
Abstract
Accelerometry and heart rate (HR) are frequently used indicators of physical strain during normal daily life. The present study focused on the sensitivity and reproducibility of accelerometry (body motility, the intensity of body movement measured with accelerometry) and HR (percentage maximal heart rate reserve, %HRRmax) in the assessment of physical strain during walking in persons with a lower leg amputation, using persons without an amputation as reference. Ten patients with an amputation of the leg and ten comparison subjects performed, at an interval of 1 month, the same walking protocol three times. Subjects walked at a preferred speed and at fixed speeds. At their preferred walking speed, speed (0.63 vs 1.31 m s−1, P=0.001), body motility [0.53 vs 0.91 (arbitrary unit), P=0.001] and %HRRmax (42.5 vs 27.6, P=0.02) differed between the amputation group and the comparison group. At fixed walking speeds, only %HRRmax differed between groups (P≤0.002) and showed a session effect (P=0.02). The relationship between body motility and %HRRmax in the patient group was significantly different from that in the comparison group. It can be concluded that accelerometry is strongly related with walking speed, but not sensitive to differences and changes in economy, contrary to %HRRmax. The use of accelerometry as an indicator of the level of physical strain in persons with an amputation is not feasible. The added value of a calibration procedure has to be studied.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
In physical medicine and rehabilitation many patients have motor impairments with effects on walking economy (the energy needed in relation to walking speed). One of the patient groups is formed by persons with a leg amputation, who are an important patient group within rehabilitation medicine. In a global study on the incidence of lower extremity amputation, amputation rates varied from 2.8 to 43.9 per 100,000 persons per year (The Global Lower Extremity Amputation Study Group 2000); in the Netherlands the incidence rate is 18–20 per 100,000 (Rommers et al. 1997).
In persons with an amputation, impairments and disabilities related to walking often exist (Collin and Collin 1995), and walking economy is decreased due to their amputation, prosthesis and distorted gait (Boonstra 1994; Fisher and Gullickson 1978; Gonzalez et al. 1974; Huang et al. 1979; Pinzur et al. 1992; Ward and Meyers 1995; Waters et al. 1976). Whether this results in an increase in energy expenditure (physical strain) depends on the patient's adaptation strategy with respect to walking speed: economy, physical strain and walking speed form a triangle of mutual influencing factors. Treatment and training of persons with an amputation are, therefore, frequently focused on these factors. Knowledge about their level and changes is important to clinicians and therapists in planning and evaluating therapy and optimisation of prosthetic design, especially in the early phase of rehabilitation.
Most studies on physical strain during prosthetic walking are performed in a laboratory setting. In these studies, oxygen uptake is a generally used and accepted measure of physical strain. It is questionable, however, whether walking performance in a laboratory is representative of daily life or natural walking performance. Furthermore, although physical strain during walking is a relevant issue in itself, the combination with data on the actual amount of walking during daily life increases its clinical relevance. This issue implies the importance of physical strain assessment during natural walking, which requires the ability to determine walking periods, but also the ability to measure ambulatory physical strain over long periods of time and during normal daily life. Because measurement of oxygen uptake does not meet these requirements, this method is not considered as an option. Two alternatives that can be used to assess physical strain during daily life are heart rate (HR) measurement and accelerometry. Many studies have been performed to assess the validity and sensitivity of these methods. Generally, and despite some limitations of each method (Astrand and Rodahl 1987; Haskell et al. 1993; McArdle et al. 1991; Patterson et al. 1993; Rose et al. 1994; Schutz et al. 2001; Westerterp 1999), they are both considered to be feasible options.
During the last decade, an activity monitor (AM) has been developed (Bussmann et al. 2001), validated (Berg-Emons et al. 2000; Bussmann et al. 1998a, b, c), and used (Berg-Emons et al. 2001), and is planned to be used in evaluative studies on the treatment of persons with a leg amputation. The AM is based on long-term (>24 h) ambulatory accelerometry—with sensors on thighs and trunk—and aimed at the automatic 1-s detection of mobility-related activities, such as walking, performed during normal daily life. Additionally, ECG or HR can be measured simultaneously. Thus, based on the accelerometer signals, the AM allows the automatic and already validated detection of walking periods and the actual amount of walking (expressed in seconds) during daily life. Furthermore, physical strain can be simultaneously assessed, from the AM accelerometer signals as well as from the HR data.
In a previous study (Bussmann et al. 2000), we examined the sensitivity of accelerometry and HR in able-bodied subjects. The sensitivity to changes due to an increase in walking speed was the highest for accelerometry, while the sensitivity to changes due to walking with a brace was lower for accelerometry than for percentage maximal heart rate reserve (%HRRmax). These results suggested a discrepancy in reaction between accelerometry and %HRRmax. Because the AM will be used in persons with an amputation—with their differences in movement pattern, strain responses and economy—the characteristics of (the changes in) accelerometry and %HRRmax should be studied in more detail.
The aim of the present study therefore was to examine whether HR or accelerometry is advantageous in the assessment of physical strain during walking in persons with an amputation. The study will focus on aspects of reproducibility and sensitivity, and is based on a walking protocol with preferred and fixed walking speeds. The design, in turn, is based on some assumptions: walking economy is decreased in persons with an amputation (leading to increased physical strain during fixed walking speeds), economy improves in patients during the initial phase of rehabilitation, and increase of walking speed increases the level of physical strain. The study was intended to answer the following questions: (1) What is the reproducibility and sensitivity of accelerometry and HR in assessing physical strain during walking, in persons with an amputation (using persons without an amputation as reference)?; and (2) what is the relationship between accelerometry, HR and walking speed?
Methods
Subjects
Ten persons with a leg amputation and ten persons without an amputation participated in the study. Patients were recruited from the Departments of Rehabilitation Medicine of the University Hospital Rotterdam and Zuiderziekenhuis, and the rehabilitation centre 'De Hoogstraat'. From the start of inclusion—different for each of the involved institutes—every patient who started gait training and passed the inclusion and exclusion criteria was asked to participate in the study. The inclusion criteria were: having undergone a unilateral transtibial (TTA), through-knee (TKA) or transfemoral (TFA) amputation; being able to perform at least two of the speed levels used in the protocol; having the (initial) prosthesis less than 2 months. Exclusion criteria were diseases and impairments influencing the walking pattern. Whether a patient could be included or not was assessed by the rehabilitation specialist of the patient. Table 1 shows some characteristics of the patients. The median of the time period between amputation and receiving the prosthesis was 68 (range 39–131) days. For each patient a matched comparison subject without amputation was selected: mass (±10) kg; height (±0.10) m; age (±10) years. A t-test showed no differences between the comparison subjects and the patients with respect to mass, height and age. The comparison subjects were recruited from relatives of members of the department and patients, or by advertisements in the university hospital. The study was approved by the Medical and Ethical Committee of 'de Hoogstraat'. The subjects signed an informed consent form before participating in the study.
Protocol
In a corridor a trajectory of about 40 m was created, bordered by light gates. Subjects walked these 40 m back and forth, with smooth turns at the borders. The number and duration of walks depended on the ability of the subjects.
After a 15-min resting period in the corridor (the subject sitting in a wheelchair, reading a magazine) to obtain a steady resting state, the subjects walked for 2 min at their preferred speed. After this a 10-min resting period was prescribed, again to obtain a steady resting state. Then, a non-randomised fixed-speed test was performed, in which walking speed was increased every minute by 0.278 m s−1 (1 km h−1), starting at 0.278 m s−1. A researcher, using a one-wheeled distance meter to which a calibrated real-time cycle-speed computer was attached, determined the walking speed. The researcher was trained to walk at the prescribed walking speed, and the subjects were asked to walk next to the researcher. The walking speed was increased to the subject's maximum walking speed, or until 1.93 m s−1 (7 km h−1) was reached. The measurements of each session had a mean duration of about 45 min. After the initial session, the measurements were repeated twice (sessions 1, 2, and 3), at an interval of 1 month.
The subjects were asked to avoid excessive activities and not to drink more than two standard glasses of alcoholic drinks on the day preceding the measurements. On the day of the measurement they were not allowed to drink coffee, to smoke, or to perform heavy tasks. All measurements took place in the morning.
Instruments
Four IC-3031 uni-axial piezo-resistive accelerometers (1.5×1.5×1 cm) were used. Before each measurement the accelerometers were calibrated (+1 g, −1 g). On each leg, one sensor was attached to the skin at the ventral side of the thigh, halfway between the spina iliaca anterior superior and the upper side of the patella; with the subject standing, these sensors were sensitive in the anterior-posterior (sagittal) direction. The other two sensors were attached to the skin of the sternum, perpendicular to one another: with the subject standing, one sensor was sensitive in the anterior-posterior (sagittal) direction and one in the cranio-caudal (longitudinal) direction (Bussmann et al. 2001). Sensor placement is primarily based on the requirements of activity detection (Bussmann et al. 2001), but the same configuration is also used in the previous study about the assessment of physical strain (Bussmann et al. 2000). The sensors were attached such that, with the subject standing, their axes were as close as possible to the vertical or horizontal plane; a maximal deviation of 15° was allowed.
The accelerometers were connected to a portable Vitaport data recorder (6×11×3 cm, 500 g.) that was carried by the subject; the signals were digitally stored on a memory card, each with a sampling frequency of 32 Hz. Analysis took place after the measurements by means of the Vitagraph software and by routines written in Signal Processing and Inferencing Language (S.P.I.L.). ECG (V5 bipolar lead, according to Mason-Likar) was simultaneously recorded on the same recorder, with a sample frequency of 128 Hz. Flashes of the light gates at the borders of the trajectory were also recorded on the Vitaport recorder, using a photocell attached to the clothes of the subject.
Data analysis
Accelerometry
In the present study body motility (the intensity of body movement measured with accelerometry) was the main accelerometry variable. The analysis of the accelerometer signals was similar to that in the study performed by Bussmann et al. (2000). From each measured signal a motility signal was derived, which depends on the variability of the acceleration signal around the mean. Therefore, the measured signals of the four sensors were successively high-pass filtered, rectified and smoothed. The high-pass-filtered signal was calculated by subtracting the low-pass-filtered derivative (Finite Impulse Response, 0.3 Hz for the legs, and 0.6 Hz for the trunk) from the measured signal; smoothing occurred by moving average and downscaling the sample frequency to 1 Hz. The more intense or dynamic an activity is, the more variable the accelerometer signals, and the higher the motility of these signals. The four motility signals were added and divided by 4, to obtain the body motility signal used in this and the previous study.
Walking speed and HR
For calculating walking speed during the preferred part of the protocol, the light flashes were used. Based on the time period between flashes and the known distance between the light gates, mean walking speed during the last part of the preferred walking interval was calculated.
HR was calculated from the R-R intervals by means of the Vitagraph software. The HR during a specific walking speed period (HRspeed) was derived from the mean HR during the last 10 s of that period. Validity of this procedure was tested by pilot measurements and by detailed analysis of the data from the present study. The resting heart rate (HRrest) was derived from the mean HR in the 14th min of the resting period in the sitting posture at the beginning of a measurement. The maximum heart rate (HRmax) was determined from the formula: HRmax=220−age (e.g. Miller et al. 1993). From these data %HRRmax was calculated as: (HRspeed−HRrest)/(HRmax−HRrest)×100 (Dallmeijer et al. 1996; Janssen et al. 1996; Karvonen et al. 1957).
Statistics
Most of the statistical procedures were based on linear regression analysis with random coefficients (Verbeke and Molenberghs 1997). By means of this technique, means (per session, speed, and group) were estimated and tested on significance of differences and changes. The calculated P value was regarded as a measure of sensitivity to change or difference. With the same technique regression equations, their standard deviations of intercept and slope (both representing between-subject variance) and their residual standard deviation (representing within-subject variability) were calculated. Furthermore, differences in intercept and slope were tested on significance. The strength of relationships was expressed by Pearson's correlation coefficient (r).
Reproducibility between the three sessions was calculated for the comparison group by means of a reliability coefficient (RC): the between-subject variance divided by the between-subject variance and the within-subject variance (similar to the intraclass correlation coefficient). From the within-subject variance the standard error of measurement (SEM) was calculated by taking the root square. These variances were calculated by means of ANOVA.
For the linear regression analysis with random coefficients SAS 6.2 for Windows was used. Other statistical procedures were performed with SPSS for Windows (release 7.5.2). An alpha value of <0.05 was taken as the level of significance.
Results
Two of the ten patients (P8 and P10, Table 1) were not measured for the third time. The eight remaining patients all performed at 0.28 m s−1 and 0.56 m s−1 in the fixed speed test. Four of them (P1, P2, P7, and P9) were able to walk at least three speed levels in all sessions.
When walking at their preferred speed, body motility and walking velocity were significantly lower in the patient group than in the comparison group, while %HRRmax was significantly higher (Table 2). At their preferred speed, walking velocity, body motility and %HRRmax did not show significant changes over time within the patient group, although the patient data at preferred speed show a general trend towards the mean values of the comparison group. During the fixed speed test, no differences were found in body motility between the patient and comparison group at any speed; %HRRmax was, however, significantly higher in the patient group at each speed (Table 2). When patient data were analysed for each speed, both body motility and %HRRmax showed no significant changes over time (i.e. between sessions). When the data were pooled, however, a significant session effect was found for %HRRmax (P=0.02), but not for body motility (P=0.57). Increasing walking speed by 0.28 m s−1 (fixed walking-speed test) caused significant changes in body motility as well as in %HRRmax, both in patients and comparison subjects; the P values of body motility and %HRRmax were not different (all P=0.0001). The data on reproducibility also did not show a clear trend in favour of body motility or %HRRmax.
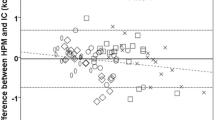
The slope of the body motility-%HRRmax regression lines of the patient data and the comparison data was significantly different (P=0.001), in contrast to the intercept (P=0.89) (Fig. 1). Both the between-subject variance (23.0 vs 18.4 %HRRmax) and within-subject variance (9.3 vs 4.1 %HRRmax) of this relationship was larger in the patient group than in the comparison group. %HRRmax, and especially body motility, showed a clear relationship with walking speed (Fig. 2). The intercept and slope of the regression line of the patient data and the comparison data were not significantly different for the body motility data (P=0.83 and 0.61, respectively), whereas for the %HRRmax data the intercept and slope were different (both P=0.001).

Scatter plot (crosses patients, circles comparisons) and estimated linear curves and regression equations of body motility against percentage maximal heart rate reserve (%HRRmax) of the patient data (dotted line), and comparison subject data (continuous line). Patients: %HRRmax=1.3+(69.0×body motility), R=0.28; comparisons: %HRRmax=2.1+(20.8×body motility), R=0.36; slope different between groups (P<0.05)

Scatter plot (crosses: patients; circles: comparisons) and estimated linear curves and regression equations of a body motility and b %HRRmax against walking speed of the patient data (dotted line) and comparison subject data (continuous line). a Patients: body motility=0.23+(0.467×walking speed), R=0.88; comparisons: body motility=0.21+(0.506×walking speed), R=0.90. b Patients: %HRRmax=14.8+(36.2×walking speed), R=0.33. Comparisons: body motility=8.5+(8.5×walking speed), R=0.40; slope and intercept different between groups (P<0.05)
Discussion
The present study has provided further insight into the potential of ambulatory accelerometry in the measurement of physical strain in persons with an amputation of the leg. Results show that accelerometry is strongly related with walking speed, but that it is not sensitive to differences and changes in economy, in contrast to %HRRmax. Therefore, accelerometry as used in the present study cannot be used as an indicator of physical strain in impaired walking.
The present study is an example of applied, patient-related research, which can be criticised from a methodological point of view, e.g. with regard to the duration of the walking intervals, the non-random testing order, and not using a reference measure for physical strain. For several reasons (e.g. poor physical capacity of the patients, time burden and load on the subjects, limitations in measurement time) an incremental walking speed protocol, with relatively small changes in walking speed and short time intervals, was the best choice from the balance between practical feasibility and methodological validity. Choices were supported by pilot measurements, which showed a clear plateau or levelling of HR within 60 s, provided that speed increments were not too large. Additional analysis of the HR data of the present study supported this assumption. Another initial comment may be that in the present study no reference measure of physical strain was used. However, to address the questions asked at the outset of this study, measurement of oxygen uptake, for example, was actually not necessary. This was partly the result of the chosen protocol, with its assumptions on "certain" changes (e.g. due to walking speed, recovery/treatment) and "certain" differences (e.g. between groups) with respect to the level of physical strain.
The differences between persons with and without amputation, with respect to walking speed and %HRRmax are in correspondence with the literature (Boonstra et al. 1994; Fisher and Gullickson 1978; Gonzalez et al. 1974; Huang et al. 1979; Jaegers et al. 1993; James 1973; Pinzur et al. 1992; Ward and Meyeres 1995; Waters et al. 1976), although some authors reported non-significant differences in physical strain at preferred walking speed, due to lowering of the walking speed (Fisher and Gullickson 1978; Gonzalez et al. 1974; Waters et al. 1976). It is generally accepted that prosthetic walking is less economical, and that walking at fixed speeds requires more energy. At preferred walking speed, body motility, %HRRmax and velocity differed between both groups. At the fixed speeds, however, body motility was not different, in contrast to %HRRmax. This indicates that the relationship between body motility and %HRRmax is not identical in both groups. This finding is demonstrated in Fig. 1: the data points of the patients are clearly positioned above the data points of the comparison group, and the slope of the patient curve is significantly steeper than the slope of the comparison regression line. The interpretation of these findings is fairly clear. Impaired walking of patients with an amputation surely leads to a decreased economy and subsequently to a higher physical strain level at fixed walking speeds. In our study, this is reflected in %HRRmax, but not in body motility. This indicates that body motility is not sensitive to differences in physical strain due to prosthetic gait, and does not support, with respect to this aspect, the use of body motility in favour of HR. This is in agreement with our previous study (Bussmann et al. 2000), in which %HRRmax was found to be more sensitive to changes due to impaired walking (walking with a brace) than body motility.
The pooled data of %HRRmax during the fixed-speed protocol showed a significant session effect. This supported the assumption that the patients' economy increased in time. A session effect was not statistically expressed in the pooled body motility data, and not in the body motility and %HRRmax data per speed, probably due to different reasons. The patient and comparison data showed that body motility is not sensitive to differences in economy; the session results suggest that body motility is not sensitive to changes in economy either. The fact that only significant changes in the pooled %HRRmax data were found can be explained from a statistical power problem of the data per speed, related to the relatively small n, a small time effect, and the large within-subject variance (expressed by RCs and SEM values, see Table 2). This despite the fact that the statistical procedure we used makes optimal use of incomplete records (e.g. absence of data for higher walking speeds). It has to be noted that the between-subject variance was substantial for both body motility and %HRRmax, contributing to high RCs. Therefore, the SEM values are also provided as an indicator of the absolute within-subject variance. If these SEM values are expressed relative to the mean differences between both groups at s 1, then no clear differences are found between body motility and %HRRmax.
The better reproducibility of body motility compared to HR found in the previous study (Bussmann et al. 2000) was not confirmed in the present study. This is merely the effect of body motility and not of %HRRmax: both in the present and in the previous study a rather low level of reproducibility was found in the determination and calculation of the %HRRmax. The %HRRmax is based upon HRmax, HRspeed, and HRrest. Additional analysis showed that difference in HRrest between sessions was an important determinant of the low reproducibility. Although these differences were also partly found in HRspeed, the %HRRmax was seriously affected by it. No logical explanations could be found for the changes in HR. The most obvious explanation—changes in drug use affecting HR, e.g. beta-blockers (Baak et al. 1987; Wilmore et al. 1985)—appeared not to be the reason. When %HRRmax is used as indicator of physical strain, careful determination of all components of it remains important.
Although their relationships are different in patients and comparison subjects, body motility and %HRRmax are significantly associated, which is also found by Eston et al. (1998). This reflects mainly the sensitivity of both body motility and HR to changes in walking speed. The relationship within the comparison group (with respect to r 2 and residual standard deviation) is comparable with the relationship found in the previous study by Bussmann et al. (2000). The regression equations found in that study are not directly comparable with the ones found in the present study, due to a different scaling of the body motility values. In the present study, the relationship between body motility and %HRRmax in the patient group was not very strong, which is due to within-subject variance and, more predominantly, to between-subject variance in the body motility-%HRRmax relationship.
The fixed-speed test showed that body motility did not differ between the groups at all three speeds. This suggests that the differences found at preferred speed were solely a result of differences in walking speed, rather than a result of inherent differences in walking pattern and movement co-ordination between the groups. This finding is also apparent from the strong relationship between body motility and walking speed in both groups, with no significant differences in regression lines. Despite a considerable difference in movement co-ordination and economy the relationship between body motility and walking speed is not different between the patient and comparison group. In the study by Bussmann et al. (2000), walking with decreased economy due to walking with a brace had no or only a small effect on body motility, but the effects were significant at higher speeds. Possibly, the speeds performed in the present study were too low to show systematic differences in body motility. Generally, it can be stated, however, that body motility is non-sensitive or shows low sensitivity to changes in economy and that body motility is probably a more feasible indicator of walking speed than of physical strain.
At the start of the study we assumed that the economy of prosthetic walking would express itself, at least partly, in body motility. However, in the present study body motility was shown to be independent of walking with or without a prosthesis, whereas it showed a close relationship with walking speed. Thus, body motility in itself can not regarded to be a valid measure of strain during prosthetic walking. One of the possible solutions for using body motility as a measure of strain is individual calibration of the body motility signal, using, for example, oxygen uptake as reference. In that case, the relationship between body motility and oxygen uptake is determined from a calibration measurement based on a standardised protocol, performed before the actual, long-term measurement during daily life. During or after this long-term measurement, motility data are transformed to oxygen uptake or energy expenditure, using a calibration equation derived from the calibration measurement. Such a procedure—applied to HR data—is also described by Haskell et al. (1993). The simultaneous availability of already validated AM data on postures and motions (such as walking) may be important; combination of these data together with data on body motility or HR—or both—may increase the validity of the assessment of physical strain during normal daily life. Bouten et al. (1994) reported little added value of individual calibration concerning the relationship between accelerometer output and energy expenditure. In their study, however, healthy subjects were involved, with probably smaller between-subject differences in economy than in the present study. Therefore, studying the feasibility and validity of individual calibration is worth being studied in the future.
The similar relationships between body motility and walking speed in patients and comparison subjects suggest that walking speed, and not movement pattern, does affect body motility. Furthermore, the clear relationship between body motility and walking speed suggests that body motility may be used as an indicator of walking speed. In combination with a calibration procedure or with another measure of physical strain (e.g. HR), body motility can be used in assessing economy of walking during daily life, similar to walking speed in the physiological cost index (Engsberg et al. 1994).
It can be concluded that accelerometry is strongly related with walking speed, but not sensitive to differences and changes in economy, in contrast to %HRRmax. When physical strain is simultaneously assessed during AM measurements in persons with an amputation—with its data on postures and motions—accelerometry is not a feasible option at this time. The added value of a calibration procedure should be studied.
References
Astrand PO, Rodahl K (1987) Textbook of work physiology; physiological bases of exercise. McGraw-Hill, Singapore, pp 188–191, 354–390, 493–497
Baak MA van, Bohm ROB, Arends BG, Hooff MEJ van, Rahn KH (1987) Long-term antihypertensive therapy with beta-blockers: submaximal exercise capacity and metabolic effects during exercise. Int J Sports Med 8:342–347
Berg-Emons HJG van den, Bussmann JBJ, Balk AH, Stam HJ (2000) Validity of ambulatory accelerometry to quantify physical activity in heart failure. Scand J Rehab Med 32:187–192
Berg-Emons H van den, Bussmann J, Keyzer-Oster D, Balk A, Stam H (2001) Mobility-related everyday activity in chronic congestive heart failure as measured with a novel activity monitor. Phys Ther 81:1502–1511
Boonstra AM, Schrama J, Fidler V, Eisma WH (1994) The gait of unilateral transfemoral amputees. Scand J Rehab Med 26:217–223
Bouten CVC, Westerterp KR, Verduin M, Janssen JD (1994) Assessment of energy expenditure for physical activity using a triaxial accelerometer. Med Sci Sports Exerc 26:1516–1523
Bussmann JBJ, Tulen JHM, Herel ECG van, Stam HJ (1998a) Quantification of physical activities by means of accelerometry: a validation study. Psychophysiology 35:488–496
Bussmann JBJ, Laar YM van de, Neeleman MP, Stam HJ (1998b) Ambulatory accelerometry to quantify motor behavior in patients after failed back surgery. Pain 74:153–161
Bussmann HBJ, Reuvekamp PJ, Veltink PH, Martens WLJ, Stam HJ (1998c) Validity and reliability of measurements obtained with an 'activity monitor' in people with and without an transtibial amputation. Phys Ther 78:989–998
Bussmann JBJ, Hartgerink I, Woude LHV van der, Stam HJ (2000) Measuring physical strain during ambulation with accelerometry. Med Sci Sports Exerc 32:1462–1471
Bussmann JBJ, Martens WLJ,Tulen JHM, Schasfoort FC, Berg-Emons HJG van den,StamHJ (2001) Measuring daily behavior using ambulatory accelerometry: the activity monitor. Behav Res Methods Instrum Comput 33:349–356
Collin C, Collin J (1995) Mobility after lower-limb amputation. Br J Surg 82:1010–1011
Dallmeijer AJ, Hopman MTE, As HHJ van, Woude LHV van der (1996) Physical capacity and physical strain in persons with tetraplegia. Spinal Cord 34:729–735
Engsberg JR, Herbert LM, Grimston SK, Fung TS, Harder JA (1994) Relation among indices of effort and oxygen uptake in below-knee amputee and able-bodied children. Arch Phys Med Rehabil 75:1335–1341
Eston RG, Rowlands AV, Ingledew DK (1998) Validity of heart rate, pedometry, and accelerometry for predicting the energy cost of children's activities. J Appl Physiol 84:362–371
Fisher SV, Gullickson G (1978) Energy cost of ambulation in health and disability: a literature review. Arch Phys Med Rehabil 59:124–133
Gonzalez EG, Corcoran PJ, Reyes RL (1974) Energy expenditure in below-knee amputees: correlation with stump length. Arch Phys Med Rehabil 55:111–119
The Global Lower Extremity Amputation Study Group (2000) Epidemiology of lower extremity amputation in centres in Europe, North America and East Asia. The global lower extremity amputation study group. Br J Surg 87:328–337
Haskell WL, Yee MC, Evans A, Irby PJ (1993) Simultaneous measurement of heart rate and body motion to quantitate physical activity. Med Sci Sports Exerc 25:109–115
Huang CT, Jackson JR, Moore NB, Fine PR, Kuhlemeier KV, Traugh GH (1979) Amputation: energy cost of ambulation. Arch Phys Med Rehabil 60:18–24
Jaegers SMHJ, Vos LDW, Rispens P, Hof AL (1993) The relationship between comfortable and most metabolically efficient walking speed in persons with unilateral above-knee amputation. Arch Phys Med Rehabil 74:521–525
James U (1973) Oxygen uptake and heart rate during prosthetic walking in healthy male unilateral above-knee amputees. Scand J Rehab Med 5:71–80
Janssen TWJ, Oers CAJM van, Rozendaal EP, Willemsen EM, Hollander AP, Woude LHV van der (1996) Changes in physical strain and physical capacity in men with spinal cord injuries. Med Sci Sports Exerc 28:551–559
Karvonen M, Kentala E, Mustula O (1957) The effects of training on heart rate. A longitudinal study. Am Med Exp Biol Fenn 35:307–315
McArdle WD, Katch FI, Katch VL (1991) Exercise physiology. Energy, nutrition and human performance. Lea & Febiger, Philadelphia, pp 804–810
Miller WC, Wallace JP, Eggert KE (1993) Predicting max HR and the HR-VO2 relationship for exercise prescription in obesity. Med Sci Sports Exerc 25:1077–1081
Patterson SM, Krantz DS, Montgomery LC, Deuster PA, Hedges SM, Nebel LE (1993) Automated physical activity monitoring: validation and comparison with physiological and self-report measures. Psychophysiology 30:296–305
Pinzur MS, Gold J, Schwartz D, Gross N (1992) Energy demands for walking in dysvascular amputees as related to the level of amputation. Orthopedics 15:1033–1037
Rommers GM, Vos LD, Groothoff JW, Schuiling CH, Eisma WH (1997) Epidemiology of lower limb amputees in the north of The Netherlands: aetiology, discharge and prosthetic use. Prosthet Orthot Int 21:92–99
Rose J, Ralston HJ, Gamble JG (1994) Energetics of walking. In: Rose J, Gamble JG (eds) Human walking. Williams & Wilkins, Baltimore, pp 45–72
Schutz Y, Weinsier RL, Hunter GR (2001) Assessment of free-living physical activity in humans: an overview of currently available and proposed new measures. Obes Res 9:368–379
Ward KH, Meyers C (1995) Exercise performance of lower-extremity amputees. Sports Med 20:207–214
Waters RL, Perry J, Antonelli D, Hislop H (1976) Energy cost of walking of amputees: the influence of level of amputation. J Bone Joint Surg 58A:42–46
Westerterp KR (1999) Physical activity assessment with accelerometers. Int J Obes 23:S45–S49
Wilmore JH, Freund BJ, Joyner MJ, Hetrick GA, Hartzell AA, Strother RT, Ewy GA, Faris WE (1985) Acute response to submaximal and maximal exercise consequent to beta-adrenergic blockade: implications for the prescription of exercise. Am J Cardiol 55:135D–141D
Acknowledgements
We would like to thank P.J. Janssens (Zuiderziekenhuis), and B. Kap (De Hoogstraat) for their valuable assistance in subject recruitment. We would also like to thank C. Moerland and the Rehabilitation Centre De Hoogstraat for their co-operation and assistance in the measurements of this study. The experiments of this study comply with the current laws of the Netherlands, in which the experiments were performed.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bussmann, J.B.J., van den Berg-Emons, H.J.G., Angulo, S.M. et al. Sensitivity and reproducibility of accelerometry and heart rate in physical strain assessment during prosthetic gait. Eur J Appl Physiol 91, 71–78 (2004). https://doi.org/10.1007/s00421-003-0916-1
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-003-0916-1