
Abstract
Objectives
Whether occupational physical activity (PA) will be assessed via questionnaires or accelerometry depends on available resources. Although self-reported data collection seems feasible and inexpensive, obtained information could be biased by demographic determinants. Thus, we aimed at comparing self-reported and objectively measured occupational sitting, standing, and walking times adjusted for socio-demographic variables.
Methods
Thirty-eight office employees (eight males, 30 females, age 40.8 ± 11.4 years, BMI 23.9 ± 4.2 kg/m2) supplied with height-adjustable working desks were asked to report sitting, standing, and walking times using the Occupational Sitting and Physical Activity Questionnaire during one working week. The ActiGraph wGT3X-BT was used to objectively measure occupational PA during the same week. Subjectively and objectively measured data were compared computing the intra-class correlation coefficients, paired t tests and Bland–Altman plots. Furthermore, repeated-measurement ANOVAs for measurement (subjective vs. objective) and socio-demographic variables were calculated.
Results
Self-reported data yielded a significant underestimation of standing time (13.3 vs. 17.9 %) and an overestimation of walking time (12.7 vs. 5.0 %). Significant interaction effects of age and measurement of standing time (F = 6.0, p = .02, η 2 p = .14) and BMI group and measurement of walking time were found (F = 3.7, p = .04, η 2 p = .17). Older employees (>39 years) underestimated their standing time, while underweight workers (BMI < 20 kg/m2) overestimated their walking time.
Conclusions
Self-reported PA data differ from objective data. Demographic variables (age, BMI) affect the amount of self-reported misjudging of PA. In order to improve the validity of self-reported data, a correction formula for the economic assessment of PA by subjective measures is needed, considering age and BMI.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Purpose
Physical inactivity (PI) is considered a major public health concern and notably contributes to numerous cardiovascular diseases, musculoskeletal complaints, obesity, type 2 diabetes as well as metabolic syndrome (Blair 2009; Blair and Brodney 1999). Sedentary behaviour has been additionally shown to be an independent risk factor for the development of various disease conditions, such as coronary heart disease, stroke, osteoporosis, or cancer (Bernstein et al. 1999; Chau et al. 2013; Li and Siegrist 2012). For occupational sitting, van Uffelen et al. (2010) stated in their review that occupational physical inactivity is associated with a higher risk of diabetes mellitus and all-cause mortality. There is only limited evidence to support positive associations between occupational sitting and health risks, in general due to a high heterogeneity of study designs, measures, and findings.
Different demographic variables have been identified to be important determinants of PI levels, such as gender, socioeconomic status, body mass index (BMI), and age (Koeneman et al. 2011; Sanchez et al. 2014). For example, higher BMI and increased age are related to decreased intensity of physical activity (PA) (Kao et al. 2014). For daily sitting time, sex, age, and educational level could be identified as socio-demographic correlates by Wallmann-Sperlich et al. (2013) in a German representative sample. Men sat longer than women, sitting time and age were negatively correlated, and sitting time as well as educational level was positively associated.
Regarding the fact that adults spend at least 30 % of their waking hours working, and this work has been developed to be more sedentary (Smith et al. 1999), the working environment needs to be seen as a major setting for the promotion of PA to overcome occupational sedentarism (Plotnikoff et al. 2005). Different studies using objective measures have shown that office workers spent between 66 and 82 % of their working time in a sedentary position (Brown et al. 2013; Thorp et al. 2012). Higher sitting times in adults at work were recently reported for individuals aged 18–29 years, obese individuals, full-time workers, employees with higher education and income, and single/divorced/widowed individuals (Clemes et al. 2015; De Cocker et al. 2014). One promising approach to increase PA levels at work is to employ height-adjustable working desks (Grunseit et al. 2013). These desks enable a switch from sitting to standing working positions.
Therefore, the assessment of physical (in)activity during working time has gained increasing research attention (Blair 2009). Accordingly, accurate values and more detailed knowledge concerning daily sitting, standing, and walking distribution seem necessary, especially in order to evaluate the effectiveness of health-promotion programmes, and to support prevention purposes.
Different methods ranging from very short to long questionnaires based on self-reports (i.e. International Physical Activity Questionnaire (Craig et al. 2003), Baecke Questionnaire (Baecke et al. 1982)) to sophisticated technical solutions to quantify the amount of PA are available to date. PA can be objectively measured by heart rate measurement, accelerometer, pedometer, sense wear bracelet, doubly labelled water method, calorimeter, or direct observation of participants (Castillo-Retamal and Hinckson 2011). The most common methods of PA data collection, particularly in large-scale epidemiological studies, are questionnaires or surveys (Prince et al. 2008). This approach serves as a feasible, time-saving, widely available, and inexpensive way for large samples. Various studies have shown that the validity of self-reports might be questionable (Ainsworth et al. 1999; Castillo-Retamal and Hinckson 2011; Prince et al. 2008). As questionnaires are mostly retrospective, reported data might suffer from misclassification due to recall errors or social desirability (Durante and Ainsworth 1996). Accurate information about PA can only be obtained from objective devices (Troiano et al. 2008). Studies which compare subjective and objective methods for assessing PA are summarized in a systematic review by Prince et al. (2008), showing low-to-moderate correlations between self-reported data and objective measures. Other studies compared reported or measured versus observed working postures (Baty et al. 1986; Laperrière et al. 2005). In using the observer estimates as the “gold standard” for validation purpose, they conclude that self-reports may be a useful addition to questionnaires and objective measurements, if posture categories are well defined.
The relationship between activity and age or BMI, respectively, is well known (Blair 2009; Cohen et al. 2015). Detailed analyses of biased self-reports concerning sitting, standing, and walking times stratified socio-demographically are missing up to now.
In the current study, actual sitting, standing, and walking times were measured with the help of the well-established accelerometer (Skotte et al. 2014) supplemented with the subjective measurement of PA via questionnaire in a sample equipped with height-adjustable working desks.
Against the cited background, we derived the following research questions:
-
1.
How is the distribution of sitting, standing, and walking times in employees with a height-adjustable working desk?
-
2.
How large is the degree of divergence between estimated and measured physical activity in our sample?
-
3.
Do the variables sex, age, BMI, and hours of work lead to larger or smaller biases in sitting, standing, and walking times in office workers?
Methods
Study design and participants
All participants were employees of the confederate Swiss health insurance (EGK). Due to the research question, only office workers supplied with a height-adjustable working desk prior to the start of the study were invited to participate (n = 80). We included both sexes between 18 and 65 years of age who worked at least 21 h per week (50 %). Employees who refused to participate or with cardiovascular diseases, trauma of the lower extremities in the past 6 months, epilepsy, pregnancy, and dizziness were excluded. The named inclusion and exclusion criteria were chosen to avoid the risk of heterogeneous subgroups. For these reasons, the sample was reduced to 38 employees (respondent rate 47.5 %). Before starting the study, we obtained informed consent of the participants. The study protocol was approved by the local ethics committee.
The demographic characteristics of the participants can be seen in Table 1. The percentage distribution of the variables sex (more females), weight group (more normal weight than overweight than underweight participants), and hours of work (more full time) significantly differed from an equal distribution (p < 0.05).
Procedures
ActiGraph wGT3X-BT
Objective sitting, standing, and walking times were measured using the ActiGraph wGT3X-BT (Pensacola, FL, US). This approach showed high sensitivity (~99 %) and specificity (100 %) in distinguishing between sitting, standing, walking, running, and cycling when worn at the thigh, described in detail elsewhere (Skotte et al. 2014). The standard deviations of acceleration enable the classification between seven different classifications (sitting, standing, walking, running, stair walking, cycling, and “moving”), using a tree structure in order to classify activity levels. However, we did differentiate only three classification patterns. The small triaxial accelerometer has an integrated inclinometer function using raw data classifying activities such as sitting, standing, and moving. “Moving” is determined by considering movements, not step counts (Steeves et al. 2015). The devices were initialized to record data at a sampling rate of 60 Hz for all three axes. Using ActiLife 6 software, all data could be downloaded and a classification of wear time could be determined according to Choi et al. (2011). For data processing, an epoch length of 60 s was used. The ActiGraph was attached with an elastic belt at the right thigh. It was allowed to remove the ActiGraph during leisure time and overnight. In our study, we focused on sitting, standing, and walking times at work. All participants got a detailed instruction for the use of the devices. The body position (sitting, standing, walking) of the participants was measured at any time for five consecutive workdays (Monday to Friday). The body positions were provided in percentages of total working time for 1 week. The wearing time of each participant could have been analysed validly by double-checked manual wear time recordings on a printed schedule and the stamping system (work time keeping) of the company. To follow the measurement process and lead to standardized behaviour, the participants were called by phone during the measurement.
Occupational Sitting and Physical Activity Questionnaire (OSPAQ)
The Occupational Sitting and Physical Activity Questionnaire (OSPAQ) was used to subjectively assess sitting, standing, and walking times by self-reported data (Chau et al. 2012). The OSPAQ asks within three questions for the number of working days, the hours of work achieved, and the percentages of the various physical activities (sitting, standing, walking, physical demanding tasks) in the past 7 days. All participants filled out the OSPAQ at the end of the same working week wearing the ActiGraph. In comparison with the objective measurement methods, the OSPAQ shows a good reliability and a moderate validity (Chau et al. 2012). Recently, the OSPAQ was compared with data collected by accelerometers in an office workplace setting and showed acceptable reliability and validity measurement properties (Jancey et al. 2014).
Statistical analyses
All calculations were performed with SPSS (version 22.0; SPSS Inc., Chicago, IL, USA). In order to describe the relationship between the subjectively and objectively measured variables, intra-class correlation coefficients (ICC) with 95 % CIs were calculated. The ICC values were rated as poor (0–0.39), moderate (0.4–0.74), excellent (0.75–1) (Fleiss 1986). Paired t tests were computed to examine the differences between the objective measures for sitting, standing, and walking times and between subjective and objective measures for each activity level. The effect size d was calculated. The observed effects were classified according to Cohen (1988) into small (d > 0.2), moderate (d > 0.5), and large (d > 0.8).
Bland–Altman plots were created to estimate heteroscedacity and to describe the deviation between subjective and objective measures. The plots show the systematic bias (mean difference between subjective and objective measures) and the limits of agreement (1.96* standard deviation of the difference between both measures) to obtain a 95 % random error component.
Separate analyses of variance with repeated measures (rANOVA) with the within-subject factor measurement (subjective vs. objective) and various between-subject variables (age, BMI, sex, hours of work) were carried out. Following significant interaction effects, post hoc tests were performed. To estimate the size of the results, the statistical effect size η 2 p was calculated. According to Cohen (1988), 0.010 < η 2 p ≤ 0.059 corresponds to a small effect, 0.059 < η 2 p ≤ 0.138 to a moderate effect and η 2 p > 0.138 to a large effect. The significance level for all tests was set at .05 a priori.
Results
Objectively versus subjectively measured sitting, standing, and walking times
Objectively measured, participants sat most of the time (77.1 %), stood 17.9 %, and walked only 5 % of their working time. The measured sitting and standing times differed significantly (t(37) = −17.92, p < .01). Table 2 summarizes the comparison of the subjectively and objectively measured sitting, standing, and walking times. The self-reported data yielded a significant subjective underestimation of standing time and a subjective overestimation of walking time in contrast to the objectively measured data. With regard to sitting time, a non-significant underestimation occurred.
Taking into account the average level of the variables, the intra-class correlation coefficients (ICC) between subjective and objective measures were only low to moderate.
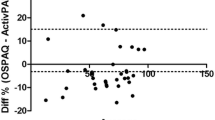
Furthermore, descriptive comparisons between subjectively and objectively measured data for sitting, standing, and walking times are shown in Fig. 1.

Comparison between subjectively and objectively measured sitting (a), standing (b), and walking times (c) using Bland–Altman plots. Each chart presents the mean difference (intermediate line) and ±1.96* standard deviation of difference (upper and lower lines), showing the limits of agreement
Effect of demographic variables on the degree of divergence
Repeated-measures ANOVA with the within-subject factor measurement of standing time (OSPAQ vs. ActiGraph) and the between-subject factor age (20–39 vs. 40–67 years) showed a large main effect of the standing time measurement (F = 14.9, p < .001, η 2 p = .29). The analysis revealed a large significant interaction effect of age and standing time measurement (F = 6.0, p = .02, η 2 p = .14). Older employees (40 years and older) underestimated their subjective standing time compared to their younger counterparts (p < .01). No such interaction was found for walking or sitting time (p > .05). In a subsequent ANOVA with the between-subject factor BMI group (underweight, normal weight, and overweight) regarding the measurement of walking time, large significant main effects for BMI group (F = 4.5, p = 0.02, η 2 p = .21) and measurement (F = 28.5, p < .001, η 2 p = .45) were found. Additionally, another large significant interaction effect for measurement and BMI group was found (F = 3.7, p = .04, η 2 p = .17). Underweight workers overestimated their walking time more than normal weight (p = .02) and overweight participants (p = .03). Both significant interaction effects are shown in Fig. 2. Regarding sitting and standing times, no such interactions were found (p > .05). Also, analyses with the between-subject factors hours of work and sex revealed no significant interaction with the differences between subjective and objective measures of sitting, standing, or walking times (all Fs < 1.60, all ps > .19).

Means and standard errors resulting from the repeated-measures ANOVA for the measurement of standing time (subjective vs. objective) and age group (left graph) and the measurement of walking time (subjective vs. objective) and BMI group (right graph) for n = 38
Discussion
The present study aimed at investigating the differences between self-reported and measured occupational sitting, standing, and walking times in employees with height-adjustable working desks. We additionally intended to evaluate the influence of demographic variables on the degree of divergence. The results show that more than three-fourth of working time is spent sitting, almost 20 % standing, and 5 % walking. This equates to within 8 h of work per day, more than 6 h spent sitting, 1.5 h standing, and almost half an hour walking. The clear predominance of sitting time is comparable to rates from employees without height-adjustable working desks (Brown et al. 2013; Thorp et al. 2012; Tudor-Locke et al. 2011), although all employees had the possibility of using their height-adjustable working desk at work and alternating their working position regularly. This is an important result showing the need for appropriate interventions to encourage for a more frequent use of height-adjustable working desks.
In the present study, employees perceive themselves as less sitting and standing and more walking compared to the objectively measured data. Our results are in line with previous studies attesting to an overestimation of subjectively measured PA (including standing and walking) and an underestimation of sedentary behaviour, especially among those who sit most of the work day (Prince et al. 2008). Social desirability concerning the knowledge about healthy behaviour and recall bias can be suggested as explanation for these discrepancies (Adams et al. 2005; Ainsworth et al. 2012). Social desirability is associated with over-reporting of activity, resulting in an overestimation of physical activity energy expenditure and in an overestimation of activity durations (Adams et al. 2005). Furthermore, for other kinds of occupational exposures, there are also various studies summarizing a low validity for self-reported data and poor correlations with objective methods, for example the duration of computer use (Ijmker et al. 2011) or the occurrence of kneeling and squatting activities (Ditchen et al. 2013).
This bias could also be seen as a result of recalling well-established and familiar behaviour patterns such as sitting and walking more easily than retrieving innovative less used standing periods at their workplace. Ijmker et al. (2011) showed that the agreement between self-reported and observed duration of computer use improved with increasing, and therefore more familiar, exposure.
In our study, older employees (40 years and older) underestimated their standing time greater than younger employees and underweight workers (BMI < 20 kg/m2) overestimated their walking time compared to normal weight and overweight participants. The overestimation of underweight workers is in line with previous findings in the literature (van Sluijs et al. 2007; Watkinson et al. 2010) and can be explained with the more active self-concept or self-perception of underweight participants resulting from the indeed higher levels of PA.
The underestimation of standing time in workers aged 40 years and older might be explained by the more challenging task of answering questionnaires and recalling their standing time. This could possibly affect the accuracy of the response (Park et al. 2001). Gender had no influence on the discrepancies which is in line with the results by Laperrière et al. (2005). The authors found only difference in length of stride between men and women resulting in different distances covered while they state the same percentages of walking time. This might have an influence on the physiological effects of walking.
When interpreting the named results, several limitations of the study should be considered. As the study was designed as pilot project, employees from only one organization were included. Furthermore, there might have been a selection bias in recruiting the employees as the study was based on voluntariness of participation resulting in a low-respondent rate. These factors led to a small sample size with no equal distribution of demographic variables and a limited internal validity and reliability. In conclusion, a larger sample with a larger variety of work tasks and workplaces spread over a larger geographical region is needed to confirm the results. Additionally, other variables could be interesting moderators of our findings such as socioeconomic status or level of fitness and leisure time PA. Identifying further variables is important to enhance the development of tailored interventions to reduce sitting time. Such intervention studies should also focus on the measurement of relevant physiological parameter such as blood flow in the lower limbs against the background of the physiological effects of different postures on the circulatory and musculoskeletal systems (Hamilton et al. 2007; Tikkanen et al. 2013). The authors show that even changes from sitting to standing are beneficial for leg muscle activity and health outcomes. Therefore, a differentiation of standing, constrained standing, slow walking and fast walking, and other postures such as running and kneeling is needed. In order to examine the health-related effects of different postures, a reliable detection is required.
Moreover, the estimation of sitting, standing, and walking times in per cent (OSPAQ) may be difficult and lead to rounded, inexact values. Heinrich et al. (2004) described that participants may assess the duration of occupational tasks better in terms of absolute time than as percentage of time. An advantage of the description in per cent is the use of continuous data instead of categorical data, like limited response categories for minutes spent sitting, standing, and walking (i.e. 0–30, 30–60 min, etc.). Furthermore, a retrospective recall for the last 7 days leads to a larger bias than an immediate daily recall. The objective measurement by the accelerometer overcomes the limitations of bias and recall, which is very common with self-reported data. Measuring PA with only seven items (OSPAQ) is a very efficient way, but has the disadvantage of no clear definition and differentiation of different postures. Due to economic reasons, it was not possible to use human observation with defined parameters, additionally. A direct observation of work activity would be helpful to interpret the data on the persistence of sitting.
Conclusions
First, due to the existing bias between self-reported and measured data, it is essential to address the problem of incorrect or invalid self-reported measurement methods, respectively. For prevalence estimations of BMI categories, a correction formula was established on the basis of self-reported and measured representative data (Kurth and Ellert 2010), which could already be applied for self-reported data (Ellert et al. 2014). To improve the validity of self-reported PA levels, subjective and objective measures from larger representative samples are needed. With the help of these data, a correction formula could be developed. A correction formula needs to consider demographic variables such as age and BMI, because they seem to affect the effect of misjudging in standing and walking time in our sample. This might be a practical solution to correct self-reported data concerning sitting, standing, and walking times which leads to an economic assessment of PA by subjective measures.
Second, our finding of a high level of sitting time in employees with a height-adjustable working desk emphasizes the need for further action to increase PA levels in office employees. There are different ways to reorganize and rebuild the office environment to provide a more “active environment” in the sense of structural prevention approaches, e.g. to overcome obstacles to stand or walk more. These recommendations were not scope of the study, but were appropriate indications for further longitudinal intervention studies. Interventions should focus on factors which lead to a low-frequent or high-frequent usage of height-adjustable working desks. Grunseit et al. (2013) named several factors for a continued use of height-adjustable working desks such as health impacts, perceived productivity while sitting and standing, practical accommodation of transitions between sitting and standing as well as electric or manual operation for height adjustment. Further interventions as described elsewhere (Shrestha et al. 2015) need to be implemented to reduce sitting times at work, i.e. computer-delivered interventions using automatic prompts.
Our results suggest furthermore implementing specific interventions for subgroups such as older aged adults and underweight adults to improve their self-assessment for standing and walking times, respectively.
Therefore, the practical implication of this study is to develop appropriate interventions that lead to a better implementation of height-adjustable working desks and the application of a correction formula to reduce misjudging of PA and establish further activities at work in order to reduce sitting time and the risk of a number of chronic diseases.
References
Adams SA, Matthews CE, Ebbeling CB, Moore CG, Cunningham JE, Fulton J, Hebert JR (2005) The effect of social desirability and social approval on self-reports of physical activity. Am J Epidemiol 161:389–398. doi:10.1093/aje/kwi054
Ainsworth BE, Richardson MT, Jacobs DR Jr, Leon AS, Sternfeld B (1999) Accuracy of recall of occupational physical activity by questionnaire. J Clin Epidemiol 52:219–227
Ainsworth BE, Caspersen CJ, Matthews CE, Masse LC, Baranowski T, Zhu W (2012) Recommendations to improve the accuracy of estimates of physical activity derived from self report. J Phys Act Health 9(Suppl 1):S76–S84
Baecke JA, Burema J, Frijters JE (1982) A short questionnaire for the measurement of habitual physical activity in epidemiological studies. Am J Clin Nutr 36:936–942
Baty D, Buckle PW, Stubbs DA (1986) Posture recording by direct observation, questionnaire assessment and instrumentation, a comparison based on a recent field study. In: Corlett NWJ, Manenica I (eds) The ergonomics of working postures: models, methods and cases. Taylor & Francis, London, pp 283–292
Bernstein MS, Morabia A, Sloutskis D (1999) Definition and prevalence of sedentarism in an urban population. Am J Public Health 89:862–867
Blair SN (2009) Physical inactivity: the biggest public health problem of the 21st century. Br J Sports Med 43:1–2
Blair SN, Brodney S (1999) Effects of physical inactivity and obesity on morbidity and mortality: current evidence and research issues. Med Sci Sports Exerc 31:S646–S662
Brown HE, Ryde GC, Gilson ND, Burton NW, Brown WJ (2013) Objectively measured sedentary behavior and physical activity in office employees relationships with presenteeism. J Occup Environ Med 55:945–953. doi:10.1097/Jom.0b013e31829178bf
Castillo-Retamal M, Hinckson EA (2011) Measuring physical activity and sedentary behaviour at work: a review. Work 40:345–357. doi:10.3233/WOR-2011-1246
Chau JY, Van Der Ploeg HP, Dunn S, Kurko J, Bauman AE (2012) Validity of the occupational sitting and physical activity questionnaire. Med Sci Sports Exerc 44:118–125. doi:10.1249/MSS.0b013e3182251060
Chau JY et al (2013) Daily sitting time and all-cause mortality: a meta-analysis. Plos One 8:e80000. doi:10.1371/journal.pone.0080000
Choi L, Liu Z, Matthews CE, Buchowski MS (2011) Validation of accelerometer wear and nonwear time classification algorithm. Med Sci Sports Exerc 43:357–364. doi:10.1249/MSS.0b013e3181ed61a3
Clemes SA, Houdmont J, Munir F, Wilson K, Kerr R, Addley K (2015) Descriptive epidemiology of domain-specific sitting in working adults: the Stormont Study. J Public Health. doi:10.1093/pubmed/fdu114
Cohen J (1988) Statistical power analysis for the behavioral sciences. Erlbaum, Hillsdale
Cohen A, Baker J, Ardern CI (2015) Association between body mass index, physical activity, and health-related quality of life in Canadian adults. J Aging Phys Act. doi:10.1123/japa.2014-0169
Craig CL et al (2003) International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc 35:1381–1395. doi:10.1249/01.MSS.0000078924.61453.FB
De Cocker K, Duncan MJ, Short C, van Uffelen JG, Vandelanotte C (2014) Understanding occupational sitting: prevalence, correlates and moderating effects in Australian employees. Prev Med 67:288–294. doi:10.1016/j.ypmed.2014.07.031
Ditchen DM, Ellegast RP, Hartmann B, Rieger MA (2013) Validity of self-reports of knee-straining activities at work: a field study with 6-month follow-up. Int Arch Occup Environ Health 86:233–243. doi:10.1007/s00420-012-0758-4
Durante R, Ainsworth BE (1996) The recall of physical activity: using a cognitive model of the question-answering process. Med Sci Sports Exerc 28:1282–1291
Ellert U, Brettschneider AK, Wiegand S, Kurth BM (2014) Applying a correction procedure to the prevalence estimates of overweight and obesity in the German part of the HBSC study. BMC Res Notes 7:181. doi:10.1186/1756-0500-7-181
Fleiss JL (1986) The design and analysis of clinical experiments. Wiley, New York
Grunseit AC, Chau JYY, van der Ploeg HP, Bauman A (2013) “Thinking on your feet”: a qualitative evaluation of sit-stand desks in an Australian workplace. BMC Public Health. doi:10.1186/1471-2458-13-365
Hamilton MT, Hamilton DG, Zderic TW (2007) Role of low energy expenditure and sitting in obesity, metabolic syndrome, type 2 diabetes, and cardiovascular disease. Diabetes 56:2655–2667. doi:10.2337/db07-0882
Heinrich J, Blatter BM, Bongers PM (2004) A comparison of methods for the assessment of postural load and duration of computer use. Occup Environ Med 61:1027–1031
Ijmker S, Huysmans MA, van der Beek AJ, Knol DL, van Mechelen W, Bongers PM, Blatter BM (2011) Software-recorded and self-reported duration of computer use in relation to the onset of severe arm-wrist-hand pain and neck-shoulder pain. Occup Environ Med 68:502–509. doi:10.1136/oem.2010.056267
Jancey J, Tye M, McGann S, Blackford K, Lee AH (2014) Application of the Occupational Sitting and Physical Activity Questionnaire (OSPAQ) to office based workers. BMC Public Health 14:762. doi:10.1186/1471-2458-14-762
Kao MC, Jarosz R, Goldin M, Patel A, Smuck M (2014) Determinants of physical activity in America: a first characterization of physical activity profile using the National Health and Nutrition Examination Survey (NHANES). PM&R 6:882–892. doi:10.1016/j.pmrj.2014.03.004
Koeneman MA, Verheijden MW, Chinapaw MJ, Hopman-Rock M (2011) Determinants of physical activity and exercise in healthy older adults: a systematic review. Int J Behav Nutr Phys Act 8:142. doi:10.1186/1479-5868-8-142
Kurth BM, Ellert U (2010) Estimated and measured BMI and self-perceived body image of adolescents in Germany: Part 1—general implications for correcting prevalence estimations of overweight and obesity. Obes Facts 3:181–190. doi:10.1159/000314638
Laperrière E, Messing K, Couture V, Stock S (2005) Validation of questions on working posture among those who stand during most of the work day. Int J Ind Ergon 35:371–378. doi:10.1016/j.ergon.2004.10.006
Li J, Siegrist J (2012) Physical activity and risk of cardiovascular disease—a meta-analysis of prospective cohort studies. Int J Environ Res Public Health 9:391–407. doi:10.3390/ijerph9020391
Park DC, Polk TA, Mikels JA, Taylor SF, Marshuetz C (2001) Cerebral aging: integration of brain and behavioral models of cognitive function. Dialogues Clin Neurosci 3:151–165
Plotnikoff RC, Prodaniuk TR, Fein AJ, Milton L (2005) Development of an ecological assessment tool for a workplace physical activity program standard. Health Promot Pract 6:453–463. doi:10.1177/1524839904263730
Prince SA, Adamo KB, Hamel ME, Hardt J, Connor Gorber S, Tremblay M (2008) A comparison of direct versus self-report measures for assessing physical activity in adults: a systematic review. Int J Behav Nutr Phys Act 5:56. doi:10.1186/1479-5868-5-56
Sanchez A, Grandes G, Ortega Sanchez-Pinilla R, Torcal J, Montoya I, Group P (2014) Predictors of long-term change of a physical activity promotion programme in primary care. BMC Public Health 14:108. doi:10.1186/1471-2458-14-108
Shrestha N, Ijaz S, Kukkonen-Harjula KT, Kumar S, Nwankwo CP (2015) Workplace interventions for reducing sitting at work. Cochrane Database Syst Rev 1:CD010912. doi:10.1002/14651858.CD010912.pub2
Skotte J, Korshoj M, Kristiansen J, Hanisch C, Holtermann A (2014) Detection of physical activity types using triaxial accelerometers. J Phys Act Health 11:76–84. doi:10.1123/jpah.2011-0347
Smith MJ, Conway FT, Karsh BT (1999) Occupational stress in human computer interaction. Ind Health 37:157–173
Steeves JA, Bowles HR, McClain JJ, Dodd KW, Brychta RJ, Wang J, Chen KY (2015) Ability of thigh-worn ActiGraph and activPAL monitors to classify posture and motion. Med Sci Sports Exerc 47:952–959. doi:10.1249/MSS.0000000000000497
Thorp AA, Healy GN, Winkler E, Clark BK, Gardiner PA, Owen N, Dunstan DW (2012) Prolonged sedentary time and physical activity in workplace and non-work contexts: a cross-sectional study of office, customer service and call centre employees. Int J Behav Nutr Phys Act 9:128. doi:10.1186/1479-5868-9-128
Tikkanen O et al (2013) Muscle activity and inactivity periods during normal daily life. PLoS ONE 8:e52228. doi:10.1371/journal.pone.0052228
Troiano RP, Berrigan D, Dodd KW, Masse LC, Tilert T, McDowell M (2008) Physical activity in the United States measured by accelerometer. Med Sci Sports Exerc 40:181–188. doi:10.1249/mss.0b013e31815a51b3
Tudor-Locke C, Leonardi C, Johnson WD, Katzmarzyk PT (2011) Time spent in physical activity and sedentary behaviors on the working day the American time use survey. J Occup Environ Med 53:1382–1387. doi:10.1097/Jom.0b013e31823c1402
van Sluijs E, Griffin S, van Poppel M (2007) A cross-sectional study of awareness of physical activity: associations with personal, behavioral and psychosocial factors. Int J Behav Nutr Phys Act 4:53
van Uffelen JG et al (2010) Occupational sitting and health risks: a systematic review. Am J Prev Med 39:379–388. doi:10.1016/j.amepre.2010.05.024
Wallmann-Sperlich B, Bucksch J, Hansen S, Schantz P, Froboese I (2013) Sitting time in Germany: an analysis of socio-demographic and environmental correlates. BMC Public Health. doi:10.1186/1471-2458-13-196
Watkinson C, van Sluijs EM, Sutton S, Hardeman W, Corder K, Griffin SJ (2010) Overestimation of physical activity level is associated with lower BMI: a cross-sectional analysis. Int J Behav Nutr Phys Act 7:68. doi:10.1186/1479-5868-7-68
Acknowledgments
We appreciate the encouragement of the Swiss health insurance (EGK Gesundheitskasse) for their infrastructural and institutional support. We are also grateful for participants’ commitment and compliance during the testing and intervention period. Special thanks to Christoph Moor for his study assistance with the ActiGraph measures.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None.
Rights and permissions
About this article

Cite this article
Wick, K., Faude, O., Schwager, S. et al. Deviation between self-reported and measured occupational physical activity levels in office employees: effects of age and body composition. Int Arch Occup Environ Health 89, 575–582 (2016). https://doi.org/10.1007/s00420-015-1095-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00420-015-1095-1