braun JA, Le Blanc R (1996) Quantitation of central activation failure during maximal voluntary contractions in humans. Muscle Nerve 19:861–869
Kent-Braun JA, Ng AV, Young K (2000) Skeletal muscle contractile and noncontractile components in young and older women and men. J Appl Physiol 88:662–668
Klein CS, Rice CL, Marsh GD (2001) Normalized force, activation, and coactivation in the arm muscles of young and old men. J Appl Physiol 91:1341–1349
Kubo K, Kanehisa H, Azuma K, Ishizu M, Kuno SY, Okada M, Fukunaga T (2003) Muscle architectural characteristics in women aged 20–79 years. Med Sci Sports Exerc 35:39–44
Lindle RS, Metter EJ, Lynch NA, Fleg JL, Fozard JL, Tobin J, Roy TA, Hurley BF (1997) Age and gender comparisons of muscle strength in 654 women and men aged 20–93 years. J Appl Physiol 83:1581–1587
Loring SH, Hershenson MB (1992) Effects of series compliance on twitches superimposed on voluntary contractions. J Appl Physiol 73:516–521
Macaluso A, De Vito G, Felici F, Nimmo MA (2000) Electromyogram changes during sustained contraction after resistance training in women in their 3rd and 8th decades. Eur J Appl Physiol 82:418–424
Macaluso A, Nimmo MA, Foster JE, Cockburn M, McMillan NC, De Vito G (2002) Contractile muscle volume and agonist-antagonist coactivation account for differences in torque between young and older women. Muscle Nerve 25:858–863
Maganaris CN, Baltzopoulos V, Sargeant AJ (1998) Differences in human antagonistic ankle dorsiflexor coactivation between legs; can they explain the moment deficit in the weaker plantarflexor leg? Exp Physiol 83:843–855
Maganaris CN, Baltzopoulos V, Ball D, Sargeant AJ (2001) In vivo specific tension of human skeletal muscle. J Appl Physiol 90:865–872
Magnusson SP, Aagaard P, Dyhre-Poulsen P, Kjaer M (2001) Load-displacement properties of the human triceps surae aponeurosis in vivo. J Physiol (Lond) 531:277–288
Milesi S, Capelli C, Denoth J, Hutchinson T, Stussi E (2000) Effects of 17 days bedrest on the maximal voluntary isometric torque and neuromuscular activation of the plantar and dorsal flexors of the ankle. Eur J Appl Physiol 82:197–205
Narici MV, Maganaris CN, Reeves ND, Capodaglio P (2003) Effect of aging on human muscle architecture. J Appl Physiol 95:2229–2234
Narici M, Landoni L, Minetti A (1992) Assessment of human knee extensor muscles stress from in vivo physiological cross-sectional area and strength measurements. Eur J Appl Physiol 65:438–444
Narici MV, Maganaris CN, Reeves N (2002) Muscle and tendon adaptations to ageing and spaceflight. J Gravit Physiol 9:137-138
Pearson SJ, Young A, Macaluso A, Devito G, Nimmo MA, Cobbold M, Harridge SD (2002) Muscle function in elite master weightlifters. Med Sci Sports Exerc 34:1199–1206
Roos MR, Rice CL, Connelly DM, Vandervoort AA (1999) Quadriceps muscle strength, contractile properties, and motor unit firing rates in young and old men. Muscle Nerve 22:1094–1103
Scaglioni G, Ferri A, Minetti AE, Martin A, Van Hoecke J, Capodaglio P, Sartorio A, Narici MV (2002) Plantar flexor activation capacity and H reflex in older adults: adaptations to strength training. J Appl Physiol 92:2292–2302
Stevens J, Binder-Macleod S, Snyder-Mackler L (2001) Characterization of the human quadriceps muscle in active elders. Arch Phys Med Rehabil 82:973–978
Stevens JE, Stackhouse SK, Binder-Macleod SA, Snyder-Mackler L (2003) Are voluntary muscle activation deficits in older adults meaningful? Muscle Nerve 27:99–101
Thom JM, Thompson MW, Ruell PA, Bryant GJ, Fonda JS, Harmer AR, De Jonge XA, Hunter SK (2001) Effect of 10-day cast immobilization on sarcoplasmic reticulum calcium regulation in humans. Acta Physiol Scand 172:141–147
Urbanchek MG, Picken EB, Kalliainen LK, Kuzon WM Jr (2001) Specific force deficit in skeletal muscles of old rats is partially explained by the existence of denervated muscle fibers. J Gerontol A 56: B191–197
Vandervoort AA, McComas AJ (1986) Contractile changes in opposing muscles of the human ankle joint with aging. J Appl Physiol 61:361–367
Young A, Stokes M, Crowe M (1985) The size and strength of the quadriceps muscles of old and young men. Clin Physiol 5:145–154
Yue GH, Ranganathan VK, Siemionow V, Liu JZ, Sahgal V (1999) Older adults exhibit a reduced ability to fully activate their biceps brachii muscle. J Gerontol A 54: M249–253
Acknowledgements
Supported by European Commission Framework V funding (‘Better-Ageing’ Project, No. QLRT-2001-00323). The authors wish to thank Dr. G. Onambele, Mr. I.J. Rothwell and Mr. T. McKee for assistance during preparation of this manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Morse, C.I., Thom, J.M., Davis, M.G. et al. Reduced plantarflexor specific torque in the elderly is associated with a lower activation capacity. Eur J Appl Physiol 92, 219–226 (2004). https://doi.org/10.1007/s00421-004-1056-y
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-004-1056-y