
Abstract
Electrical impedance tomography (EIT) is a non-invasive imaging technique for detecting blood volume changes that can visualize pulmonary perfusion. The two studies reported here tested the hypothesis that the size of the pulmonary microvascular bed, rather than stroke volume (SV), determines the EIT signal. In the first study, the impedance changes relating to the maximal pulmonary pulsatile blood volume during systole (ΔZ sys) were measured in ten healthy subjects, ten patients diagnosed with chronic obstructive pulmonary disease, who were considered to have a reduced pulmonary vascular bed, and ten heart failure patients with an assumed low cardiac output but with a normal lung parenchyma. Mean ΔZ sys (SD) in these groups was 261 (34)×10−5, 196 (39)×10−5 (P<0.001) and 233 (61)×10−5 arbitrary units (AU) (P=NS), respectively. In the second study, including seven healthy volunteers, ΔZ sys was measured at rest and during exercise on a recumbent bicycle while SV was measured by means of magnetic resonance imaging. The ΔZ sys at rest was 352 (53)×10−5 and 345 (112)×10−5 AU during exercise (P=NS), whereas SV increased from 83 (21) to 105 (34) ml (P<0.05). The EIT signal likely reflects the size of the pulmonary microvascular bed, since neither a low cardiac output nor a change in SV of the heart appear to influence EIT.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Electrical impedance tomography (EIT) makes it possible to measure dynamic changes of blood volume non-invasively (Brown et al. 1992, 1994; Eyuboglu et al. 1987; Frerichs et al. 2002; Newell et al. 2002; Smith et al. 1995; Vonk Noordegraaf et al. 1997, 2000). For pulmonary pulsatile blood volume changes, EIT is based on visualization and quantification of impedance changes within the thorax, related to changes in the blood volume during the cardiac cycle (McArdle et al. 1988; Zadehkoochak et al. 1992). Systolic pulmonary blood flow will lead to a distension of the pulmonary vascular bed and an increase in blood velocity; such a distension of the pulmonary vessels causes a decrease in electrical impedance. Equally, pulmonary vasoconstriction and vasodilatation changes the EIT signal (Smit et al. 2002; Vonk Noordegraaf et al. 1998). Since the small pulmonary vessels contain the largest pool of blood in the lungs and have the largest distensibility (Enson 1983; Rushmer 1970), these vessels dominate the pulsatile-related volume increase of the pulmonary vascular bed and therefore show up most in EIT.
We hypothesized that a reduction of the pulmonary microvascular bed would cause a decrease in EIT signal, since this reduction would be accompanied by a proportional decrease of the distensible vessels. On the other hand, the stroke volume (SV) of the heart was not expected to change the EIT signal, since this would be accompanied by an increase in pulmonary blood flow velocity but not by a change in the distensibility characteristics of the pulmonary microvascular bed. To test this hypothesis we performed two studies. First, we compared patients suffering from chronic obstructive pulmonary disease (COPD), who have a reduced pulmonary microvascular bed, and patients with a low cardiac output (chronic heart failure patients) with healthy controls of matching body mass index (BMI). Secondly, we increased SV in healthy controls by means of exercise.
Methods
A group of ten healthy volunteers without symptoms of disease of either the heart or lungs, and with normal exercise capacity, were compared under resting conditions with ten COPD patients and ten patients with left-sided heart failure due to previous myocardial infarction or cardiomyopathy, matched for BMI (Table 1). All heart failure patients had markedly reduced left ventricular contractility according to echocardiography, diminished ejection fraction on the nuclear scan at rest (mean 30% of predicted, range 20–43%) and normal aspect of lung parenchyma on chest radiographs. The diagnosis of COPD was made according to the criteria of the American Thoracic Society (1995). COPD patients with a history of systemic hypertension, ischaemic or valvular heart disease or episodes of right- and/or left-sided cardiac failure were excluded from the study.
In the second part of the study, seven healthy volunteers [six males and one female; mean age 46 years (range 36–53 years)] without complaints or signs of cardiac or respiratory diseases, and with normal lung function, were evaluated at rest and during exercise. The protocol was approved by the institutional human ethics committee. All patients and volunteers gave informed consent.
Study design
In the first part of the study the subjects were seated upright and EIT was measured in duplicate; the mean value is reported. In the second study, a change in SV was induced by exercise on a supine bicycle ergometer (LODE-MRI-ergometer, Lode, Groningen, The Netherlands). The SV was measured by means of magnetic resonance imaging (MRI),which for technical reasons could not be performed simultaneously with EIT. First, the subject was positioned in the MRI scanner and, after 10 min, measurements were made. Then, the subjects started exercising with the workload increased until their heart rate reached 120 beats/min for 1 min. Then, exercise was terminated and MRI started immediately. Due to movement artefacts it was not possible to perform the measurements while the subjects exercised. Two days after the MRI measurements, the exercise protocol was repeated using EIT, with the subjects in the same position.
Lung function
Lung function was assessed within 2 weeks of the EIT measurements. Dynamic and static lung volumes and single breath carbon monoxide diffusing capacity (DLCO) measurements were determined (SensorMedics, Yorba Linda, Calif., USA) according to the European Respiratory Society recommendations, and compared to the reference values (Quanjer et al. 1993).
EIT protocol
The EIT was performed with a 2-D applied potential tomograph (DAS-01 P Portable Data Acquisition System, IBEES, Sheffield, UK) (Brown et al. 1994; Smith et al. 1995) applying 16 Ag/AgCl electrodes (Meditrace 200, Graphic Controls, Gananoque, Ont., Canada) equidistantly attached in a transverse plane at the level of the third intercostal space, at the costo-sternal junction. A single frequent sinusoidal current (50 kHz, 5 mA peak–peak) was used and signals were processed by means of the Sheffield back-projection algorithm to yield images. Data collection was synchronized with the R-wave of the electrocardiograph (ECG) using 100 (first study) or 80 (second study) cardiac cycles to obtain one averaged data set. In the second study, 80 heart beats were averaged in the MRI measurements to determine SV, considering that breathing artefacts were eliminated by the averaging procedure. One data set contained 30 frames at 40 ms intervals.
Difference images were generated with the Sheffield tomograph and the first frame at end-diastole was defined as the reference frame. The maximal impedance change during systole, relative to end-diastole, was used as a measure of the impedance changes relating to the pulmonary pulsatile blood volume (ΔZ sys). Owing to the used back-projection algorithm of the EIT, this technique makes it impossible to provide basal impedance. Since the resistivity of blood is less than that of other tissues, blood results in a decrease in impedance (Duck 1990). This makes it possible to study the dynamics of the pulmonary blood volume changes during the cardiac cycle in the sequence of images produced by the ECG-gated EIT.
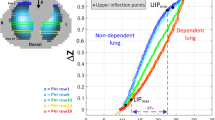
To quantify the impedance change within the lungs, a region of interest (ROI) analysis was performed. An area (“inner half circle”; Fig. 1) was chosen as the ROI, to exclude impedance increase in the anterior part of the thorax (probably due to the heart), and to exclude disturbance at the borders of the image. The average pixel value within the ROI was plotted as a function of time to show the impedance change during the cardiac cycle. All measurements of impedance change should be expressed as the value ×10−5, provided by the algorithm of the EIT device, as can be seen in the figures. The average pixel value is dimensionless as a consequence of the reconstruction algorithm based on normalized differences. Therefore, the change of the average pixel value in the sequence during the cardiac cycle relative to end-diastole was expressed as an arbitrary unit (AU).

An impedance tomogram. Left Distribution of impedance in the plane spanned by 16 electrodes with marked region of interest (ROI = “inner half circle”). Right The impedance change in arbitrary units (AU) within this ROI during a cardiac cycle
MRI velocity quantification in the pulmonary artery
MRI was performed on a 1-T whole-body system (Impact Expert, Siemens, Erlangen, Germany), using a quadruple phased-array circularly polarized body coil with two receiver antennas locally applied on the anterior, and two on the posterior, chest wall. The MR velocity mapping was performed on the main pulmonary artery. A single oblique image plane was planned on a sagittal scout image that showed the right ventricle and the main pulmonary artery. A two-dimensional gradient-echo pulse sequence was used with an excitation angle of 25°, an echo time of 6.5 ms, and a receiver bandwidth of 195 Hz. One-dimensional velocity encoding was perpendicular to the image plane. The phase-encoding steps of two acquisitions (repetition time =14 ms) were interleaved, one with velocity encoding of phase and one without. Subtraction of the resulting phase maps compensated for phase changes caused by inhomogeneity of the magnetic field, leaving only phase changes related to velocity. The temporal resolution within the cardiac cycle was thus 2×14 ms=28 ms. The velocity sensitivity was set at 150 cm/s, by adjustment of the amplitude of the velocity-encoding gradients. Field of view was (300 mm)2 and matrix size was 230×256, while the RR interval (time between two heart beats) was registered during MR acquisition of the main pulmonary artery flow.
Analysis of flow curves
In each time phase of the velocity images the cross-sectional area of the pulmonary artery was delineated by hand, in order to account for translations of the artery with respect to the image plane. The spatial mean velocity in this area was plotted against time. No aliasing due to high peak systolic velocities was encountered. Volume flow was obtained by multiplying the spatial mean velocity with the cross-sectional area. Finally, integrating the volume flow curve over systole yielded SV (Marcus et al. 1998).
Statistical analysis
The Mann-Whitney test was used to compare subject and lung function characteristics and ΔZ sys in healthy volunteers with COPD patients and with patients with heart failure. The categorical variables were evaluated by means of the chi squared test. The two-tailed Wilcoxon signed rank test for matched pairs was used to compare ΔZ sys at rest and immediately after cycling. This test was also used to compare SV at rest and after exercise. Analyses were performed with GraphPad Prism, version 3.02 for Windows (GraphPad Software, San Diego, Calif., USA). All results were reported as mean (SD). A P value of <0.05 was considered significant.
Results
The EIT measurements could be performed in all subjects both at rest and directly after exercise. Patients with heart failure were characterized by a low cardiac output leading to decreased pulsatile blood volume changes of the lungs, which is also reflected by a low DLCO (Table 1). The mean ΔZ sys in the pulmonary vessels of the heart failure patients was not significantly different from healthy subjects. Mean ΔZ sys was 261 (34)×10−5 AU in the healthy subjects, 233 (61)×10−5 AU in the heart failure patient group (P=NS) but 196 (39)×10−5 AU in the COPD patients (P<0.001) (Fig. 2).

Impedance changes at rest in 10 healthy volunteers, 10 chronic obstructive pulmonary disease (COPD) patients and 10 heart failure patients, while sitting upright. Groups were matched for body mass index. No significant change in ΔZ sys between the healthy subjects and those with heart failure was found. Difference in ΔZ sys between healthy subjects and COPD patients was significant (P<0.001)
The influence of exercise-induced increase in SV on ΔZ sys in healthy subjects is shown in Fig. 3 upper. The mean impedance change at rest was 352 (53)×10−5 AU and was 345 (112)×10−5 AU during exercise (P=NS). In contrast, SV increased from rest to just after exercise in all subjects: from 83 (21) to 105 (34) ml (P<0.05) (Fig. 3 lower)

Systolic impedance change (ΔZ sys) (upper) and stroke volume (lower) change in 7 healthy subjects at rest and after supine exercise
Discussion
This study evaluated the origin of the systolic impedance changes in the lungs. Since it is not possible to validate EIT by means of a comparable technique, we used different groups with well-described cardiac and pulmonary diseases and physiological stimuli to unravel the EIT signal of the pulmonary perfusion. The patients in the heart failure group had reduced contractility of the left ventricle, a reduced DLCO with normal lung parenchyma on high-resolution CT scans and no airway obstruction, indicative of reduced SV with a preserved pulmonary vascular bed. Conversely, the COPD patients had damaged lung parenchyma on high-resolution CT scans, and thus had a proportional reduction of the pulmonary vascular bed and a reduced DLCO. We did not measure SV, but COPD patients have a normal cardiac output (Boushy and North 1977; Scharf et al. 2002). To test the hypothesis that the amount of blood vessels in the pulmonary microvascular bed is an important determinant of the EIT signal, rather than SV, we measured the systolic impedance changes in a group of healthy subjects. We considered that diminished pulmonary blood vessels in COPD patients would lead to lowered systolic impedance changes (whereas a lowered SV in heart failure would not change the EIT signal), and found a lower ΔZ sys in the COPD patients, in comparison with healthy volunteers and heart failure patients.
We investigated the potential influence of a change in SV on the EIT signal by means of exercise. After exercise, SV increased but there was no significant change of ΔZ sys, suggesting that an increase in SV caused an increase in blood flow velocity without altering the distensibility characteristics of the pulmonary circulation. The increase in heart rate did not influence the EIT signal, as impedance change was expressed per heart beat.
To quantify the impedance change within the lungs, ROI analysis was performed. Although the choice of a ROI is arbitrary, we constructed a ROI that contained the inner part of the posterior half of the EIT image resembling the posterior parts of the lungs. The choice of this ROI was based on the maximal exclusion of cardiac regions and thoracic wall, which could be possible sources of error for the pulmonary perfusion measurements. An earlier study showed that this ROI provides highly reproducible measurements of the pulmonary perfusion (Smit et al. 2003a). Furthermore, we showed recently that by using this ROI pulmonary vascular responses to hypoxia and hyperoxia in healthy subjects and COPD patients can be measured (Smit et al. 2003b). A disadvantage of this method is that the anterior parts of the lungs are excluded from analysis.
Since we measured the impedance changes only in the posterior parts of the lungs, the impedance differences found between the healthy subjects in the first and second part of the study can be explained as a consequence of altered body position. Nuclear studies showed that there is a gravity-related perfusion inhomogenity, with the maximal perfusion in the dependent part of the lungs (Kosuda et al. 2000). Thus, the posterior parts of the lungs will be more perfused in the supine position compared to the upright position, which explains the higher EIT values of the pulmonary perfusion in the supine position (second part of the study) compared to the upright position (first part of the study). This finding is in agreement with an earlier study showing that regional differences in pulmonary perfusion can be detected by means of EIT (Kunst et al. 1998).
In conclusion, this study demonstrates that a decrease of the EIT signal, as observed in COPD patients, is most likely caused by a reduction of the pulmonary vascular bed, and not by a low cardiac output. Furthermore, a change in SV does not alter the EIT signal.
References
American Thoracic Society (1995) Standards for the diagnosis and care of patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med 152:S77–121
Boushy SF, North LB (1977) Hemodynamic changes in chronic obstructive pulmonary disease. Chest 72:565–570
Brown BH, Leathard A, Sinton A, McArdle F, Smith RW, Barber DC (1992) Blood flow imaging using electrical impedance tomography. Clin Phys Physiol Meas 13 [Suppl A]: 175–179
Brown BH, Barber DC, Morice AH, Leathard AD (1994) Cardiac and respiratory related electrical impedance changes in the human thorax. IEEE Trans Biomed Eng 41:729–734
Duck FA (1990) Physical Properties of Tissue: a comprehensive reference book. Academic Press, London, pp 171–172
Enson Y (1983) The normal pulmonary circulation. In: Baum GL, Wolinsky E (eds) Textbook of pulmonary diseases, 3rd edn. Little, Brown, Boston, pp 995–1006
Eyuboglu BM, Brown BH, Barber DC, Seagar AD (1987) Localisation of cardiac related impedance changes in the thorax. Clin Phys Physiol Meas 8 [Suppl A]:167–173
Frerichs I, Hinz J, Herrmann P, Weisser G, Hahn G, Quintel M, Hellige G (2002) Regional lung perfusion as determined by electrical impedance tomography in comparison with electron beam CT imaging. IEEE Trans Med Imaging 21:646–652
Kosuda S, Kobayashi H, Kusano S (2000) Change in regional pulmonary perfusion as a result of posture and lung volume assessed using technetium-99m macroaggregated albumin SPET. Eur J Nucl Med 27:529–535
Kunst PW, Vonk Noordegraaf A, Hoekstra OS, Postmus PE, de Vries PM (1998) Ventilation and perfusion imaging by electrical impedance tomography: a comparison with radionuclide scanning. Physiol Meas 19:481–490
Marcus JT, Vonk Noordegraaf A, de Vries PM, Van Rossum AC, Roseboom B, Heethaar RM, Postmus PE (1998) MRI evaluation of right ventricular pressure overload in chronic obstructive pulmonary disease. J Magn Reson Imaging 8:999–1005
McArdle FJ, Suggett AJ, Brown BH, Barber DC (1988) An assessment of dynamic images by applied potential tomography for monitoring pulmonary perfusion. Clin Phys Physiol Meas 9 [Suppl A]:87–91
Newell JC, Blue RS, Isaacson D, Saulnier GJ, Ross AS (2002) Phasic three-dimensional impedance imaging of cardiac activity. Physiol Meas 23:203–209
Quanjer PH, Tammeling GJ, Cotes JE, Pedersen OF, Peslin R, Yernault JC (1993) Lung volumes and forced ventilatory flows. Report Working Party Standardization of Lung Function Tests, European Community for Steel and Coal. Official Statement of the European Respiratory Society. Eur Respir J [Suppl] 16:5–40
Rushmer RF (1970) Properties of the vascular system. In: Cardiovascular dynamics, 3rd edn.Saunders, Philadelphia, pp 25–32
Scharf SM, Iqbal M, Keller C, Criner G, Lee S, Fessler HE (2002) Hemodynamic characterization of patients with severe emphysema. Am J Respir Crit Care Med 166:314–322
Smit HJ, Vonk Noordegraaf A, Roeleveld RJ, Bronzwaer JG, Postmus PE, de Vries PM, Boonstra A (2002) Epoprostenol-induced pulmonary vasodilatation in patients with pulmonary hypertension measured by electrical impedance tomography. Physiol Meas 23:237–243
Smit HJ, Handoko ML, Vonk Noordegraaf A, Faes TJ, Postmus PE, de Vries PM, Boonstra A (2003a) Electrical impedance tomography to measure pulmonary perfusion: is the reproducibility high enough for clinical practice? Physiol Meas 24:491–499
Smit HJ, Vonk Noordegraaf A, Marcus JT, van der Weiden S, Postmus PE, de Vries PM, Boonstra A (2003b) Pulmonary vascular responses to hypoxia and hyperoxia in healthy volunteers and COPD patients measured by electrical impedance tomography. Chest 123:1803–1809
Smith RW, Freeston IL, Brown BH (1995) A real-time electrical impedance tomography system for clinical use–design and preliminary results. IEEE Trans. Biomed Eng 42:133–140
Vonk Noordegraaf A, Kunst PW, Janse A, Smulders RA, Heethaar RM, Postmus PE, Faes TJ, de Vries PM (1997) Validity and reproducibility of electrical impedance tomography for measurement of calf blood flow in healthy subjects. Med Biol Eng Comput 35:107–112
Vonk Noordegraaf A, Kunst PW, Janse A, Marcus JT, Postmus PE, Faes TJ, de Vries PM (1998) Pulmonary perfusion measured by means of electrical impedance tomography. Physiol Meas 19:263–273
Vonk Noordegraaf A, Janse A, Marcus JT, Bronzwaer JG, Postmus PE, Faes TJ, de Vries PM (2000) Determination of stroke volume by means of electrical impedance tomography. Physiol Meas 21:285–293
Zadehkoochak M, Blott BH, Hames TK, George RF (1992) Pulmonary perfusion and ventricular ejection imaging by frequency domain filtering of EIT (electrical impedance tomography) images. Clin Phys Physiol Meas 13 [Suppl A]:191–196
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Smit, H.J., Vonk Noordegraaf, A., Marcus, J.T. et al. Determinants of pulmonary perfusion measured by electrical impedance tomography. Eur J Appl Physiol 92, 45–49 (2004). https://doi.org/10.1007/s00421-004-1043-3
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-004-1043-3