
Abstract
Background
Background levels of metals of toxicological or industrial importance have been reported for several populations in the world. The information on the levels of metals of industrial, occupational or clinical importance in blood of general Japanese populations is however still scarce.
Objectives
The objectives of the study were to establish background levels of Cd, Cr, Mn, Ni and Pb in blood of Japanese population using inductively coupled plasma-sector field mass spectrometry (ICP-SF-MS), which was expected to be sensitive enough to measure low-level Pb in blood of general populations. For this purpose, women, rather than men, were studied to minimize the effect of smoking. An additional objective was to examine possible contamination from devices in phlebotomy process.
Methods
Blood samples were collected in 2000’s from 1,420 adult women in eight prefectures of no known anthropogenic environmental metal pollution in Japan, and the samples were subjected to ICP-SF-MS analyses after wet digestion with extra-pure nitric acid. Ultra pure water samples aspirated into blood sampling vacuum tubes were analyzed to detect possible metal contamination.
Results
Contamination of blood samples from phlebotomy device was detected for Cr and possibly for Mn and Ni, whereas it was below measurable levels with regard to Cd, Ni and Pb. Under this limitation, GM metal concentrations in blood were 1.23 μg/l for Cd, 0.55 μg/l for Cr, 13.2 μg/l for Mn, 1.81 μg/l for Ni and 15.8 μg/l for Pb. Cd and Pb tended to increase in association with age, whereas Cr, Mn and Ni tended to decrease. Smoking induced elevation both in Cd and in Pb in blood. It was also made clear that the ICP-SF-MS is reliable for measurements of Cd, Mn and Pb in blood allowing evaluation even on an individual basis, while the results of Cr and Ni should be reliable on a group basis (e.g., n ≥ 5). Limitation in compatibility was discussed between the results by ICP-SF-MS and that by traditional graphite furnace atomic absorption spectrometry.
Conclusions
ICP-SF-MS is a reliable method of blood analysis for Cd, Mn and Pb even for the evaluation on an individual basis. Cr and Ni analyses should be reliable on a group basis, probably due to limited performance inherent to the analysis principle and matrix. Possible contamination from phlebotomy devices with Cr should be taken into account in evaluating the results.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Biological exposure monitoring has been winning popularity not only in occupational health fields where the concept has been first established but also in environmental health and clinical practice. The target chemicals may be classified into four groups, i.e., organic solvents, inorganic metals, pesticides and others (Mikeev 1996a, b).
In the present study, five metals [ i.e., cadmium (Cd), chromium (Cr), manganese (Mn), nickel (Ni) and lead (Pb)] of industrial, environmental or clinical importance (e.g., Bader et al. 1999; Herber 1999; Ikeda et al. 2000a, b; Apostoli et al. 2002; Polizzi et al. 2002; Muttamara and Leong 2004; Kim et al. 2005; Al-Saleh et al. 2006; Afridi et al. 2006, 2009; Ekong et al. 2006; Heitland and Köster 2006; Vitayavirasuk et al. 2006; Coelho et al. 2007; McKelvey et al. 2007; Antoniou et al. 2008; Bazzi et al. 2008; Farzin et al. 2008; Gao et al. 2008; Jusko et al. 2008; Kummrow et al. 2008; Bulat et al. 2009) were selected, and the levels in the blood of populations in areas with no known anthropogenic environmental metal pollution in Japan were determined by inductively coupled plasma-sector field mass spectrometry (ICP-SF-MS), as a sensitive tool for metal analysis at low levels (Schramel et al. 1997; Zhang et al. 1997; White 1999). For this purpose, women were selected to minimize the effects of smoking. The results were summarized in the present report and discussed with existing databases on blood metals in conjunction with environmental exposure to metals in Japan.
Materials and methods
Blood samples
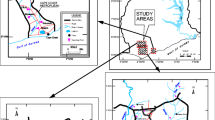
Blood samples, 1,214 in total, collected in a previous study from adult women in six prefectures (Prefectures 2–4 and 6–8; Fig. 1) in Japan in 2002 (Tsukahara et al. 2003) were subjected to the analysis. In addition, 100 and 106 blood samples, respectively, were collected in 2008 from adult women in other two prefectures (Prefectures 1 and 5; Fig. 1) for the present study. Thus, 1,420 blood samples were available in total. Of the 1,420 women, 1,383 women (97%) gave information on smoking habits through a self-administered questionnaire survey; 978 (71%), 167 (12%) and 238 women (17%) were never, current and ex-smokers, respectively (Tsukahara et al. 2003, and the present study).

The locations of the eight prefectures where blood samples were collected. The eight prefectures of blood sample collection are shown with shades. The numbers correspond to the numbers in Table 2. Note that Japan consists of 47 prefectures in total
The survey covered eight prefectures in total scattering all over the country of Japan (for locations, see Fig. 1); Japan consists of 47 prefectures in total. No anthropogenic metal pollution of the general environment had been known in the regions where the women lived, and none of them had ever engaged in work with use of target metals as confirmed by the questionnaire surveys (Tsukahara et al. 2003; the present study).
The study protocol was approved by the Ethics Committee in Kyoto Industrial Health Association. Each of women provided informed consent in writing.
Blood analyses
An aliquot (0.1 ml) of each blood sample was taken into a PFA vial (made of perfluoroalkyl vinyl ether; a product of ARAM Co., Osaka, Japan) and mixed with 0.5 ml extra-pure nitric acid (for specification, see the Reagent section). The vessel was sealed, and the mixture was wet-ashed in a microwave digestion system (ETHOS 1, Milestone Srl, Sorisole, Italy) by linear heating up to 180°C for 30 min and keeping at the temperature for 20 min, followed by cooling down to room temperature (Mizushima et al. 1996). The ash was taken up in 5 ml ultra pure water (for preparation, see the “Reagents” section) and subjected to ICP-SF-MS analysis.
The instrument used was a double-focusing sector field ICP-MS (EMENT2, Thermo Fisher Scientific Inc, Bremen, Germany). The operation conditions are summarized in Table 1.
The performance of the system was approved by German Society on Occupational Medicine and Environmental Medicine (G-EQUAS 44 in 2010) for Cd and Pb in occupational and environmental medicine fields, and for Cr, Mn and Ni in occupational medicine fields; no test sample was available for Cr, Mn and Ni in environmental medicine field.
The results of internal quality assurance with SERO AS (Billingstad, Norway) were such that the accuracy (%) [CV (%; n = 10) in parenthesis] with SERO201505 was 93.5 (4.6) for Cd, 76.0 (16.9) for Cr, 100.8 (1.6) for Mn, 94.7 (24.1) for Ni and 101.2 (1.9) for Pb and that with SERO201605 were 100.6 (9.5) for Cd, 99.7 (3.0) for Cr, 100.3 (2.3) for Mn, 97.6 (16.5) for Ni and 97.2 (1.4) for Pb. Thus, there was a good agreement of the AM measured values with the certified values for all five metals, but the precision might be relatively low for Ni and possibly for Cr also.
The reagent blank–based limits of determination [LOD (A)] were calculated as 3xSD; the SD was obtained after determination of 10 reagent blank samples (i.e., ultra pure water being employed in place of blood, mixed with nitric acid and heated in PFA vials by microwave). The 3xSD values were 0.0001, 0.0076, 0.0049, 0.0132 and 0.0024 μg/l for Cd, Cr, Mn, Ni, and Pb, respectively. In blood analyses, the wet-ash of 0.1 ml of blood was taken up in 5 ml ultra pure water (see above) so that each sample was diluted by 50 times. Taking this dilution into consideration, the LOD (A) was calculated (after rounding) to be 0.1, 0.4, 0.2, 0.7 and 0.1 μg/l for Cd, Cr, Mn, Ni and Pb, respectively.
The instrument limits of determination (μg/l) [LOD (B)] were calculated as 3xSD obtained by 10 times determination of ultra pure water; the 3xSD values were 0.0006, 0.0006, 0.0003, 0.0012 and 0.0003 μg/l for Cd, Cr, Mn, Ni and Pb, respectively. Taking the 50-times dilution into consideration, the LOD (B) was set at 0.03, 0.03, 0.02, 0.06 and 0.02 μg/l for Cd, Cr, Mn, Ni, and Pb, respectively.
Testing of phlebotomy device for possible contamination with metals
Two types of popularly used vacuum tubes for phlebotomy were tested for possible metal contamination in the process of blood sampling. The tubes tested were 5-ml tubes containing heparin Na (65 units) (as anti-coagulant) and 5-ml tubes with ethylenediaminetetraacetic acid (EDTA) 2 K salt (3.6 mg) (both from TERUMO, Tokyo, Japan). Needles (21G x 1 1/2; MN-2138MS) and holders were also from TERUMO, Tokyo, Japan.
After connecting a needle to a holder, the sharp top of the needle was inserted into ultra pure water, and 5-ml of the water was aspirated into a vacuum tube by connection of a vacuum tube to the other end of the needle in the holder. The anti-coagulant in the vacuum tube was thoroughly dissolved by gentle shaking. The water in the tube was taken out, and 0.1 ml aliquot was mixed with 0.5 ml extra-pure nitric acid. The mixture was subjected to metal analysis (without microwave treatment) as if the water were a blood sample. The procedure was repeated with five sets each of fresh needle–holder–vacuum tube combination for two types of the tubes. Five portions of the ultra pure water (without vacuum tube treatment) were also analyzed for metals. Thus, 15 analyses were conducted in total.
Reagents
Nitric acid of high purity (TAMAPURE-AA-100)TM was purchased from Tama Chemicals, Kawasaki, Japan. The specification concentrations were <100 ng/l for all 5 metals, and observed concentrations were <10 ng/l for Cd, Cr and Mn and <50 ng/l for Ni and Pb. Ultra pure water was obtained using the Milli-Q system, Nihon Millipore, Tokyo, Japan.
Statistical analysis
Concentrations of the five metals in blood distributed log-normally. Accordingly, the metal concentrations were expressed in terms of geometric means (GMs) and geometric standard deviations (GSDs). A normal distribution was assumed for age to be expressed in terms of arithmetic means (AMs) and arithmetic standard deviations (ASDs). In calculating GM values, the values below LOD (A) or LOD (B) were taken as if they were half the LOD.
Possible age dependency was examined by simple (SRA) and multiple regression analysis (MRA). Correlation was examined by correlation matrix analysis. ANOVA followed by multiple comparison (Scheffé), t-test and χ2 test was also employed.
Results
Populations surveyed
Ages of the 1,420 women in eight prefectures were distributed in a wide range from 20 to 81 years, with a median of 45 years. The number of the subjects and their median age by prefecture were various, i.e., 100 women (median age; 49 years), 122 (44 years), 209 (44 years), 100 (34 years), 106 (45 years), 486 (46 years), 47 (39 years), and 250 (50 years) in Prefecture 1, 2, 3, 4, 5, 6, 7 and 8, respectively.
Reproducibility of metal levels by ICP-SF-MS
In order to confirm that the values obtained by ICP-SF-MS were reproducible, 60 samples from one prefecture (Prefecture 4) were analyzed twice with a lapse in time of one year; before and during the 1 year storage, the blood samples were kept in tightly capped acid-washed tubes at −30°C and thawed immediately before each of the analyses. The regression line between the two measurements (without logarithmic conversion) showed that the measured values were exactly reproducible in case of Cd, Mn and Pb; the slopes were essentially 1, and the intercepts on the vertical axis were very close to zero, with r values next to 1 (p < 0.01). Thus, the values were thought to be reproducible even on an individual basis (Table 2). In cases of Cr and Ni, however, r values were as small as <0.2, and the slopes were not close to 1; the findings were taken to suggest that the reproducibility on an individual basis was hardly expectable.
Similar analyses after logarithmic conversion of the metal concentrations gave somewhat greater r values even for Cr and Ni (with p < 0.05) and also greater slopes. The 95% upper limits however did not reach 1.
Nevertheless, the differences between GMs for the first and the second measurements were statistically insignificant (p > 0.10). To examine the smallest number of cases necessary for group basis evaluation, the 60 cases of the first measurement were divided into several cases of an equal size and possible difference in GMs was examined by multiple comparison test (Scheffé). No significant difference (p > 0.10) was detected in 12 GM values when the 60 cases were divided into 12 subgroups of an equal size (n = 5). The results were taken to indicate that five samples would be sufficient to obtain reproducible GM values.
Possible contamination of blood samples from phlebotomy device
The results of testing are summarized in Table 3, by type of vacuum tubes employed. It should be noted that a fresh needle–holder complex was used for each of the five vacuum tubes of the two types.
Extent of contamination varied substantially depending on vacuum tube types and metals. Cr was detected at measurable amounts in both types. The level was similar in both types with GM = 0.05 μg/l but the maximum appeared to be different, i.e., Max = 0.06 μg/l in Type 1 and 0.08 μg/l in Type 2. In case of Mn, contamination was measurable in Type 1 (GM = 0.28 μg/l) in Type 1 whereas it was not so in Type 2. With regard to Cd, Ni and Pb, no measurable contamination was detected irrespective of tube types.
Metal levels in blood
The GM levels of the five target metals among 1,420 cases as a whole are summarized in the top line in Table 4 together with medians (Med) and the maximum (Max). GSD values are given in the footnote as GSD ranges. For calculating GM and GSD values, the reagent blank–based LOD for each metal [(LOD (A); for details, see the “Materials and methods” section)] was employed. In cases of Cd, Mn and Pb, all values measured were greater than LOD (A), and 1.23, 13.2 and 15.8 μg/l were obtained as GM for Cd, Mn and Pb, respectively. With regard to Cr and Ni, the values were <LOD (A) in 399 cases (28.1%) and 37 cases (2.6%), respectively. Assuming that the values below corresponding LOD (A) had been half the LOD (A), 0.55 and 1.81 μg/l were obtained as GM for Cr and Ni, respectively. It should be noted that Cr values were <LOD (A) in more than one-fourth of the total cases. When the instrument limit of determination [i.e., LOD (B)] for Cr (0.03 μg/l) was applied, the number of <LOD (B) cases was reduced to 10 (0.7%). The GM value (0.55 μg/l) however stayed essentially unchanged.
Thus, the GM values were various subject to the metals; the level was highest for Pb (15.8 μg/l), followed by Mn (13.2 μg/l). Levels for two metals, Ni (1.81 μg/l) and Cd (1.23 μg/l), were about one-tenth of that of Pb and Mn, and the level was lowest for Cr (0.55 μg/l). Cr in addition showed wide variation in distribution with the largest GSD (1.97–2.48). In fact, the minimum was below the LOD as described above. The wide variation in observation might be related to the analytical difficulty of this metal and possible contamination from phlebotomy devices as to be discussed elsewhere.
When the metal concentrations were evaluated by prefectures (Table 4), the GM levels were highest in Prefecture 3 for Cd, Cr and Ni, but it was in Prefecture 7 for Mn and Prefecture 6 for Pb. ANOVA followed by multiple comparison test (Scheffé) showed that age distribution was not uniform among the prefectures as previously discussed. Cd, Cr and Ni (after logarithmic conversion) were significantly (p > 0.01 to 0.05) higher in Prefecture 3 than in most of other prefectures, and it was also the case for log Pb in Prefecture 6. For Mn, however, no significant (p > 0.10) bias was observed among prefectures (Table 4).
Multiple regression analysis was conducted taking age and prefectures as independent variables and one of the five metal concentrations (after logarithmic conversion) as a dependent variable. The analysis showed that age was an effective variable for Cd, Cr, Mn and Pb (p < 0.01) and also for Ni (p < 0.05). R 2 was 0.014 to 0.110, suggesting that the power of all nine independent variables in combination was limited.
Correlation between two metal levels
Correlation matrix was calculated first on the prefectural basis (n = 8) (in the upper-right corner in Table 5). Correlations between the five metals were all insignificant (p > 0.10). In case of analysis on the individual basis (n = 1,420) (in the lower left corner of Table 5), there were several pairs for which the correlation between the pair was statistically significant (p < 0.05). Nevertheless, some of the differences might be over-evaluated due to the large number of cases, e.g., p < 0.05 despite |r| was as small as 0.063 for the pair of Mn and Pb. Significant correlation of Cd with Pb (r = 0.235, p < 0.01) and with Mn (r = 0.168, p < 0.01) might deserve attention. The correlation coefficient was even higher (r = 0.501, p < 0.01) for the pairs of Cr and Ni. The latter observation should however be taken as yet inconclusive due to the technical limitations on the Cr and Ni determination as discussed above.
A close correlation was observed for Cd, Cr, Mn and Pb with age. This point will be discussed later.
Effects of aging on metal levels in blood
As the multiple regression analysis showed that the age was an influential variable on Cd, Cr, Mn and Pb in blood (after logarithmic conversion), the effect of age on the logarithm of metal level was examined by simple regression analysis (top half in Table 6). The analysis revealed that log Cd and log Pb increased and log Mn decreased as a function of age. |r| was 0.118 (p < 0.01) for log Cr or greater. The 95% ranges for slopes did not include zero. In cases of log Cr and log Ni, the values decreased as age progressed, but |r| was smaller (i.e., 0.118 for log Cr and 0.058 for log Ni) although p was <0.01 probably due to the large number of cases (n = 1,420).
To examine whether the observation was reproducible on a single prefecture basis, similar analyses were conducted with cases in Prefecture 6 (the bottom half in Table 6), where the number of cases per prefecture was largest (n = 486) among the eight prefectures (Table 4). The increases in log Cd and log Pb with age were noted. For log Cr and log Ni, the decreasing trends were reproduced but the |r|’s were not significant (p > 0.10), partly because less number of cases was available.
Effects of smoking on metal levels in blood
Metal levels in blood were compared between 1,216 non-smokers (i.e., never smokers and ex-smokers in combination) and 167 current smokers by ANOVA (followed by multiple comparison by Schffé). The analysis showed that significant difference (p < 0.01) was observed between the two groups for Cd and Pb, but not for other three metals. GMs (GSDs) for non-smokers and current smokers were 1.20 μg/l (1.70) and 1.41 μg/l (1.67) in case of Cd, and 15.6 μg/l (1.53) and 17.1 μg/l (1.48) in case of Pb, respectively.
Further analysis by MRA taking either log Cd or log Pb as a dependent variable and age and smoking habits (non-smoking vs. current smoking) as independent variables showed that both age and smoking habits were influential (p < 0.01 for all cases) although R 2 was small (i.e., 0.070 for log Cd and 0.120 for log Pb).
Discussion
The present analysis of 1,420 blood samples from adult Japanese women showed that the GM concentrations in blood were 1.23 μg/l for Cd, 0.55 μg/l for Cr, 13.2 μg/l for Mn, 1.81 μg/l for Ni and 15.8 μg/l for Pb (Table 4). Cd and Pb increased with age as previously observed (Watanabe et al. 1983, 1985; Moriguchi et al. 2005). Smoking induced increases in Cd and Pb in blood also as previously observed in urine (Ikeda et al. 2005). It was further made clear that the ICP-SF-MS is reliable for measurements of Cd, Mn and Pb on an individual basis, while the results of Cr and Ni are reliable on a group basis (n ≥ 5).
Although only two types of vacuum tubes were tested, the phlebotomy device study (Table 3) made it clear that metal contamination would occur especially with Cr and to a lesser extent with Mn, possibly both from needles and from vacuum tubes including anti-coagulant reagents. With this regard, Minoia et al. (1992) compared metal concentrations in blood samples obtained by use of steel syringe with that by Teflon catheter. The difference in the concentration (AMs in μg/l; syringe vs. catheter) was remarkable for Cr (5.65 vs. 0.19), followed by Ni (8.8 vs. 2.3), to less extent for Mn (8.8 vs. 8.4) and minimum for Cd (0.55 vs. 0.57) and Pb (161 vs. 159). The present observation that contamination with Cd and Pb from the device is practically negligible (Table 3) is in agreement with Minoia et al. (1992). Takagi et al. (2009) also found minimum contamination of blood with Pb from the device. In case of Cr, the expected increment in Cr in blood as the worst case (as GM × GSD2) was 0.08 (Type 1) or 0.10 μg/l (Type 2), whereas observed Cr in blood was 0.55 μg/l as GM (Table 4). Thus about 20% increase may induced by contamination. Similar worst case estimation for Mn (i.e., 13.2 μg/l vs. 0.31 μg/l as observed GM in blood vs. GM × GSD2 of contamination) suggests that about 3% increment would be expected for Mn, the rate apparently acceptable for practical purpose. With this regard, no information is available for the devices used for blood collection in 2002, unfortunately. In case of 2008 collection, Type 2 and Type 1 vacuum tubes were employed in Prefecture 1 and Prefecture 5, respectively. Thus, it may be possible to estimate that (0.55–0.05) = 0.50 μg/l and (0.41–0.05) = 0.36 μg/l are true average Cr concentration in Prefecture 1 and 5, respectively.
The difficulty in ICP-MS measurement for low atomic weight metals (including Cr and Ni) has been pointed out by Nuttall et al. (1995) as ‘not amenable’. In practice, risk of interference was pointed out for 52Cr and for 60Ni in massive presence of 40Ar12C and 23Na37Cl, respectively, in the analyses of biological samples such as blood after wet digestion (Case et al. 2001). Thus, the difficulty encountered in the present study may be inherent to the principle of the analytical method and analytical conditions, as well as matrix for analysis, and the sector field technique could remove the problems only partly.
In Table 7, results of the present analysis on metal concentrations in blood of Japanese women were compared with the levels reported in literatures. With regard to Cd levels, the present GM level of 1.23 μg/l was higher than others except for 4.0 μg/l reported by Afridi et al. (2006) and 1.7 μg/l by Farzin et al. (2008). The high Cd levels in blood of Japanese populations (Ikeda et al. 1999; Zhang et al. 1999; the present study) are on line with high dietary intake of Cd among the populations, although lower values in the present survey when compared with the values published in 1999 also suggest gradual decrease in the dietary Cd intake as previously discussed (Ikeda et al. 2004). In contrast, Pb in blood of Japanese population, 15.8 μg/l, was substantially lower than the levels reported for other populations, i.e., 21.3 μg/l (Clark et al. 2007) to 180 μg/l (Afridi et al. 2006), possibly in refection of low Pb intake from both the atmospheric air through respiration and foods via ingestion (Ikeda et al. 2000a, b). The very low Pb value of 1.15 μg/l (Gao et al. 2008) should be due to the fact that plasma (and not whole blood) was analyzed whereas a majority (some 95%) of Pb in blood is bound to erythrocytes (Alessio and Foá 1983)
It was difficult to make comparative evaluation of the present observation on other three metals (separate from possible problem in analytical chemistry, which was not taken into account) because data were rather scarce on these metals. The Cr level, 0.55 μg/l, would probably be comparable to other values except for two extremely high values of 74.9 μg/l by Afridi et al. (2006) and 29 μg/l by Sathwara et al. (2007). The Mn level, 13.2 μg/l, may be somewhat higher than others except for 48.0 μg/l reported by Afridi et al. (2009), and the level of Ni, 1.83 μg/l, may probably be comparable to values reported by others (Table 7). Nevertheless, possible contamination with these metals from phlebotomy devices should also be considered as expressed above.
Two major limitations should be considered in evaluating present results. With regard to sample collection, selection of blood sample donors did not follow rigid sampling strategy (such as random sampling) but by chance, which was practically inevitable under present survey conditions. Furthermore, not all prefectures were studied (i.e., eight prefectures out of 47), and the number of samples for each prefecture was not in proportion to the size of population in each prefecture. Thus, the values obtained may be taken as an estimate for the national values. Technically, standard phlebotomy devices (i.e., vacuum tube and holder sets for clinical use) were employed for blood sampling in Prefectures 2–4 and 6–8 in 2002, as the samples were originally for evaluation of Cd determination and diagnosis of iron-deficiency anemia in relation to Cd body burden (Tsukahara et al. 2003). Thus, the possibility of blood contamination with Cr and Ni from the device used (Table 3, and Minoia et al. 1992) could not be ruled out. With regard to samples collected in Prefectures 1 and 5 in 2008, it was possible to estimate Cr and Ni concentrations in blood excluding contamination from the devices.
Despite such limitations, however, it is prudent to conclude that Cd concentrations for Japanese populations appeared to be higher than the levels reported for other populations, whereas Pb concentrations were lower than others. Due to limitation in availability of information, no meaningful comparison was possible for the levels of Cr, Mn and Ni.
References
Afridi HI, Kazi TG, Jamali MK, Kazi GH, Arain MB, Jalbani N, Shar GQ, Sarfaraz A (2006) Evaluation of toxic metals in biological samples (scalp hair, blood and urine) of steel mill workers by electrothermal atomic absorption spectrometry. Toxicol Ind Health 22:381–393
Afridi HI, Kazi TG, Kazi NG, Jamali MK, Arain MB, Sirajuddin Kandhro GA, Shah AQ, Baig JA (2009) Evaluation of arsenic, cobalt, copper and manganese in biological samples of steel mill workers by electrothermal atomic absorption spectrometry. Toxicol Ind Health 25:59–69
Alessio L, Foá V (1983) Lead. In: Alessio L, Berlin A, Roi R, Boni M (eds) Human biological monitoring of industrial chemicals series, vol. 1 joint research centre. Ispra Establishment, Ispra, Italy, pp 105–132
Al-Saleh I, Shinwari N, Mashhour A, Mohamed GE, Ghosh MA, Shammasi Z, Al-Nasser A (2006) Cadmium and mercury levels in Saudi women and its possible relationship with hypertension. Biol Trace Elem Res 12:13–29
Antoniou J, Zukor DJ, Mwale F, Minarik W, Petit A, Huk OL (2008) Metal ion levels in the blood of patients after hip resurfacing: a comparison between twenty-eight and thirty-six-millimeter-head metal-on-metal prostheses. J Bone Joint Surg 90(Suppl. 3):142–148
Apostoli P, Baj A, Bavazzano P, Ganzi A, Neri G, Ronchi A, Soleo L, Di Lorenzo L, Spinelli P, Valente T, Minoia C (2002) Blood lead reference values: the results of an Italian polycentric study. Sci Total Environ 287:1–11
Bader M, Dietz MC, Ihrig A, Tribig G (1999) Biomonitoring of manganese in blood, urine and axillary hair following low-dose exposure during the manufacture of dry ell batteries. Int Arch Occup Environ Health 72:521–527
Bazzi A, Nriagu JO, Lunder AM (2008) Determination of toxic and essential elements in children’s blood with inductively coupled plasma-mass spectrometry. J Environ Monit 10:1226–1232
Bulat ZP, Ðukić-Ćokić D, Dokić M, Bulat P, Matović V (2009) Blood and urine cadmium and bioelements profile in nickel-cadmium battery workers in Servia. Toxicol Ind Health 25:129–135
Case CP, Ellis L, Turner JC, Fairman B (2001) Development of routine method for the determination of trace metals in whole blood by magnetic sector inductively coupled plasma mass spectrometry with particular relevance to patients with total hip and knee arthroplasty. Clin Chem 47:275–280
Clark NA, Teschke K, Rideout K, Copes R (2007) Trace element levels in adults from the west coast of Canada and association with age, gender, diet, activities, and levels of other trace elements. Chemosphere 70:155–164
Coelho P, Silva S, Roma-Torres J, Costa C, Henriques A, Teixeira J, Gomes M, Mayan O (2007) Health impact of living near an abandoned mine—case study: Jales mines. Int J Hyg Environ Health 210:399–402
Ekong EB, Jaar BG, Weaver VM (2006) Lead-related nephrotoxicity: a review of the epidemiologic evidence. Kidney Int 70:2074–2084
Farzin L, Amiri M, Shams H, Faghih MAA, Moassesi ME (2008) Blood levels of lead, cadmium, and mercury in residents of Tehran. Biol Trace Elem Res 123:14–26
Gao S, Jin Y, Unverzagt FW, Ma F, Hall KS, Murrell JR, Cheng Y, Shen J, Ying B, Ji R, Matesan J, Liang C, Hendrie HC (2008) Trace element levels and cognitive function in rural elderly Chinese. J Gerontol 63A:635–641
Heitland P, Köster HD (2006) Biomonitoring of 37 trace elements in blood samples from inhabitants of northern Germany by ICP-MS. J Trace Elem Med Biol 20:253–262
Herber RF (1999) Review of trace element concentrations in biological specimens according to the TRACY protocol. Int Arch Occup Environ Health 72:279–283
Herber RFM, Christensen JM (1997) Critical evaluation and review of cadmium concentrations in blood for use in occupational health according to the TRACY protocol. Int Arch Occup Environ Health 69:372–378
Ikeda M, Zhang Z-W, Higashikawa K, Watanabe T, Shimbo S, Moon C-S, Nakatsuka H, Matsuda-Inoguchi N (1999) Background exposure of general women populations in Japan to cadmium in the environment and possible health effects. Toxicol Lett 108:161–166
Ikeda M, Zhang Z-W, Shimbo S, Watanabe T, Nakatsuka H, Moon C-S, Matsuda-Inoguchi N, Higashikawa K (2000a) Urban population exposure to lead and cadmium in east and south-east Asia. Sci Total Environ 249:373–384
Ikeda M, Zhang Z-W, Shimbo S, Watanabe T, Nakatsuka H, Moon C-S, Matsuda-Inoguchi N, Higashikawa K (2000b) Exposure of women in general populations to lead via food and air in east and southeast Asia. Am J Ind Med 38:271–280
Ikeda M, Ezaki T, Tsukahara T, Moriguchi J (2004) Dietary cadmium intake in polluted and non-polluted areas in Japan in the past and in the present. Int Arch Occup Environ Health 77:227–234
Ikeda M, Moriguchi J, Ezaki T, Fukui Y, Ukai H, Okamoto S, Shimbo S, Sakurai H (2005) Smoking-induced increase in urinary cadmium levels among Japanese women. Int Arch Occup Environ Health 78:533–540
Jusko TA, Henderson CR, Lanphear BP, Cory-Stechta DA, Parsons PJ, Canfield RL (2008) Blood lead concentrations < 10 μg/dl and child intelligence at 6 years of age. Environ Health Perspect 116:243–278
Kim Y-J, Kassab F, Berven SH, Zurakowski D, Hresko MT, Emans JB, Kasser JR (2005) Serum levels of nickel and chromium after instrumented posterior spinal arthrodesis. Spine 30:923–926
Kummrow F, Silva FF, Kuno R, Souza AL, Oliveira PV (2008) Biomonitoring method for the simultaneous determination of cadmium and lead in whole blood by electrothermal atomic absorption spectrometry for assessment of environmental exposure. Talanta 75:246–252
McKelvey W, Gwynn C, Jeffery N, Kass D, Thorpe LE, Garg RK, Palmer CD, Parsons P (2007) A biomonitoring study of lead, cadmium, and mercury in the blood of New York city adults. Environ Health Perspect 115:1435–1441
Micciolo R, Canal L, Maranelli G, Apostoli P (1994) Non-occupational lead exposure and hypertension in northern Italy. Int J Epidemiol 23:312–320
Mikeev MI (ed) (1996a) Biological monitoring of chemical exposure in the workplace, vol 1. World Health Organization, Geneva
Mikeev MI (ed) (1996b) Biological monitoring of chemical exposure in the workplace, vol 2. World Health Organization, Geneva
Minoia C, Pietra R, Sabbioni E, Ronchi A, Gatti A, Cavalleri A, Manzo L (1992) Trace element reference values in tissues from inhabitants of European Community. III. The control of pre analytical factors in the biomonitoring of trace elements in biological fluids. Sci Total Environ 120:63–79
Mizushima R, Yonezawa M, Ejima A, Koyama H, Satoh H (1996) Microwave digestion using dual PTFE containers for analysis of trace elements in small amounts of biological samples. Tohoku J Exp Med 178:75–79
Moriguchi J, Ezaki T, Tsukahara T, Fukui Y, Ukai H, Okamoto S, Shimbo S, Sakurai H, Ikeda M (2005) Effects of aging on cadmium and tubular dysfunction markers in urine from adult women in non-polluted areas. Int Arch Occup Environ Health 78:446–451
Muttamara S, Leong ST (2004) Health implication among occupational exposed workers in a chromium alloy factory, Thailand. J Environ Sci 16:181–186
Nuttall KL, Gordon WH, Ash KO (1995) Inductively coupled plasma mass spectrometry for trace element analysis in the clinical laboratory. Ann Clin Lab Sci 25:264–271
Polizzi S, Pira E, Ferrara M, Bugiani M, Papaleo A, Albera R, Palmi S (2002) Neurotoxic effects of aluminium among foundry workers and Alzheimer’s disease. NeuroToxicology 23:761–774
Rodushkin I, Ödman F, Branth S (1999) Multielement analysis of whole blood by high resolution inductively coupled plasma mass spectrometry. Fresenius J Anal Chem 364:338–346
Sathwara NG, Patel KG, Vyas JB, Patel S, Trivedi MR, Dave LM, Madia MM, Kulkarni PK, Parikh DJ, Saiyed HN (2007) Chromium exposure study in chemical based industry. J Environ Biol 28:405–408
Schermaier AJ, O’Conner LH, Pearson KH (1985) Semi-automated determination of chromium in whole blood and serum by Zeeman electrothermal atomic absorption spectrophotometry. Clin Chim Acta 152:123–134
Schramel S, Wendler I, Angerer J (1997) The determination of metals (antimony, bismuth, lead, cadmium, mercury, palladium, platinum, tellurium, thallium, tin and tungsten) in urine samples by inductively coupled plasma-mass spectrometry. Int Arch Occup Environ Health 69:219–223
Sugita M, Tsuchiya K (1995) Estimation of variation among individuals of biological half-times of cadmium calculated from accumulation data. Environ Res 68:31–37
Takagi M, Tamiya S, Yoshinaga J, Kaji M (2009) Lead in blood of Japanese children; analytical conditions. Jpn J Hyg 64:403 (in Japanese)
Tsukahara T, Ezaki T, Moriguchi J, Furuki K, Fukui Y, Ukai H, Okamoto S, Sakurai H, Ikeda M (2003) No significant effect of iron deficiency on cadmium body burden or kidney dysfunction among women in the general population in Japan. Int Arch Occup Environ Health 76:275–281
Vitayavirasuk B, Junhom S, Tantisaeranee P (2005) Exposure to lead, cadmium and chromium among spray painters in automobile body repair shops. J Occup Health 47:518–522
Watanabe T, Koizumi A, Fujita H, Kumai M, Ikeda M (1983) Cadmium levels in the blood of inhabitants in nonpolluted areas in Japan with special references to aging and smoking. Environ Res 31:472–483
Watanabe T, Fujita H, Koizumi A, Chiba K, Miyasaka M, Ikeda M (1985) Baseline level of blood lead concentration among Japanese farmers. Arch Environ Health 40:170–176
White MA (1999) A comparison of inductively coupled plasma mass spectrometry with electrothermal atomic absorption spectrometry for determination of trace elements in blood and urine from non occupationally exposed populations. J Trace Elements Med Biol 13:93–101
Zhang Z-W, Shimbo S, Ochi N, Eguchi M, Watanabe T, Moon C-S, Ikeda M (1997) Determination of lead and cadmium in food and blood by inductively coupled plasma mass spectrometry: a comparison with graphite furnace atomic absorption spectrometry. Sci Total Environ 205:179–187
Zhang Z-W, Qu J-B, Watanabe T, Shimbo S, Moon C-S, Ikeda M (1999) Exposure of citizens in China and in Japan to lead and cadmium; a comparative study. Toxicol Lett 108:167–172
Acknowledgments
This study was supported by Grants-in-Aid from Food Safety Commission, Japan (No. 0802; Head Investigator, M. Ikeda), for the fiscal years of 2008 and 2009. ICP-SF-MS analyses for metals were conducted by Inorganic Analysis Laboratories, Toray Research Center, Inc., Ohtsu, Shiga, Japan. Thanks are due to Hirosaki City Medical Association (Hirosaki, Japan) and Fukui Health Service Association (Fukui, Japan) for their cooperation in collecting blood samples, and Kyoto University Human Specimen Bank (Organizer; Professor A. Koizumi) for their generous supply of blood samples. The authors are grateful to the administration and staff of Kyoto Industrial Health Association (Kyoto, Japan) for their interest in and support to this study.
Conflict of interest statement
The authors declare that they have no conflict of interests.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ikeda, M., Ohashi, F., Fukui, Y. et al. Cadmium, chromium, lead, manganese and nickel concentrations in blood of women in non-polluted areas in Japan, as determined by inductively coupled plasma-sector field-mass spectrometry. Int Arch Occup Environ Health 84, 139–150 (2011). https://doi.org/10.1007/s00420-010-0542-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00420-010-0542-2