
Abstract
Background
The use of benchmark dose (BMD) and the 95% lower confidence limit of benchmark dose (BMDL) have been gaining popularity not only in experimental studies but also in epidemiological studies including those on toxicology of cadmium (Cd), a ubiquitous hazardous element in the environment. However, the reproducibility of BMD and BMDL values has seldom been examined.
Objectives
This study was initiated to determine whether consistent BMD and BMDL values are obtained for similar non-exposed populations, i.e., the populations with no anthropogenic exposure to Cd in a single nation of Japan.
Methods
Cd (an exposure marker), α1-microglobulin (α1-MG), β2-microglobulin (β2-MG) and N-acetyl-β-D-glucosaminidase (NAG) (three effect markers of tubular dysfunction) levels in the urine of adult Japanese women from five previous publications of this study group were examined. Overall, data were available for 17,375 cases (in 16 prefectures) regarding Cd, α1-MG and β2-MG, and 6,409 cases (in ten prefectures) regarding NAG. The data were used to calculate BMD and BMDL values taking advantage of the hybrid approach (Budtz-Jǿrgensen et al. in Biometrics 57:698–706, 2001). It was possible to calculate BMD and BMDL values for α1-MG and β2-MG for all of the 16 prefectures with 17,375 cases, whereas the values for NAG were successfully calculated for nine prefectures with 5,843 cases.
Results
The application gave BMD values of 1.92, 2.46 and 2.32 μg Cd/g cr for α1-MG, β2-MG and NAG, respectively, and BMDL values of 1.83, 2.32 and 2.09 μg Cd/g cr. Large inter-prefectural variations were observed in the BMD and BMDL; there was about fourfold difference both in BMD and in BMDL calculated for α1-MG and β2-MG in 16 prefectures, and the variation was greater (i.e., by about sevenfold) in BMD and BMDL for NAG in nine prefectures. A survey of relevant literature revealed variation in BMD and BMDL values of similar folds as observed in the present analyses in five studies of Japanese populations. Multiple regression analyses taking BMD or BMDL as a dependent variable and age, CR concentration and Cd concentration as independent variables showed both BMD and BMDL were significantly influenced by Cd concentration in cases of α1-MG and β2-MG, whereas BMD and BMDL for NAG was by CR.
Conclusions
Even when the analysis was conducted in a single nation, both BMD and BMDL for the Cd effect markers varied by ca. fourfold when examining α1-MG or β2-MG and the values varied by ca. sevenfold for NAG among Cd-non-exposed populations. The most influential factors in the study population may include urine density and Cd levels in the urine.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The benchmark dose (BMD) approach [including the use of the 95% lower confidence limit of benchmark dose (BMDL)] has gained popularity as a tool for estimating no-effect level in hazard associated with non-cancer responses (Bailer et al. 1997; Crump 2002; Filipsson et al. 2003; Slob et al. 2005; Muri et al. 2009). The application of these methods to epidemiological data has also been recommended (Bailer et al. 1997; Budtz-Jǿrgensen et al. 2001; Morales and Ryan 2005; Sand et al. 2006).
The application has been expanded from metal toxicology in environmental health [e.g., organic mercury on the central nervous system development (van Wijngaarden et al. 2006), cadmium on renal tubular dysfunction (as to be reviewed in the “Discussion” section), on pancreatic function (Lei et al. 2007) and on osteoporosis (Suwazono et al. 2010a)] to occupational health issues, for example, effects of lead on haematopoiesis (Murata et al. 2003; Karita et al. 2005) and manganese on Parkinsonian syndrome (Park et al. 2006; Santamaria and Sulsky 2010).
The methods have been used also in studies on lifestyle-related factors, such as alcohol consumptions on liver function (Dakeishi et al. 2004, 2006) and working hours on mental and physical fatigue symptoms (Suwazono et al. 2007). Recently, the European Food Safety Authority (2009a, b) employed BMD approach to issue an opinion regarding Cd levels in foods. However, the number of groups of populations analyzed in each of these studies was generally limited, and the stability or reproducibility of the BMD and BMDL values was seldom examined, leading to questions regarding whether the application of the BMD and BMDL methods to similar populations would give consistent values.
For the present study, data were available on Cd and the tubular effect marker levels in urine from more than 17,000 adult women in non-polluted areas in 16 prefectures in Japan. The present study was initiated to investigate whether consistent BMD and BMDL values would be obtained when the same procedures for BMD and BMDL calculation were applied to multiple but similar groups of people who lived in Cd-non-polluted areas in Japan with no occupational exposure to Cd.
Materials and methods
Ethical issues
The study protocol for the BMD and BMDL analyses was approved by the Ethics Committee of the Kyoto Industrial Health Association, Kyoto, Japan. Each of the participating women provided informed consent in writing at the time of each survey.
Data sources and methods of urinalyses
Urine samples were collected from 17,468 adult women in Cd-non-polluted areas in 16 prefectures (Prefectures 1, 2, 4, 5, 6, 14, 15, 16, 17, 18, 20, 26, 34, 39, 40 and 47; see Fig. 1 for locations) all over Japan from the northern-most Prefecture 1 to the southern-most Prefecture 47. Japan is divided into 47 prefectures, primarily by watershed mountain ranges, rivers or seas (see Fig. 1).

The locations of the sixteen prefectures where urine samples were collected. The sixteen prefectures of urine sample collection are shown with shades. The numbers correspond to the numbers in Table 2. Note that Japan consists of 47 prefectures in total
For the present study, the data were cited from the six previous publications of Ezaki et al. (2003a), Tsukahara et al. (2003) for Prefectures 1, 4, 14, 15, 20, 26, 34, 39, 40 and 47, Moriguchi et al. (2005a, 2010) for Prefectures 5, 6 and 17, Yamagami et al. (2006) for Prefecture 16 and Ikeda et al. (2011) for Prefectures 2 and 18.
Urine samples were analyzed for Cd, the three renal tubular dysfunction markers of α1-microglobulin (α1-MG), β2-microglobulin (β2-MG), and N-acetyl-β-D-glucosaminidase (NAG), and creatinine (CR) by graphite furnace atomic absorption spectrometry [0.5 μg/l as the material limit of determination (LOD) for Cd], latex methods (0.6 mg/l for α1-MG and 1.0 μg/l for β2-MG,), a NAG test kit from Shionogi Pharmaceuticals, Osaka, Japan (0.01 unit/l for NAG) and a clinical auto-analyzer method (0.05 mg/l for CR), respectively. The analyses were conducted using the same methods throughout all studies. The results were corrected for CR concentration (Jackson 1966). The quality of Cd determination was certified by Round Robin (German Society of Occupational Medicine and Environmental Medicine, 2001–2009). The qualities of other assays were approved by Japan Medical Association (2001–2009) (Ezaki et al. 2003a, b; Moriguchi et al. 2010).
BMD and BMDL calculations
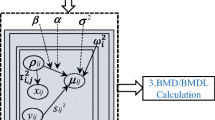
The hybrid approach by Budtz-Jǿrgensen et al. (2001) was employed. BMR = 5%, and BMD05 and BMDL05 (rather than BMD10 and BMDL10) were used; hereafter, BMD05 and BMDL05 are described as BMD and BMDL, respectively, unless otherwise specified.
α1-MG, β2-MG and NAG were introduced after logarithmic conversion for quasi-normal distribution of the response parameters (van Wijngaarden et al. 2006). For the present study, 93 cases with β2-MG ≥ 1,000 μg/g cr (Ezaki et al. 2003b; Bernard 2008) were deleted, and α1-MG and β2-MG data were available for the 17,375 cases in 16 prefectures (to be called ‘the total prefecture database’). NAG was measured in 6,409 cases. Nevertheless, preliminary analyses for BMD and BMDL revealed that dose–response relationship was not significant (p > 0.05) in Pref. 16 (as to be detailed in the “Results” section), and 566 cases in the prefecture were excluded in further analyses so that 5,843 cases in 9 prefectures were employed as ‘the selected prefecture database’ with complete sets of three effect markers of α1-MG, β2-MG and NAG (Table 1).
Distribution patterns and statistical analysis
Age and CR were distributed normally. A log-normal distribution was assumed for Cd, α1-MG, β2-MG and NAG. Accordingly, the distributions of age and CR were presented as arithmetic means and arithmetic standard deviations (i.e., AM ± ASD), whereas the Cd, α1-MG, β2-MG and NAG data were presented as geometric means and geometric standard deviations [GM (GSD)]. In calculating GM and GSD, the value below the corresponding LOD was assumed to be half the LOD.
Wilcoxon test and Spearman rank correlation analysis were employed when an assumption of a normal distribution was not applicable to the parameter distribution. Multiple regression analysis was also used. In evaluating correlation coefficients, a value of 0.2 was selected as a cut-off to identify the significance when the number was >100 (Ezaki et al. 2003a).
Results
Populations surveyed
The basic parameters are presented in Table 1 for individual prefectures and the total study population (Table 1) in terms of means (AMs or GMs) and standard deviations (ASDs or GSDs) for age, CR (as a urine density marker), Cd (as an exposure marker), and α1-MG, β2-MG and NAG (as the three effect markers). As NAG was measured only in selected prefectures, the numbers of available cases for NAG are shown separately from the numbers of the parameters other than NAG. The parameters are presented for the total prefecture database and for the selected prefecture database (‘A’ and ‘B’ in Table 1).
When the total prefecture database was taken as an example, the number of cases by prefecture was not uniform, distributing in a broad range from 650 (Prefecture 16) to 3,081 cases (Prefecture 26). In examining NAG, the fewest cases were observed in Prefecture 4 (104 cases), and the most abundant cases (1,789 cases) were in Prefecture 26. The lowest and highest levels of the exposure marker, Cd, were 0.79 and 2.67 μg/g cr as GM, respectively, with >3-fold difference. The grand GM was 1.34 μg/g cr. Prefectural GM values for α1-MG, β2-MG and NAG were distributed in relatively narrow ranges with the minimum and the maximum of 2.06–3.12 mg/g cr for α1-MG, 94–133 μg/g cr for β2-MG and 2.89–4.17 units/g cr for NAG. The GSDs by prefecture were mostly <2, but the GSD for NAG was up to 3 in four prefectures out of ten studied.
BMD and BMDL by prefectures
The calculation for BMD and BMDL values was possible for α1-MG and β2-MG in all prefectures in the total prefecture database (Table 2). In cases of NAG BMD and BMDL, calculation was not possible in 6 prefectures as no data were available (Table 1). In addition, the calculation results were not reliable in Pref. 16 due to poor dose–response relationship with p > 0.05 for the regression coefficient. Thus, the values were available for 9 prefectures with 5,843 cases (the selected prefecture database). BMD and BMDL for α1-MG and β2-MG were recalculated for the selected prefectures in parallel with NAG (Table 3).
The BMD and BMDL for the total study population of 17,375 cases were 1.92 and 1.83 μg Cd/g cr, respectively, for α1-MG, 2.46 and 2.32 μg Cd/g cr for β2-MG (Table 2). There were variations in the calculated BMD and BMDL values for α1-MG and β2-MG among 16 prefectures. For example, the minimum and the maximum BMD were 0.78 and 3.18 μg Cd/g cr, respectively, for α1-MG, and 1.05 and 4.82 μg Cd/g cr, respectively, for β2-MG. Similar variations were observed also in BMDL values for α1-MG and β2-MG.
With regard to BMD and BMDL for NAG (Table 3), the values for a total of 5,843 cases in 9 prefectures were 2.32 and 2.09 μg Cd/g cr, respectively. Although the number of prefectures available for NAG BMD and BMDL calculation was limited to nine, the BMD and BMDL values for each of the nine prefectures distributed in a range of 0.70–4.98 μg Cd/g cr for BMD, and 0.53–3.50 μg Cd/g cr for BMDL.
Comparison on BMD and BMDL values for effect markers
Comparison of 16 BMDs for α1-MG and β2-MG (Table 2) by Wilcoxon test indicated a significant difference (p = 0.013) among the BMDs of the two effect markers. A similar comparison of BMDL values also showed a significant difference (p = 0.013). A further comparison of the three pairs of α1-MG and β2-MG, α1-MG and NAG, and β2-MG and NAG (Table 3), however, detected no significant differences (p > 0.05) in any pairs. The absence of the significant differences may be due to limited number (n = 9) of available prefectures (Table 3).
Factors possibly influencing BMD or BMDL
In a preliminary analysis, correlation of age (AM in years), CR (AM in g/l) and Cd (GM in μg/g cr) with BMD and BMDL for α1-MG, β2-MG and NAG was examined by calculating Spearman rank correlation coefficient. Cd correlated significantly (p < 0.01–0.05) with all of BMD and BMDL for α1-MG, β2-MG and NAG. In contrast, age and CR did not show significant correlation (p > 0.05) with any of BMD or BMDL for the three markers.
Subsequently, multiple regression analyses were conducted taking one of the BMD or BMDL for α1-MG, β2-MG or NAG as a dependent variable, and age, CR and Cd as independent variables (thus calculation of 6 cases). In all of the 6 cases examined (Table 4), the regression coefficient (r) was significant (p < 0.01) with R 2 of 0.74–0.96. Among the three independent variables, Cd correlated significantly (p < 0.01–0.05) with BMD and BMDL of both α1-MG and β2-MG. In addition, significant correlations of age with BMD and BMDL of α1-MG were observed. In case of NAG, CR showed significant (p < 0.01) correlations with both BMD and BMDL.
Discussion
The analysis of 17,375 urine samples from non-exposed adult women for α1-MG and β2-MG and 5,843 cases for NAG followed by application of the hybrid approach resulted in calculated BMD values of 1.92, 2.46 and 2.32 μg Cd/g cr for α1-MG, β2-MG and NAG, respectively, with the corresponding BMDL values of 1.83, 2.32 and 2.09 μg Cd/g cr (Tables 2, 3). Substantial variations were observed in BMD and BMDL values among prefectures. There was 4.1-fold to 4.6-fold difference in the BMD and BMDL values between the minimum and the maximum for prefectures when they were calculated for α1-MG and β2-MG in 16 prefectures, and the variation was even greater (i.e., 6.6-fold to 7.1-fold) for NAG in nine prefectures (Tables 2, 3). Attempts to identify BMD- and BMDL-influencing factors indicated that Cd levels in urine were most influential to BMD and BMDL of α1-MG and β2-MG among age, average urine density (in terms of the CR level in the urine) and the Cd concentration (Table 4), but none of them affected both BMD an BMDL of all of the three effect markers. Previously, Kobayashi et al. (2008) observed age-dependent decrease in BMD and BMDL values for β2-MG. It was not possible in the present analyses to observe such effects (Table 4).
To compare the present study results with the values in literature, studies were sorted for BMD and BMDL values of effect markers among the populations exposed to Cd either occupationally or environmentally, or among the populations with no anthropogenic exposures to Cd. Table 5 summarizes the results of the literature review along with the relevant results of the present study at the top of the table.
Five studies (Kobayashi et al. 2006a, b, 2008; Shimizu et al. 2006; Uno et al. 2005) out of ten (the studies mentioned above plus Hong et al. 2004; Jin et al. 2004; Chen et al. 2006; Shao et al. 2007) studied Japanese populations. α1-MG was examined in one study (Suwazono et al. 2006), whereas β2-MG and NAG were measured in 15 and 12 groups of people, respectively. An examination of the reported BMD and BMDL values clearly indicates that the use of the 84% cut-off always gives smaller values than the 97.5% cut-off, as expected. Of particular interest is the range of reported BMD and BMDL values for each of the three effect markers. When studies on Japanese women (with 84% cut-off) were selected to ensure similarity in lifestyles with cases of the present study, the literature BMD and BMDL values for β2-MG were in ranges of 0.9–3.8 and 0.7–3.2 μg Cd/g cr, respectively, and the values were 0.8–4.7 and 0.6–3.7 μg Cd/g cr for NAG (Table 5). Thus, the minimum and the maximum values reported differ by four to sixfold for BMD and BMDL of β2-MG and NAG, respectively (the bottom of Table 5). The observation suggests that the variations reported in literature were apparently similar to what was observed in the present study (Tables 2, 3). A similar within-Japan variation was reported in a recent review of four studies in Japan, and one study each in China and Sweden (Suwazono et al. 2010b). As for the potential modifier for BMD and BMDL values, the present analyses suggest that Cd in urine affects BMD and BMDL of both α1-MG and β2-MG, age influences BMD and BMDL of α1-MG and β2-MG and CR those of NAG (Table 4).
It is of practical interest to identify an effect marker that gives the lowest BMD and BMDL among the three effect markers studied. The present analysis indicated that BMD and BMDL for α1-MG appeared to be lower than the values for and β2-MG when the total prefecture database was employed (Table 2). However, comparison of NAG with α1-MG and β2-MG by use of the selected prefecture database failed to identify any superior marker. Nevertheless, higher sensitivity for α1-MG in comparison with β2-MG is consistent with the previous observations by this study group (Moriguchi et al. 2004, 2005b) on better sensitivity of α1-MG than β2-MG as an indicator of Cd-induced effects on the renal tubules. Overall, published data on α1-MG-based BMD and BMDL values are still limited (Table 5) to examine whether α1-MG is the best marker of Cd-induced health effects.
An overall evaluation of the results of the present analysis in combination with findings in the literature suggests that both BMD and BMDL values vary substantially depending on the populations studied. Such was the case even when all data are from non-exposed adult women in a single nation.
References
Bailer AJ, Stayner LT, Smith RJ, Kuempel ED, Prince MM (1997) Estimating benchmark concentrations and other noncancer endpoints in epidemiology studies. Risk Anal 17:771–780
Bernard A (2008) Biomarkers of metal toxicity in population studies; research potential and interpretation issues. J Toxicol Environ Health A71:1259–1265
Budtz-Jǿrgensen E, Reiding N, Grandjean P (2001) Benchmark dose calculation from epidemiological data. Biometrics 57:698–706
Chen L, Jin T, Huang B, Nordberg G, Nordberg M (2006) Critical exposure level of cadmium for elevated urinary metallothionein—an occupational population study in China. Toxicol Appl Pharmacol 215:93–99
Crump K (2002) Critical issues in benchmark calculations from continuous data. Crt Rev Toxicol 32:133–153
Dakeishi M, Iwata T, Ishii N, Murata K (2004) Effects of alcohol consumption on hepatocellular injury in Japanese men. Tohoku J Exp Med 202:31–39
Dakeishi M, Murata K, Tamura A, Iwata T (2006) Relation between dose and no-observed-adverse-effect level in clinical research: effects of daily alcohol intake on blood pressure in Japanese salesmen. Risk Anal 26:115–123
European Food Safety Authority (2009a) Use of the benchmark dose approach in risk assessment: guideline of the SAcientific Committee. EFSA J 1150:1–72
European Food Safety Authority: Panel on Contaminants in the Food Chain (2009b) Scientific opinion on cadmium in food on a request from the European Commission on cadmium in food. EFSA J 980:1–139
Ezaki T, Tsukahara T, Moriguchi J, Furuki K, Fukui Y, Ukai H, Okamoto S, Sakurai H, Honda S, Ikeda M (2003a) No clear-cut evidence for cadmium-induced tubular dysfunction among over 10,000 women in the Japanese general population; a nationwide large-scale survey. Int Arch Occup Environ Health 76:186–196
Ezaki T, Tsukahara T, Moriguchi J, Furuki K, Fukui Y, Ukai H, Okamoto S, Sakurai H, Honda S, Ikeda M (2003b) Analysis for threshold levels of cadmium in urine that induce tubular dysfunction among women in non-polluted areas in Japan. Int Arch Occup Environ Health 76:197–204
Filipsson AF, Sand S, Nilsson J, Victorin K (2003) The benchmark dose method—review of available models, and recommendations for application in health risk assessment. Crit Rev Toxicol 33:505–542
Hong F, Jin T, Zhang A (2004) Risk assessment on renal dysfunction caused by co-exposure to arsenic and cadmium using benchmark dose calculation in a Chinese population. Biometals 17:573–580
Ikeda M, Fukui Y, Ohashi F, Sakuragi S, Moriguchi J (2011) Low cadmium levels in urine of residents in two prefectures where cadmium levels in locally harvested brown rice are higher than in other prefectures in Japan. Biol Trace Elem Res 139:217–227
Jackson S (1966) Creatinine in urine as an index of urinary excretion rate. Health Phys 12:843–850
Jin T, Wu X, Tang T, Nordberg M, Bernard A, Ye T, Kong Q, Lundström N-G, Nordberg GF (2004) Environmental epidemiological study and estimation of benchmark dose for renal tubular dysfunction in a cadmium-polluted area in China. Biometals 17:525–530
Karita K, Yano E, Dakeishi M, Iwata T, Murata K (2005) Benchmark dose of lead inducing anemia at the workplace. Risk Anal 25:957–962
Kobayashi E, Suwazono Y, Uetani M, Inaba T, Oishi M, Kido T, Nishijo M, Nakagawa H, Nogawa K (2006a) Estimation of benchmark dose as the threshold levels of urinary cadmium, based on excretion of total protein, β2-microglobulin, and N-acetyl-β-D-glucosaminidase in cadmium nonpolluted regions in Japan. Environ Res 101:401–406
Kobayashi E, Suwazono Y, Uetani M, Inaba T, Oishi M, Kido T, Nishijo M, Nakagawa H, Nogawa K (2006b) Estimation of benchmark dose for renal dysfunction in a cadmium non-polluted area in Japan. J Appl Toxicol 26:351–355
Kobayashi E, Suwazono Y, Dochi M, Honda R, Nishijo M, Kido T, Nakagawa H (2008) Estimation of benchmark dose as threshold levels of urinary cadmium, based on excretion of β2-microglobulin in cadmium-polluted and non-polluted regions in Japan. Toxicol Lett 179:108–112
Lei L-J, Jin T-Y, Nordberg M, Chang X-U (2007) Estimation of benchmark dose for pancreatic damage in cadmium-exposed smelters. Toxicol Sci 97:189–195
Morales KH, Ryan LM (2005) Benchmark dose estimation based on epidemiologic cohort data. Environmetrics 16:435–447
Moriguchi J, Ezaki T, Tsukahara T, Furuki K, Fukui Y, Okamoto S, Ukai H, Sakurai H, Ikeda M (2004) α1-Microglobulin as a promising marker of cadmium-induced tubular dysfunction, possibly better than β2-microglobulin. Toxicol Lett 148:11–20
Moriguchi J, Ezaki T, Tsukahara T, Fukui Y, Ukai H, Okamoto S, Shimbo S, Sakurai H, Ikeda M (2005a) Effects of aging on cadmium and tubular dysfunction markers in urine from adult women in non-polluted areas. Int Arch Occup Environ Health 78:446–451
Moriguchi J, Ezaki T, Tsukahara T, Furuki K, Fukui Y, Okamoto S, Ukai H, Sakurai H, Ikeda M (2005b) α1-Microglobulin levels and correlation with cadmium and other metals in urine of non-smoking women among general populations in Japan. Toxicol Environ Chem 87:119–133
Moriguchi J, Inoue Y, Kamiyama S, Sakuragi S, Horiguchi M, Murata K, Fukui Y, Ohashi F, Ikeda M (2010) Cadmium and tubular dysfunction marker levels in urine of residents in non-polluted areas with natural abundance of cadmium in Japan. Int Arch Occup Environ Health 83:455–466
Murata K, Sakai T, Morita Y, Iwata T, Dakeishi M (2003) Critical dose of lead affecting δ-aminolevulinic acid levels. J Occup Health 45:209–214
Muri SD, Schlatter JR, Brüschweiler BJ (2009) The benchmark dose approach in food risk assessment: is it applicable and worthwhile? Food Chem Toxicol 47:2906–2925
Park RM, Bowler RM, Eggerth DE, Diamond E, Spencer KJ, Smith D, Gwiazda R (2006) Issues in neurological risk assessment for occupational exposure; the Bay Bridge welders. Neurotoxicology 27:373–384
Sand S, von Rosen D, Victorin K, Filipsson AF (2006) Identification of a critical dose level for risk assessment: developments in benchmark dose analysis of continuous endpoints. Toxicol Sci 90:241–251
Santamaria AB, Sulsky SI (2010) Risk assessment of an essential element: manganese. J Toxicol Environ Health 73:128–155
Shao B, Jin TY, Wu XW, Kong OH, Ye TT (2007) Application of benchmark dose (BMD) in estimating biological exposure limit (BEL) to cadmium. Biomed Environ Sci 20:460–464
Shimizu A, Kobayashi E, Suwazono Y, Uetani M, Oishi M, Inaba T, Kido T, Nogawa K (2006) Estimation of benchmark doses for urinary cadmium based on β2-microglobulin excretion in cadmium-polluted regions of the Kakehashi River basin, Japan. Int J Environ Health Res 16:329–337
Slob W, Moerbeek M, Rauniomaa E, Piersma AH (2005) A statistical evaluation of toxicity study designs for the estimation of the benchmark dose in continuous endpoints. Toxicol Sci 84:167–185
Suwazono Y, Sand S, Vahter M, Filipsson AF, Skerfving S, Lidfeldt J, Akesson A (2006) Benchmark dose for cadmium-induced renal effects in humans. Environ Health Perspect 114:1072–1076
Suwazono Y, Nagashima S, Okubo Y, Uetani M, Kobayashi E, Kido T, Nogawa K (2007) Estimation of the number of working hours critical for the development of mental and physical fatigue symptoms in Japanese male workers—application of benchmark dose method. Am J Ind Med 50:173–182
Suwazono Y, Sand S, Vahter M, Skerfving S, Lidfeldt J, Åkesson A (2010a) Benchmark dose for cadmium-induced osteoporosis in women. Toxicol Lett 197:123–127
Suwazono Y, Uetani M, Åkesson A, Vahter M (2010b) Recent applications of benchmark dose method for estimation of reference cadmium exposure for renal effects in man. Toxicol Lett 198:40–43
Tsukahara T, Ezaki T, Moriguchi J, Furuki K, Fukui Y, Ukai H, Okamoto S, Sakurai H, Ikeda M (2003) No significant effect of iron deficiency on cadmium body burden or kidney dysfunction among women in the general population in Japan. Int Arch Occup Environ Health 76:275–281
Uno T, Kobayashi E, Suwazono Y, Okubo Y, Miura K, Sakata K, Okayama A, Ueshima H, Nakagawa H, Nogawa K (2005) Health effects of cadmium exposure in the general environment in Japan with special reference to the lower limit of the benchmark dose as the threshold level of urinary cadmium. Scand J Work Environ Health 31:307–315
van Wijngaarden E, Beck C, Shamlaye CF, Cernichiari E, Davidson PW, Myers GJ, Clarkson TW (2006) Benchmark concentrations for methyl mercury obtained from the 9-year follow-up of the Seychelles Child Development Study. Neurotoxicology 27:702–709
Yamagami T, Ezaki T, Moriguchi J, Fukui Y, Okamoto S, Ukai H, Sakurai H, Aoshima K, Ikeda M (2006) Low-level cadmium exposure in Toyama City and its surroundings in Toyama prefecture, Japan, with references to possible contribution of shellfish intake to increase urinary cadmium levels. Sci Total Environ 362:56–67
Acknowledgments
The authors are grateful to the administration and staff of the Kyoto Industrial Health Association, Kyoto, Japan, for their interest in and support for this study.
Conflicts of interest
The authors declare that they have no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Sakuragi, S., Takahashi, K., Hoshuyama, T. et al. Variation in benchmark dose (BMD) and the 95% lower confidence limit of benchmark dose (BMDL) among general Japanese populations with no anthropogenic exposure to cadmium. Int Arch Occup Environ Health 85, 941–950 (2012). https://doi.org/10.1007/s00420-012-0734-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00420-012-0734-z