
Abstract
Pregnancy is a state of oxidative stress arising from increased placental mitochondrial activity and production of reactive oxygen species (ROS), mainly superoxide anion. The placenta also produces other ROS including nitric oxide, carbon monoxide, and peroxynitrite which have pronounced effects on placental function including trophoblast proliferation and differentiation and vascular reactivity. Excessive production of ROS may occur at certain windows in placental development and in pathologic pregnancies, such as those complicated by preeclampsia and/or IUGR, overpowering antioxidant defenses with deleterious outcome. In the first trimester, establishment of blood flow into the intervillous space is associated with a burst of oxidative stress. The inability to mount an effective antioxidant defense against this results in early pregnancy loss. In late gestation increased oxidative stress is seen in pregnancies complicated by diabetes, IUGR, and preeclampsia in association with increased trophoblast apoptosis and deportation and altered placental vascular reactivity. Evidence for this oxidative stress includes increased lipid peroxides and isoprostanes and decreased expression and activity of antioxidants. The interaction of nitric oxide and superoxide produces peroxynitrite, a powerful prooxidant with diverse deleterious effects including nitration of tyrosine residues on proteins thus altering function. Nitrative stress, subsequent to oxidative stress is seen in the placenta in preeclampsia and diabetes in association with altered placental function.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Oxidative stress is described as an imbalance in the production of reactive oxygen species (ROS) and the ability of antioxidant defenses to scavenge them. It can arise from increased production of ROS and/or a decrease in antioxidant capacity. These ROS are free radicals and they induce cellular damage by acting on proteins and lipids. Pregnancy per se is a state of oxidative stress (Wisdom et al. 1991) arising from the increased metabolic activity in placental mitochondria and reduced scavenging power of antioxidants. Oxidative stress has been clearly shown in placental tissue. However, in certain pathologic pregnancies, i.e., those complicated by maternal diabetes, preeclampsia, or early pregnancy loss, a heightened level of oxidative stress is encountered. This increased oxidative stress can then affect placental function. This review will describe the determinants of oxidative stress in the placenta, review the evidence for increased oxidative stress in pathologic pregnancies, and discuss the functional consequences.
Generation of ROS in the placenta
The most common ROS is the superoxide anion (O2.−) formed as the first step in the one-electron reduction of molecular oxygen. Superoxide is generated in living cells by NADPH oxidase, xanthine oxidase, flavin enzymes, and enzymes in the mitochondrial electron transport chain (METC). The reactivity due to the unpaired electron in superoxide then leads to the production of other ROS including the hydroxyl radical and hydrogen peroxide. Reactive oxygen species are recognized to be signal transduction agents in addition to their well-defined roles in combating pathogens. Superoxide can also be generated under certain conditions by enzymatic pathways that produce other ROS including nitric oxide and carbon monoxide which have vasoactive effects in the placenta but are also realized to have roles in signal transduction. The pathways leading to the production of these ROS are described in more detail below.
Enzymatic pathways
Mitochondrial electron transport chain
The mitochondria are responsible for consumption of the majority of oxygen and ATP generation. It has been estimated that about 2–3% of all electrons in the METC leak out of the mitochondria, estimated to produce 160–320 mmol superoxide per day by a 60 kg woman (Chance et al. 1979). Although METC complex III was considered as the major ROS generation site (Chen et al. 2003), Kudin et al. (2004) found that inhibition of complex I resulted in a greater Vmax for H2O2 generation (0.68 nmol/min per mg with rotenone, a complex I inhibitor, vs 0.14 nmol/min per mg with antimycin A, a complex III inhibitor) in isolated rat and human brain mitochondria. Inhibition of METC complex I with rotenone caused apoptosis in HL60, a leukemia cell, and in HT1080, a fibrosarcoma cell, via ROS generation showing a functional effect of superoxide generation (Li et al. 2003). Similarly, hypoxia may cause halting of complete mitochondrial oxygen reduction thus generating superoxide. Hypoxia may alter METC complex I in lung epithelial cells (Li et al. 2002), and in cultured pulmonary artery myocytes, hypoxia-induced ROS generation was attenuated by an inhibitor of METC complex I. This may explain the apparent paradox of hypoxia-induced oxidative stress. In addition, ROS seem to act as second messengers for oxygen sensing in the mitochondria since antioxidants abolished hypoxic pulmonary vasoconstriction without affecting contraction to U46619, and the hypoxic response was absent in cells that were depleted of METC (Waypa et al. 2001). The participation of METC in early pregnancy is not clear. However, mitochondrial mass in the placenta increases both with gestational age, suggesting increased contribution of METC to ROS generation, and in placental pathologies such as preeclampsia whereby a hampered oxygen sensing was suggested (Wang and Walsh 1998).
Xanthine oxidoreductase
Xanthine oxidoreductase exists in two functionally distinct forms. Under normal conditions, the larger part of the enzyme occurs as an NAD(+)-dependent dehydrogenase form (XDH) which converts hypoxanthine to xanthine with reduction of NAD to NADH. The dehydrogenase can be transformed under various pathophysiological conditions, i.e., hypoxia or cytokine stimulation, to an oxygen-dependent oxidase form (XO). Xanthine oxidase then catalyses the oxidation of xanthine to uric acid, with accompanying superoxide production. Hypoxia has been shown to upregulate expression of XO (Hassoun et al. 1994). However, studies in bovine pulmonary vascular endothelial cells showed that XO was quickly inactivated by in vitro and in vivo reoxygenation (Terada et al. 1988; Partridge et al. 1992), suggesting XO may serve as an initial source but not a prolonged source of ROS generation. This may have implications during early pregnancy (see later).
Xanthine oxidase was first described in villous trophoblast, stroma and endothelial cells by Many et al. (1996) with a modest increase in expression seen throughout gestation. Increased expression of XO mRNA in villous endothelial cells and extravillous trophoblast accompanied by decreased superoxide dismutase (SOD) expression in the same cells, was subsequently described in preeclamptic women (Many et al. 1996, 2000). However, XO activity was reportedly absent in fresh human placenta (Wajner and Harkness 1989). Therefore, the involvement of XO in generation of placental oxidative stress is not confirmed. Furthermore, placental transport of uric acid and hypoxanthine, the substrate of XDH, are very limited (van Kreel and van Dijk 1977) suggesting XO may only be a minor generator of superoxide in the placenta.
NADPH oxidase
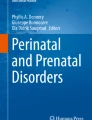
The enzyme NADPH oxidase is capable of generating large amounts of ROS in neutrophils, macrophages, and monocytes (Babior et al. 2002). This phagocytic isoform is a multimeric enzyme consisting of five unique peptides, p22phox, p47phox, p67phox, Rac, and gp91phox. Under appropriate stimulation these subunits assemble at the cell membrane. A flavocytochrome consisting of two membrane-bound peptides of 22 and 91 kDa (p22phox and gp91phox or Nox2, respectively) makes up the redox pathway, and contains binding sites for NADPH, flavin, and heme. The placental macrophage, the Hofbauer cell, has been shown to express subunits of this phagocytic NADPH oxidase (Myatt et al. unpublished data; Fig. 1).

Expression of Nox2 in human villous tissue. Frozen term villous tissue was immunostained with anti-cytochrome b558 antisera (left panel) or with the absence of primary antibody (right panel) using the Vectastain ABC kit. Magnification ×400
An oxidase activity was detected and was confined to the microvillous membrane of syncytiotrophoblast with non-specific cytochemical methods (Matsubara and Sato 2001). More recently, Manes (2001) isolated a protein consisting of a 58- and a 33-kDa subunit from term placenta, presumably from syncytiotrophoblast. In vitro, this placental NADPH oxidase is constitutively active and differs from that of phagocytes in several biochemical properties suggesting another isoform exists in placenta. Recently, several homologues of human gp91phox subunit have been identified in somatic cell types by molecular cloning (Table 1). The products are characterized by five to six transmembrane domains with a highly homologous C-terminus NADPH/FAD binding region. Although the physiological function of the non-phagocytic Nox genes remains largely unknown, some of these novel Nox isoforms have been shown to generate ROS in reoxygenation models (Caraceni et al. 1995; Zulueta et al. 1995; Souren et al. 1997; Al-Mehdi et al. 1998; Spranger et al. 1998; De Deken et al. 2000). Vascular endothelial growth factor (VEGF) mRNA, VEGF receptors, and metalloproteinase activity were markedly increased in Nox1-expressing cells (Arbiser et al. 2002). It has also been found that Nox5 induces apoptosis in prostate epithelial cells (Brar et al. 2003). These novel NADPH oxidase enzymes are possibly involved in the pathophysiology of atherosclerosis and hypertension and can be stimulated by ligands, such as angiotensin II, PDGF, cytokines, and thrombin, changes in hemodynamic forces, and cellular metabolism (Griendling et al. 2000) to produce superoxide.
Our laboratory has recently identified two Nox isoforms, Nox1 and Nox5, in cytotrophoblasts isolated from term human placenta (Cui et al. unpublished observations). Employing anti-Nox1 and anti-Nox5 peptide antisera, we observed specific staining in syncytiotrophoblast and villous vascular endothelial cells by immunohistochemistry (Fig. 2). We postulate that these novel Nox enzymes may play an important role in both ROS generation and oxygen sensing.

Expression of Nox1 and Nox5 in human villous tissue. Frozen villous tissue sections were immunostained using polyclonal antibodies specific for Nox1 or Nox5 (right panels). Preimmune sera was used as immunologic control (left panels)
Nitric oxide synthase
Nitric oxide is an active vasodilator in the fetal placental vasculature (Myatt et al. 1991) where it maintains basal vascular tone and attenuates the action of vasoconstrictors. However, it may fulfill other roles such as anti-adhesive and anti-aggregatory roles in syncytiotrophoblast, immunomodulatory roles in Hofbauer cells, together with being a signal transduction agent. We first described that the type III or endothelial nitric oxide synthase (eNOS) isoform was immunolocalized to villous vascular endothelium and syncytiotrophoblast (Eis et al. 1995). In vitro expression of eNOS increased in syncytiotrophoblast as they differentiated from cytotrophoblast (Eis et al. 1995). In contrast type II or inducible NOS is expressed in Hofbauer cells (Myatt et al. 1997b). It is controversial whether eNOS is expressed in extravillous trophoblast cells where it may play a role in regulation of trophoblast invasion (Eis et al. 1995; Martin and Conrad 2000; Lyall 2003). We have found that expression of eNOS was increased in vascular endothelium with preeclampsia (Myatt et al. 1997a) perhaps as a compensatory response to vasoconstriction-induced increased shear stress across endothelial cells seen in these placentas. In conjunction with superoxide generation from NADPH oxidase by the same cells, this may lead to increased formation of the powerful prooxidant peroxynitrite (ONOO.) which nitrates tyrosine residues on proteins thus covalently modifying protein function (Beckman and Koppenol 1996).
Heme oxygenase
Carbon monoxide is a vasodilator in the placenta (Lyall et al. 2000) and is synthesized by the enzyme heme oxygenase (HO). There is little of the HO-1 isoform in the placenta (Lyall et al. 2000; McLean et al. 2000; Yoshiki et al. 2000; Barber et al. 2001) whereas HO-2 is found in vascular endothelium and villous and extravillous trophoblast. A reduction in HO-2 expression was found in endothelial cells in preeclampsia (Barber et al. 2001).
Formation of peroxynitrite
Nitric oxide is inactivated by superoxide anion (Moncada et al. 1991) which, therefore, limits its bioactivity. Conversely, the activity of nitric oxide is prolonged by the presence of SOD which removes superoxide. The action of superoxide per se is limited by its low lipid solubility, limited membrane transport, and by its removal by SOD. However, when tissues are induced to simultaneously produce both nitric oxide and superoxide in a concentrated and localized manner by inflammatory stimuli, sepsis, and ischemia/reperfusion, nitric oxide and superoxide react to produce peroxynitrite, a potent long-lived oxidant at a diffusion-limited rate constant. Peroxynitrite anion (ONOO−) is a powerful oxidant of a variety of biomolecules (Beckman et al. 1990) and is cytotoxic as it inhibits mitochondrial electron transport resulting in inhibition of cellular respiration (Radi et al. 1994), oxidizes sulfhydryl groups in proteins, initiates lipid peroxidation without the requirement for transition metals (Radi et al. 1991), and nitrates aromatic amino acids such as tyrosine (Ischiropoulos et al. 1992), thus affecting many signal transduction pathways. Peroxynitrite can also increase DNA breaks which can lead to initiation of a futile DNA repair cycle by activation of poly (ADP-ribose) polymerase, resulting in depletion of cellular NAD+ and ATP stores (Zhang et al. 1994). In the isolated perfused rat heart, peroxynitrite impairs relaxation (Villa et al. 1994) and it causes vascular dysfunction in rats by selective impairment of adrenoreceptors when given systemically (Benkusky et al. 1999). Peroxynitrite production can be indirectly localized by the presence of nitrotyrosine residues (Beckman et al. 1994). Nitrotyrosine residues have been demonstrated in human atherosclerotic plaques (Beckman et al. 1994) and in lung sections of patients and animals with acute lung injury (Haddad et al. 1994) indicating areas of cellular damage including vascular damage. Ischemia-reperfusion causes increased formation of nitrotyrosine in cardiac tissue and inhibition of NOS enzyme reduces both the level of protein nitration and reperfusion injury (Wang and Zweier 1996; Liu et al. 1997; Zweier et al. 2001; Baker et al. 2002) which supports the role both of nitric oxide and protein tyrosine nitration.
When immunostaining placental tissues from pregnancies complicated by preeclampsia we found increased nitrotyrosine residues in the placenta, especially in the vascular endothelium when compared to normotensive pregnancies (Myatt et al. 1996). Later extension of these studies to pregestational diabetes showed abundant nitrotyrosine immunostaining in the vascular endothelium and villous stroma (Fig. 3) when compared to control patients (Lyall et al. 1998). Thus, we have evidence that the oxidative stress of pregnancies complicated by preeclampsia or pregestational diabetes is associated with generation and action of peroxynitrite as assessed by nitrotyrosine immunostaining.

Expression of nitrotyrosine residues in villous tissue of normal and diabetic pregnancies. Frozen sections from normal term (A, B) or diabetic (C, D) pregnancies were immunostained with a monoclonal anti-nitrotyrosine antibody using the Vectastain ABC kit. Control incubations (B, D) contained no primary antibody. Magnification ×125
Antioxidants in the placenta
All the major antioxidant systems including Mn and Cu/ZnSOD, catalase, glutathione, glutathione peroxidase, glutathione S-transferase, thiol/disulfide oxidoreductase, and vitamins C and E are present in the placenta. We find that the two SOD isoforms show cell-specific expression patterns in the placenta (Fig. 4). The mitochondrial MnSOD isoform is faintly expressed in syncytiotrophoblast but very intensely in villous vascular endothelium whereas the cytosolic Cu/ZnSOD isoform is intensely expressed in villous stroma, probably in the Hofbauer cell but only faintly in trophoblast (Myatt et al. 1997c). There is evidence for regional differences in the expression of antioxidant enzymes in the placenta perhaps in relation to the degree of oxygenation (Hempstock et al. 2003a) with the central region being well-oxygenated compared to the periphery, owing to the direction of maternal blood flow. However, central villi are morphologically and enzymatically immature compared to peripheral villi. Activity of catalase and glutathione peroxidase was higher in central than peripheral villi, but no difference was detected for total SOD. Also the mRNA concentration was higher in the center for catalase and for glutathione peroxidase but no differences were found for Cu/ZnSOD or MnSOD. Thus, it appears that the activities of catalase and glutathione peroxidase may reflect gradients established by the pattern of maternal intralobular blood flow, and that oxygen tension may be a regulatory factor in vitro (Hempstock et al. 2003a).

Expression of manganese (MnSOD) and copper/zinc (Cu/ZnSOD) superoxide dismutase isoforms in villous tissue. Serial sections of frozen term villous tissue were immunostained using polyclonal MnSOD or monoclonal Cu/ZnSOD antibodies with the Vectastain ABC kit. Control sections omitted the primary antibody. Magnification ×250
Evidence for oxidative stress in normal and pathologic pregnancies
Oxidative stress in early pregnancy
The placenta receives oxygenation from the maternal circulation and is positioned in an oxygen gradient between the mother and fetus. The placenta and fetus exist in a hypoxic environment during early pregnancy as the intrauterine oxygen tension is extremely low (pO2<20 mmHg, ~5% O2) at 8 weeks, (Jauniaux et al. 2000) prior to establishment of blood flow into the intervillous space. The placenta and fetus depend at this time on histiotrophic nutrition. However, the O2 tension rises steeply at the end of first trimester when the invasion of trophoblast allows the occluded uterine spiral arteries to open and the pO2 in the intervillous space reaches 50 mmHg (Jauniaux et al. 2000). The hypoxia/reoxygenation at this time imposes an ischemia-reperfusion insult. Therefore, the placenta is subjected to hypoxia and then hypoxia/reoxygenation in the first trimester of gestation.
In early pregnancy this increase in O2 tension is associated with increase in mRNA of the antioxidant enzymes catalase, glutathione peroxidase, and SOD within placental tissues. The reperfusion of placenta between 8 and 9 weeks may be responsible for expression of heat shock protein (HSP) 70 and formation of nitrotyrosine residues (markers for oxidative stress) in syncytiotrophoblast (Jauniaux et al. 2000). The magnitude of oxidative stress may depend on both the severity of the insult and on the effectiveness of the placental antioxidant defenses. The cytotrophoblast begins to synthesize SOD by 11 weeks, while syncytiotrophoblast SOD increases by 16 weeks. This may explain why first trimester cytotrophoblast survives better in low pO2 in culture and displays a better defense to pO2 increase in second trimester (Watson et al. 1998). Similarly, syncytiotrophoblast and mitochondrial morphology improved, and mitochondrial activity was retained for 6 h and more if 8- to 10-week-old tissue was placed into a low oxygen environment immediately after removal from the uterus.
Burton’s group also established an in vitro model using term placental tissues that recapitulated the ischemia/reperfusion seen in early pregnancy and also purported to occur in preeclampsia. Rapid generation of ROS was detected by fluorescent dye in different placental cell types with an intensity of villous endothelium >syncytiotrophoblast >stromal cells. Concomitantly, increased concentrations of HSP72, nitrotyrosine, and 4-HNE (markers of oxidative stress) were seen in placental endothelial and smooth muscle cells and syncytiotrophoblast (Hung et al. 2001). Preloading placental tissues with ROS scavengers desferrioxamine and α-phenyl-N-tert-butylnitrone reduced the level of oxidative stress seen. These data show the ability of placental tissues to generate ROS and the necessity for adequate antioxidants to scavenge them.
Oxidative stress and miscarriage
Using Doppler ultrasonography Jauniaux et al. (2003) showed that onset of intervillous blood flow increased with gestational age, being detected in 9 of 25 cases at 8–9 weeks but in 18 of 20 cases at 12–13 weeks. However, in abnormal pregnancies, which end in fetal demise, flow was detected in nearly all cases at 8–9 weeks and regional differences in flow to the placenta were observed between the normal and abnormal pregnancies. Early flow was restricted to the peripheral regions of most normal placentas but was most common in central regions or throughout the placenta in missed miscarriages. In comparison, immunoreactivity for HSP70 and nitrotyrosine residues (markers of oxidative stress) was greater in samples from peripheral than from central regions of normal placentas and from missed miscarriages compared to controls. The data suggest that oxidative damage to the trophoblast, induced by premature and widespread onset of the maternal placental circulation, is a key factor in early pregnancy loss (Jauniaux et al. 2003).
This group also determined if the disorganized and early onset of the maternal blood flow to the placenta seen in miscarriage was associated with excessive levels of oxidative damage and stress in placental tissues (Hempstock et al. 2003b). Indeed morphological and immunohistochemical markers of cellular stress and damage, including HSP70, nitrotyrosine residues, and lipid peroxidation, were increased in tissues obtained from missed miscarriages compared with controls particularly those with gestation shorter than 77 days and with evidence of recent fetal demise. Increased apoptosis and decreased numbers of mitotic cells were seen indicating that oxidative stress overwhelms cellular antioxidant defense systems. These data reinforce the concept that placental oxidative stress with resultant damage to the syncytiotrophoblast, secondary to early onset of the maternal circulation, may be a mechanism contributing to early fetal loss (Hempstock et al. 2003b).
Oxidative stress in preeclampsia
Preeclampsia is the clinical syndrome of edema, hypertension, and proteinuria in the pregnant woman and occurs primarily in nulliparous women in their third trimester. Approximately 7% of pregnancies in the United States are affected by preeclampsia which is the leading cause of fetal growth restriction, indicated premature delivery, and maternal death. The underlying maternal pathophysiology involves generalized arteriolar constriction and intravascular depletion that can produce symptoms related to ischemia, necrosis, and hemorrhage of organs resulting in poor perfusion of the maternal and fetal circulations of the placenta leading to abnormal fetal growth and development. Shallow trophoblast invasion is the major pathologic finding in the preeclamptic placenta, particularly those that are early-onset. Since maximal placental trophoblast invasion occurs at the end of the first trimester when pO2 increases sharply, a developmental failure of oxygen handling by trophoblast has been suggested in preeclampsia. In addition, hypoxia-reoxygenation has been shown to cause apoptosis in many cells, and an increased deportation of trophoblast fragments secondary to increased apoptosis in the syncytiotrophoblast is observed in preeclampsia (Allaire et al. 2000; Redman and Sargent 2000; Leung et al. 2001; Ishihara et al. 2002).
Exposure of the mother to the shed placental trophoblast may be responsible for onset of systemic inflammation in the mother. Maternal leukocytes from preeclamptic individuals were hyperactive in regard to constitutive and cytokine-induced ROS generation as compared to normal subjects (Gervasi et al. 2001; Lee et al. 2003). A significant increase of neutrophil-endothelial adhesion and adhesion molecules expression is seen in neutrophils exposed to conditioned medium derived from preeclamptic placental villous culture compared to normal placental culture (Wang et al. 2001). Sera obtained from patients with severe preeclampsia stimulated isolated healthy neutrophils significantly more than sera from normal subjects (Zusterzeel et al. 2001b). In addition, neutrophils are stimulated by shed syncytiotrophoblast microvillous membranes to generate ROS in women with preeclampsia (Aly et al. 2004). Tumor necrosis factor α (TNFα), a cytokine produced mainly by macrophages, was abnormally increased in preeclamptic placentas (Conrad et al. 1998) perhaps in response to hypoxia. TNFα might contribute to the increased oxidative stress by induction of oxygen free radicals (Wang and Walsh 1996b).
An agonistic autoimmune antibody to angiotensin II type 1 receptor has been reported to develop in preeclampsia patients which triggers receptor-mediated NADPH oxidase activation in the placenta (Dechend et al. 2003). Therefore, NADPH oxidase might be responsible for generating and/or sensing the oxidative stress and might be abnormally regulated in preeclamptic pregnancies. However, employing cerium as a capturing agent for enzymatic histochemistry, Matsubara and Sato (2001) did not find differences in distribution pattern and NADPH oxidase enzyme intensities among normal, preeclamptic, and IUGR placentas. Currently our laboratory is using specific antibodies to NADPH oxidase isoforms to map differences in expression.
In preeclamptic patients there is increased placental oxidative potential. Increased superoxide generation was observed employing a direct electron paramagnetic spin trap resonance technique (Sikkema et al. 2001). Wang and Walsh (1998) have reported that the amount of mitochondrial protein is 47% greater and the activity of the mitochondrial enzyme, citrate synthase, 56% greater in the preeclamptic placenta as compared to normal placentas, indicating an increase in the mitochondria number. These investigators also observed much higher lipid peroxide generation from preeclamptic mitochondria. However, Matsubara et al. (1997) found that mitochondrial cytochrome c oxidase activity was significantly decreased in trophoblast from preeclampsia. This may have resulted from prolonged hypoxia which has been shown to inhibit cytochrome c activity in isolated rat hepatocytes mitochondria (Chandel et al. 1995). However, these observations suggest that the increased amount of mitochondria may be a compensatory response, and that trophoblast cell mitochondrial dysfunction could be associated with preeclampsia.
Lipid peroxide formation, a marker of oxidative stress, is increased during pregnancy and preeclampsia (Casasco et al. 1997; Morris et al. 1998; Wang and Walsh 1998; Mutlu-Turkoglu et al. 1999). These lipid peroxides are produced mainly in the placenta due to membrane disruption by ROS. Microvillous membrane lipid peroxide concentration can be quantitated as malondialdehyde (MDA) in syncytiotrophoblast plasma membranes. A twofold increase of MDA along with increased arachidonic acid content was observed in preeclamptic women as compared to healthy subjects (Cester et al. 1994). Higher concentrations of MDA were found in the culture media of placental explants from preeclampsia patients, a finding recapitulated by culture of normal tissue in media containing XO/xanthine (Walsh et al. 2000). Concentrations of the isoprostane 8-iso-PGF2α, a specific marker for oxidative stress, are also seen in the preeclamptic placenta (Walsh et al. 2000).
Placental and decidual protein carbonyl levels (biomarkers for ROS-mediated protein damage) were higher in preeclampsia with HELLP than in normal pregnancy, whereas FRAP levels (a marker for antioxidant capacity) were lower (Zusterzeel et al. 2001a). The level of protein thiol/disulfide oxidoreductases (thioredoxin, glutaredoxin, and protein disulfide isomerase) were increased two- to threefold in preeclampsia placenta, indicating an adaptive protection against oxidative stress in trophoblast (Shibata et al. 2001). As an indirect indication of excessive ROS generation, nitrotyrosine content is increased in placental villous vessel endothelium in preeclampsia (Myatt et al. 1996; Adams et al. 2000).
Often there is upregulation of antioxidant defenses in response to oxidative stress but persistent overwhelming oxidative stress leads to consumption and depression of antioxidants. Thus increased glutathione levels (Knapen et al. 1999) and increased glutathione peroxidase (Knapen et al. 1999) and catalase (Wang and Walsh 1996a) activities have been described in the placenta in preeclampsia. In contrast decreased mRNA expression and activity of Cu/ZnSOD (Wang and Walsh 2001), SOD, glutathione, and glutathione peroxidase (Wang and Walsh 1996a) have been reported together with reduced glutathione S-transferase (Zusterzeel et al. 1999) but no change in vitamin E (Poranen et al. 1998). The magnitude of oxidative stress and antioxidant changes correlate well with diastolic blood pressure (Madazli et al. 2002). However, no differences in localization or intensity of SOD isoforms were found between normal or preeclampsia tissues (Myatt et al. 1997c). Overall the severity of preeclampsia correlates with loss of antioxidant power.
Together these data suggest a loss of the balance in preeclampsia between ROS production and antioxidant scavenging capacity which is maintained under normal physiological conditions in the placenta. However, while we have appreciable data on oxidative stress and expression of antioxidant enzymes there is as yet no clear picture identifying the enzymes that are responsible for ROS generation and the site of these enzymes.
Oxidative stress in diabetic pregnancy
Diabetes during pregnancy encompasses a range of disease entities including gestational diabetes and overt diabetes mellitus. True gestational diabetes mellitus is an impairment in carbohydrate metabolism that first manifests during pregnancy. Pregestational diabetes mellitus complicates 0.25% of pregnancies, and, despite improvements in perinatal care over the last several decades, there still exists significant morbidity and mortality particularly in cases of poorly controlled glucose homeostasis (Garner et al. 1990). Like preeclampsia, diabetes is also characterized as a state of endothelial dysfunction and reactive nitrogen and oxygen species contribute to the progression of diabetes (Honing et al. 1998; Rosen et al. 2001). Women who are diabetic have a four times greater rate of development of preeclampsia suggesting their preexisting endothelial dysfunction may predispose them to preeclampsia. In diabetes, ROS including superoxide are thought to be produced as a result of prolonged periods of exposure to hyperglycemia, which is known to cause non-enzymatic glycation of plasma proteins (Tames et al. 1992). This superoxide, in the absence of appropriate levels of scavengers, may lead to an imbalance between prooxidants and antioxidants and produce a state of oxidative stress.
We determined the presence and level of expression of nitrotyrosine residues in placental villous tissue of diabetic pregnancies as an index of vascular damage linked to oxidative stress (Lyall et al. 1998). Villous tissue was collected from ten White Class C and D pregestational diabetic patients and ten normotensive controls matched for gestational age. Serial sections of tissue were immunostained for nitrotyrosine, eNOS, and MnSOD. All tissues demonstrated immunostaining for eNOS in both syncytiotrophoblast and stem villous vascular endothelium with no apparent differences between groups. Significantly more intense nitrotyrosine staining was apparent in vascular endothelium and villous stroma of diabetic placentas (Fig. 3). The endothelium of large villous vessels of diabetic tissues also showed more intense immunostaining for MnSOD (Fig. 5). In these diabetic pregnancies, we were unable to show increased eNOS, unlike previous findings in preeclamptic pregnancies. The presence of nitrotyrosine may indicate vascular damage in the diabetic placenta due to peroxynitrite action formed from increased synthesis/interaction of nitric oxide and superoxide. The apparently paradoxical increase in MnSOD expression may be an adaptive response to increased superoxide generation.

Expression of MnSOD in villous tissue of normal and diabetic pregnancies. Frozen sections from normal term (A, B) or diabetic (C, D) pregnancies were immunostained with a polyclonal anti-MnSOD antibody using the Vectastain ABC kit. Control incubations (B, D) contained no primary antibody. Magnification ×125
Functional consequences of oxidative stress in placental physiology
Trophoblast proliferation, invasion and migration, fusion and apoptosis, are processes required for normal embryo plantation and placental angiogenesis which eventually determine fetus growth (Fig. 6). However, whether and how these cellular events are linked and regulated remains largely unknown. Changes in pO2 trigger several differentiation processes, including erythropoiesis and vasculogenesis/angiogenesis. Such processes are often medicated by oxygen-regulated expression of hormones or growth factors. Hypoxia-induced factor is a transcription factor that plays a central role in induction of VEGF, TGF, and erythropoietin.

Pathways of trophoblast proliferation and differentiation
Trophoblast fusion/differentiation
In vitro, isolated cytotrophoblasts aggregate and fuse to form a syncytium, a process associated with disappearance of several cellular markers (for example, desmoplakin) while hCG secretion increases. Exposure to 9% O2 impairs cell fusion and differentiation since desmoplakin and E-cadherin persist and a 70% decrease of hCG secretion was observed, suggesting cytotrophoblast aggregation without fusion (Alsat et al. 1996). Impaired fusion and differentiation were also observed following overexpression of Cu/ZnSOD, a gene product of chromosome 21, in cytotrophoblasts (Frendo et al. 2001). Interestingly, higher levels of Cu/ZnSOD mRNA, protein, as well as enzymatic activity were observed in trisomy 21-affected placentas, where there is a defect in syncytiotrophoblast formation and a decrease in the production of pregnancy-specific hormones. Choriocarcinoma cells have been widely employed as a convenient approach to mimic trophoblast cellular events. BeWo, JEG-3, and JAR cells may be induced to fuse and differentiate in vitro (Wice et al. 1990; Vaughan and Walsh 2002; Kudo et al. 2003). Forskolin-induced BeWo cell fusion (determined by a quantitative flow cytometry assay) was reversibly suppressed in 2% oxygen compared to 20% oxygen. This was associated with suppressed secretion of hCG (Kudo et al. 2003). In addition, H2O2 dose-dependently decreases hCG secretion in JEG-3 (McAleer and Tuan 2001).
Trophoblast proliferation
Hypoxia, however, has been shown to promote cytotrophoblast and extravillous trophoblast proliferation (Caniggia et al. 2000). Huppertz et al. (2003) observed that the proliferation rate of cytotrophoblast was decreased when exposed to higher pO2. Recently, Fisher’s group has employed proteomics to analyze protein expression of first trimester cytotrophoblast and observed a twofold decrease of MnSOD and a threefold decrease of 1-Cys peroxiredoxin, both antioxidant enzymes, when cells were exposed to extreme hypoxia (2% O2; Hoang et al. 2001). Since hypoxia changes the differentiation property of the first trimester cytotrophoblast to proliferation (Genbacev et al. 1996, 1997), these results reinforce the existence of oxidative stress in early placenta which potentiates cell proliferation.
Oxidative stress and trophoblast apoptosis
Although morphological measurements of placental constituents and the villous surface area in placentas from uncomplicated pregnancies from 10 weeks of gestation to term reveal no evidence for placental senescence up to term, the rate of growth of the villous surface area decreases gradually from approximately 34 weeks gestation onward (Boyd 1984). The number of nuclei in cytotrophoblast and syncytiotrophoblast continuously increased while the percentage of cytotrophoblast maintains at 12–13% throughout villous arborizations (Sen et al. 1979). An increase of syncytial knot formation is observed during gestation. Thus apoptosis occurs in normal placental tissues, mainly in villous trophoblast (Smith et al. 1997b; Mayhew et al. 1999). Apoptosis is, however, enhanced in pregnancies complicated by preeclampsia (Leung et al. 2001) and also IUGR (Smith et al. 1997a) where the inadequate perfusion of the intervillous space is thought to give rise to oxidative stress.
Reactive oxygen species mediate cytokine-induced trophoblast apoptosis (Smith et al. 1999) and pO2 differentially regulates apoptosis events. Both basal and TNFα-induced apoptosis were highest when term cytotrophoblast was exposed to 0% O2 (pO2<10 mmHg; Kilani et al. 2003). Cytotrophoblast was resistant to apoptosis when cultured at intermediate oxygen levels, i.e., 2–5% O2. Severe hypoxia (2% O2), however, increased syncytiotrophoblast necrotic shedding (Huppertz et al. 2003). Similarly, apoptosis of chorion leave trophoblast is induced by oxidative stress (Ohyama et al. 2001).
Effect of ROS on placental angiogenesis
Placental angiogenesis is regulated by maternal and placental growth hormones. Placental growth factor (PIGF) belongs to the VEGF family of growth factors and significant expression of PIGF is found in the placenta (Maglione et al. 1991, 1993; Hauser and Weich 1993), with the primary site of synthesis being trophoblast (Khaliq et al. 1996; Shore et al. 1997; Vuorela et al. 1997). Recently hypoxia was shown to differentially regulate PIGF and VEGF expression; PIGF is downregulated by hypoxia while VEGF mRNA is upregulated (Khaliq et al. 1996). Elevated VEGF mRNA was detected in trophoblast-derived cells which were cultured under hypoxic conditions known to cause ROS generation (Taylor et al. 1997). This might be due to ROS increasing VEGF mRNA stability (Kuroki et al. 1996). Exogenous VEGF induces 3H-thymidine incorporation an effect mediated by p42/p44MAPK via induction of eNOS in BeWo cells (Cha et al. 2001).
The mitogen-activated protein kinases (MAPK) are activated by oxidative stress in various cell types (Torres 2003). MAPK cascades seem to be involved in placental development since mutation in the mouse gene resulted in deficient phenotypes (Giroux et al. 1999; Adams et al. 2000; Mudgett et al. 2000; Yang et al. 2000). Targeted disruption of the p38αSAPK gene results in homozygous embryonic lethality due to severe defects in placental development which appear to be secondary to insufficient oxygen and nutrient transfer across the placenta (Adams et al. 2000). In particular, p38αSAPK mutant placentas display a lack of vascularization of the labyrinth layer as well as increased rates of apoptosis, consistent with a defect in placental angiogenesis and lack of expression of VEGF and angiopoietin. When the placental defect was rescued, p38αSAPK(−/−) embryos developed to term and were normal in appearance (Mudgett et al. 2000).
Effect of oxidative stress on placental vascular reactivity
Oxidative stress may increase production of superoxide and nitric oxide, leading to formation of prooxidant peroxynitrite to cause vascular dysfunction. We find nitrotyrosine residues in the placenta in preeclampsia and diabetes but the functional significance remains to be fully elucidated. We sought to directly determine (Kossenjans et al. 2000) whether peroxynitrite caused a functional deficit in the placental vascular bed in placentas of pregnancies complicated by preeclampsia or diabetes by comparing the responses of diabetic, preeclamptic, and normal placentas to increasing concentrations of the vasoconstrictors U46619 and angiotensin II and the vasodilators glyceryl trinitrate and prostacyclin. In addition, we determined the response to these agents in normal placentas before and after treatment with authentic peroxynitrite for 30 min. Interestingly, we found that the responses to both vasoconstrictors and vasodilators were significantly attenuated in diabetic and preeclamptic placentas compared to controls. Similarly, the responses to U46619, glyceryl trinitrate, and prostacyclin, but not angiotensin II, were significantly attenuated in a normal placenta following peroxynitrite treatment. Immunostaining for nitrotyrosine residues confirmed that nitrotyrosine residues were present in the placenta from preeclamptic and diabetic pregnancies, but also that peroxynitrite treatment of the placental vasculature led to the formation of nitrotyrosine residues (Kossenjans et al. 2000). Taken together, these data suggest but do not prove a cause-and-effect relationship whereby peroxynitrite formation in the placental vasculature is capable of attenuating vascular responses. A significant attenuation of the vasoconstrictor response to U46619 in the fetal-placental circulation of women with preeclampsia was also reported (Read et al. 1999), although no effect was seen on vasodilator responses to prostacyclin. Similarly, Wilkes et al. (1994) found responses to U46619 to be attenuated in the fetal-placental vasculature of diabetic pregnancies accompanied by reduction of the affinity of thromboxane receptors.
Protein tyrosine nitration has been detected under apparently normal physiologic conditions (Greenacre and Ischiropoulos 2001) in numerous tissues including endothelial cells, fibroblasts, and vascular smooth muscle cells (Davidge et al. 1998; Frustaci et al. 2000; Kajstura et al. 2001). Several nitrated proteins have been identified including myofibrillar creatine kinase (Mihm et al. 2001a), PGI2 synthase (Zou et al. 1999), and heart succinyl-Co-A:3-oxoacid CoA transferase (Turko et al. 2001), and structural proteins such as myosin heavy chain, α-actinin, and desmin (Mihm et al. 2001b). Low levels of protein nitration may be a physiologic regulatory mechanism in redox regulation for signaling pathways by changing tyrosine into a negatively charge hydrophilic nitrotyrosine moiety and changing the function of a protein. A gain of function as well as no effect on function were reported for tyrosine nitrated proteins (Gole et al. 2000; Balafanova et al. 2002). More commonly, however, inhibition of function is found (Ischiropoulos 1998; Greenacre and Ischiropoulos 2001). Tyrosine nitration may function as a feedback inhibitory mechanism as ONOO− inhibits inducible NOS activity (Robinson et al. 2001) and inhibits XO activity and O2− activity (Lee et al. 2000). Conversely as ONOO− inhibits SOD activity it may exacerbate oxidative stress (MacMillan-Crow et al. 1998). The concept of protein nitration functioning as a posttranslational modification akin to phosphorylation is attractive and has been studied. Proteomics (2D gel electrophoresis and mass spectrometry) has been used to identify nitrated proteins (Aulak et al. 2001). A putative denitrase activity has been demonstrated (Gow et al. 1996; Kuo et al. 1999, 2002), however, neither the enzyme responsible nor the reaction product have been identified to date.
Our subsequent studies will identify the protein targets that are covalently modified by peroxynitrite.
References
Adams RH, Porras A, Alonso G, Jones M, Vintersten K, Panelli S, Valladares A, Perez L, Klein R, Nebreda AR (2000) Essential role of p38alpha MAP kinase in placental but not embryonic cardiovascular development. Mol Cell 6:109–116
Allaire AD, Ballenger KA, Wells SR, McMahon MJ, Lessey BA (2000) Placental apoptosis in preeclampsia. Obstet Gynecol 96:271–276
Al-Mehdi AB, Zhao G, Dodia C, Tozawa K, Costa K, Muzykantov V, Ross C, Blecha F, Dinauer M, Fisher AB (1998) Endothelial NADPH oxidase as the source of oxidants in lungs exposed to ischemia or high K+. Circ Res 83:730–737
Alsat E, Wyplosz P, Malassine A, Guibourdenche J, Porquet D, Nessmann C, Evain-Brion D (1996) Hypoxia impairs cell fusion and differentiation process in human cytotrophoblast, in vitro. J Cell Physiol 168:346–353
Aly AS, Khandelwal M, Zhao J, Mehmet AH, Sammel MD, Parry S (2004) Neutrophils are stimulated by syncytiotrophoblast microvillous membranes to generate superoxide radicals in women with preeclampsia. Am J Obstet Gynecol 190:252–258
Arbiser JL, Petros J, Klafter R, Govindajaran B, McLaughlin ER, Brown LF, Cohen C, Moses M, Kilroy S, Arnold RS, Lambeth JD (2002) Reactive oxygen generated by Nox1 triggers the angiogenic switch. Proc Natl Acad Sci U S A 99:715–720
Aulak KS, Miyagi M, Yan L, West KA, Massillon D, Crabb JW, Stuehr DJ (2001) Proteomic method identifies proteins nitrated in vivo during inflammatory challenge. Proc Natl Acad Sci U S A 98:12056–12061
Babior BM, Lambeth JD, Nauseef W (2002) The neutrophil NADPH oxidase. Arch Biochem Biophys 397:342–344
Baker CS, Frost MT, Rimoldi O, Moore K, Halliwell B, Polak JM, Camici PG, Hall RJ (2002) Repetitive myocardial stunning in pigs is associated with an increased formation of reactive nitrogen species. Heart 87:77–78
Balafanova Z, Bolli R, Zhang J, Zheng Y, Pass JM, Bhatnagar A, Tang XL, Wang O, Cardwell E, Ping P (2002) Nitric oxide (NO) induces nitration of protein kinase C epsilon (PKCepsilon), facilitating PKCepsilon translocation via enhanced PKCepsilon-RACK2 interactions: a novel mechanism of NO-triggered activation of PKCepsilon. J Biol Chem 277:15021–15027
Barber A, Robson SC, Myatt L, Bulmer JN, Lyall F (2001) Heme oxygenase expression in human placenta and placental bed: reduced expression of placenta endothelial HO-2 in preeclampsia and fetal growth restriction. FASEB J 15:1158–1168
Beckman JS, Koppenol WH (1996) Nitric oxide, superoxide, and peroxynitrite: the good, the bad, and the ugly. Am J Physiol 271:C1424–C1437
Beckman JS, Beckman TW, Chen J, Marshall PA, Freeman BA (1990) Apparent hydroxyl radical production by peroxynitrite: implications for endothelial injury from nitric oxide and superoxide. Proc Natl Acad Sci U S A 87:1620–1624
Beckman J, Ye Y, Anderson P, Chen J, Accqvitti M, Trapey M, White C (1994) Extensive nitration of protein tyrosines in human atherosclerosis detected by immunohistochemistry. Biol Chem 375:81–88
Benkusky NA, Lewis SJ, Kooy NW (1999) Peroxynitrite-mediated attenuation of alpha- and beta-adrenoceptor agonist-induced vascular responses in vivo. Eur J Pharmacol 364:151–158
Boyd PA (1984) Quantitative structure of the normal human placenta from 10 weeks of gestation to term. Early Hum Dev 9:297–307
Brar SS, Corbin Z, Kennedy TP, Hemendinger R, Thornton L, Bommarius B, Arnold RS, Whorton AR, Sturrock AB, Huecksteadt TP, Quinn MT, Krenitsky K, Ardie KG, Lambeth JD, Hoidal JR (2003) NOX5 NAD(P)H oxidase regulates growth and apoptosis in DU145 prostate cancer cells. Am J Physiol Cell Physiol
Caniggia I, Winter J, Lye SJ, Post M (2000) Oxygen and placental development during the first trimester: implications for the pathophysiology of pre-eclampsia. Placenta 21(suppl A):S25–S30
Caraceni P, Ryu HS, van Thiel DH, Borle AB (1995) Source of oxygen free radicals produced by rat hepatocytes during postanoxic reoxygenation. Biochim Biophys Acta 1268:249–254
Casasco A, Calligaro A, Casasco M, Tateo S, Icaro Cornaglia A, Reguzzoni M, Farina A (1997) Immunohistochemical localization of lipoperoxidation products in normal human placenta. Placenta 18:249–253
Cester N, Staffolani R, Rabini RA, Magnanelli R, Salvolini E, Galassi R, Mazzanti L, Romanini C (1994) Pregnancy induced hypertension: a role for peroxidation in microvillus plasma membranes. Mol Cell Biochem 131:151–155
Cha MS, Lee MJ, Je GH, Kwak JY (2001) Endogenous production of nitric oxide by vascular endothelial growth factor down-regulates proliferation of choriocarcinoma cells. Biochem Biophys Res Commun 282:1061–1066
Chance B, Sies H, Boveris A (1979) Hydroperoxide metabolism in mammalian organs. Physiol Rev 59:527–605
Chandel N, Budinger GR, Kemp RA, Schumacker PT (1995) Inhibition of cytochrome-c oxidase activity during prolonged hypoxia. Am J Physiol 268:L918–L925
Chen Q, Vazquez EJ, Moghaddas S, Hoppel CL, Lesnefsky EJ (2003) Production of reactive oxygen species by mitochondria: central role of complex III. J Biol Chem 278:36027–36031
Conrad KP, Miles TM, Benyo DF (1998) Circulating levels of immunoreactive cytokines in women with preeclampsia. Am J Reprod Immunol 40:102–111
Davidge ST, Ojimba J, McLaughlin MK (1998) Vascular function in the vitamin E-deprived rat: an interaction between nitric oxide and superoxide anions. Hypertension 31:830–835
Dechend R, Viedt C, Muller DN, Ugele B, Brandes RP, Wallukat G, Park JK, Janke J, Barta P, Theuer J, Fiebeler A, Homuth V, Dietz R, Haller H, Kreuzer J, Luft FC (2003) AT1 receptor agonistic antibodies from preeclamptic patients stimulate NADPH oxidase. Circulation 107:1632–1639
De Deken X, Wang D, Many MC, Costagliola S, Libert F, Vassart G, Dumont JE, Miot F (2000) Cloning of two human thyroid cDNAs encoding new members of the NADPH oxidase family. J Biol Chem 275:23227–23233
Eis AL, Brockman DE, Pollock JS, Myatt L (1995) Immunohistochemical localization of endothelial nitric oxide synthase in human villous and extravillous trophoblast populations and expression during syncytiotrophoblast formation in vitro. Placenta 16:113–126
Frendo JL, Therond P, Bird T, Massin N, Muller F, Guibourdenche J, Luton D, Vidaud M, Anderson WB, Evain-Brion D (2001) Overexpression of copper zinc superoxide dismutase impairs human trophoblast cell fusion and differentiation. Endocrinology 142:3638–3648
Frustaci A, Kajstura J, Chimenti C, Jakoniuk I, Leri A, Maseri A, Nadal-Ginard B, Anversa P (2000) Myocardial cell death in human diabetes. Circ Res 87:1123–1132
Garner P, D’Alton M, Dudley D, Huard P, Hardie M (1990) Preeclampsia in diabetic pregnancies. Am J Obstet Gynecol 162:505–508
Genbacev O, Joslin R, Damsky CH, Polliotti BM, Fisher SJ (1996) Hypoxia alters early gestation human cytotrophoblast differentiation/invasion in vitro and models the placental defects that occur in preeclampsia. J Clin Invest 97:540–550
Genbacev O, Zhou Y, Ludlow JW, Fisher SJ (1997) Regulation of human placental development by oxygen tension. Science 277:1669–1672
Gervasi MT, Chaiworapongsa T, Pacora P, Naccasha N, Yoon BH, Maymon E, Romero R (2001) Phenotypic and metabolic characteristics of monocytes and granulocytes in preeclampsia. Am J Obstet Gynecol 185:792–797
Giroux S, Tremblay M, Bernard D, Cardin-Girard JF, Aubry S, Larouche L, Rousseau S, Huot J, Landry J, Jeannotte L, Charron J (1999) Embryonic death of Mek1-deficient mice reveals a role for this kinase in angiogenesis in the labyrinthine region of the placenta. Curr Biol 9:369–372
Gole MD, Souza JM, Choi I, Hertkorn C, Malcolm S, Foust RF III, Finkel B, Lanken PN, Ischiropoulos H (2000) Plasma proteins modified by tyrosine nitration in acute respiratory distress syndrome. Am J Physiol Lung Cell Mol Physiol 278:L961–L967
Gow AJ, Duran D, Malcolm S, Ischiropoulos H (1996) Effects of peroxynitrite-induced protein modifications on tyrosine phosphorylation and degradation. FEBS Lett 385:63–66
Greenacre SA, Ischiropoulos H (2001) Tyrosine nitration: localisation, quantification, consequences for protein function and signal transduction. Free Radic Res 34:541–581
Griendling KK, Sorescu D, Ushio-Fukai M (2000) NAD(P)H oxidase: role in cardiovascular biology and disease. Circ Res 86:494–501
Haddad IY, Pataki G, Hu P, Galliani C, Beckman JS, Matalon S (1994) Quantitation of nitrotyrosine levels in lung sections of patients and animals with acute lung injury. J Clin Invest 94:2407–2413
Hassoun PM, Yu FS, Shedd AL, Zulueta JJ, Thannickal VJ, Lanzillo JJ, Fanburg BL (1994) Regulation of endothelial cell xanthine dehydrogenase xanthine oxidase gene expression by oxygen tension. Am J Physiol 266:L163–L171
Hauser S, Weich HA (1993) A heparin-binding form of placenta growth factor (PlGF-2) is expressed in human umbilical vein endothelial cells and in placenta. Growth Factors 9:259–268
Hempstock J, Bao YP, Bar-Issac M, Segaren N, Watson AL, Charnock-Jones DS, Jauniaux E, Burton GJ (2003a) Intralobular differences in antioxidant enzyme expression and activity reflect the pattern of maternal arterial bloodflow within the human placenta. Placenta 24:517–523
Hempstock J, Jauniaux E, Greenwold N, Burton GJ (2003b) The contribution of placental oxidative stress to early pregnancy failure. Hum Pathol 34:1265–1275
Hoang VM, Foulk R, Clauser K, Burlingame A, Gibson BW, Fisher SJ (2001) Functional proteomics: examining the effects of hypoxia on the cytotrophoblast protein repertoire. Biochemistry 40:4077–4086
Honing ML, Morrison PJ, Banga JD, Stroes ES, Rabelink TJ (1998) Nitric oxide availability in diabetes mellitus. Diabetes Metab Rev 14:241–249
Hung TH, Skepper JN, Burton GJ (2001) In vitro ischemia-reperfusion injury in term human placenta as a model for oxidative stress in pathological pregnancies. Am J Pathol 159:1031–1043
Huppertz B, Kingdom J, Caniggia I, Desoye G, Black S, Korr H, Kaufmann P (2003) Hypoxia favours necrotic versus apoptotic shedding of placental syncytiotrophoblast into the maternal circulation. Placenta 24:181–190
Ischiropoulos H (1998) Biological tyrosine nitration: a pathophysiological function of nitric oxide and reactive oxygen species. Arch Biochem Biophys 356:1–11
Ischiropoulos H, Zhu L, Chen J, Tsai M, Martin JC, Smith CD, Beckman JS (1992) Peroxynitrite-mediated tyrosine nitration catalyzed by superoxide dismutase. Arch Biochem Biophys 298:431–437
Ishihara N, Matsuo H, Murakoshi H, Laoag-Fernandez JB, Samoto T, Maruo T (2002) Increased apoptosis in the syncytiotrophoblast in human term placentas complicated by either preeclampsia or intrauterine growth retardation. Am J Obstet Gynecol 186:158–166
Jauniaux E, Watson AL, Hempstock J, Bao YP, Skepper JN, Burton GJ (2000) Onset of maternal arterial blood flow and placental oxidative stress. A possible factor in human early pregnancy failure. Am J Pathol 157:2111–2122
Jauniaux E, Greenwold N, Hempstock J, Burton GJ (2003) Comparison of ultrasonographic and Doppler mapping of the intervillous circulation in normal and abnormal early pregnancies. Fertil Steril 79:100–106
Kajstura J, Fiordaliso F, Andreoli AM, Li B, Chimenti S, Medow MS, Limana F, Nadal-Ginard B, Leri A, Anversa P (2001) IGF-1 overexpression inhibits the development of diabetic cardiomyopathy and angiotensin II-mediated oxidative stress. Diabetes 50:1414–1424
Khaliq A, Li XF, Shams M, Sisi P, Acevedo CA, Whittle MJ, Weich H, Ahmed A (1996) Localisation of placenta growth factor (PIGF) in human term placenta. Growth Factors 13:243–250, color plates I–II pre bk cov
Kilani RT, Mackova M, Davidge ST, Guilbert LJ (2003) Effect of oxygen levels in villous trophoblast apoptosis. Placenta 24:826–834
Knapen MF, Peters WH, Mulder TP, Merkus HM, Jansen JB, Steegers EA (1999) Glutathione and glutathione-related enzymes in decidua and placenta of controls and women with pre-eclampsia. Placenta 20:541–546
Kossenjans W, Eis A, Sahay R, Brockman D, Myatt L (2000) Role of peroxynitrite in altered fetal-placental vascular reactivity in diabetes or preeclampsia. Am J Physiol Heart Circ Physiol 278:H1311–H1319
Kudin AP, Bimpong-Buta NY, Vielhaber S, Elger CE, Kunz WS (2004) Characterization of superoxide-producing sites in isolated brain mitochondria. J Biol Chem 279:4127–4135
Kudo Y, Boyd CA, Sargent IL, Redman CW (2003) Hypoxia alters expression and function of syncytin and its receptor during trophoblast cell fusion of human placental BeWo cells: implications for impaired trophoblast syncytialisation in pre-eclampsia. Biochim Biophys Acta 1638:63–71
Kuo WN, Kanadia RN, Shanbhag VP, Toro R (1999) Denitration of peroxynitrite-treated proteins by ‘protein nitratases’ from rat brain and heart. Mol Cell Biochem 201:11–16
Kuo WN, Kocis JM, Webb JK (2002) Protein denitration/modification by Escherichia coli nitrate reductase and mammalian cytochrome P-450 reductase. Front Biosci 7:a9–a14
Kuroki M, Voest EE, Amano S, Beerepoot LV, Takashima S, Tolentino M, Kim RY, Rohan RM, Colby KA, Yeo KT, Adamis AP (1996) Reactive oxygen intermediates increase vascular endothelial growth factor expression in vitro and in vivo. J Clin Invest 98:1667–1675
Lee CI, Liu X, Zweier JL (2000) Regulation of xanthine oxidase by nitric oxide and peroxynitrite. J Biol Chem 275:9369–9376
Lee VM, Quinn PA, Jennings SC, Ng LL (2003) NADPH oxidase activity in preeclampsia with immortalized lymphoblasts used as models. Hypertension 41:925–931
Leung DN, Smith SC, To KF, Sahota DS, Baker PN (2001) Increased placental apoptosis in pregnancies complicated by preeclampsia. Am J Obstet Gynecol 184:1249–1250
Li C, Wright MM, Jackson RM (2002) Reactive species mediated injury of human lung epithelial cells after hypoxia-reoxygenation. Exp Lung Res 28:373–389
Li N, Ragheb K, Lawler G, Sturgis J, Rajwa B, Melendez JA, Robinson JP (2003) Mitochondrial complex I inhibitor rotenone induces apoptosis through enhancing mitochondrial reactive oxygen species production. J Biol Chem 278:8516–8525
Liu P, Hock CE, Nagele R, Wong PY (1997) Formation of nitric oxide, superoxide, and peroxynitrite in myocardial ischemia-reperfusion injury in rats. Am J Physiol 272:H2327–H2336
Lyall F (2003) Development of the utero-placental circulation: the role of carbon monoxide and nitric oxide in trophoblast invasion and spiral artery transformation. Microsc Res Tech 60:402–411
Lyall F, Gibson JL, Greer IA, Brockman DE, Eis AL, Myatt L (1998) Increased nitrotyrosine in the diabetic placenta: evidence for oxidative stress. Diabetes Care 21:1753–1758
Lyall F, Barber A, Myatt L, Bulmer JN, Robson SC (2000) Hemeoxygenase expression in human placenta and placental bed implies a role in regulation of trophoblast invasion and placental function. FASEB J 14:208–219
MacMillan-Crow LA, Crow JP, Thompson JA (1998) Peroxynitrite-mediated inactivation of manganese superoxide dismutase involves nitration and oxidation of critical tyrosine residues. Biochemistry 37:1613–1622
Madazli R, Benian A, Aydin S, Uzun H, Tolun N (2002) The plasma and placental levels of malondialdehyde, glutathione and superoxide dismutase in pre-eclampsia. J Obstet Gynaecol 22:477–480
Maglione D, Guerriero V, Viglietto G, Delli-Bovi P, Persico MG (1991) Isolation of a human placenta cDNA coding for a protein related to the vascular permeability factor. Proc Natl Acad Sci U S A 88:9267–9271
Maglione D, Guerriero V, Viglietto G, Ferraro MG, Aprelikova O, Alitalo K, Del Vecchio S, Lei KJ, Chou JY, Persico MG (1993) Two alternative mRNAs coding for the angiogenic factor, placenta growth factor (PlGF), are transcribed from a single gene of chromosome 14. Oncogene 8:925–931
Manes C (2001) Human placental NAD(P)H oxidase: solubilization and properties. Placenta 22:58–63
Many A, Westerhausen-Larson A, Kanbour-Shakir A, Roberts JM (1996) Xanthine oxidase/dehydrogenase is present in human placenta. Placenta 17:361–365
Many A, Hubel CA, Fisher SJ, Roberts JM, Zhou Y (2000) Invasive cytotrophoblasts manifest evidence of oxidative stress in preeclampsia. Am J Pathol 156:321–331
Martin D, Conrad KP (2000) Expression of endothelial nitric oxide synthase by extravillous trophoblast cells in the human placenta. Placenta 21:23–31
Matsubara S, Sato I (2001) Enzyme histochemically detectable NAD(P)H oxidase in human placental trophoblasts: normal, preeclamptic, and fetal growth restriction-complicated pregnancy. Histochem Cell Biol 116:1–7
Matsubara S, Minakami H, Sato I, Saito T (1997) Decrease in cytochrome c oxidase activity detected cytochemically in the placental trophoblast of patients with pre-eclampsia. Placenta 18:255–259
Mayhew TM, Leach L, McGee R, Ismail WW, Myklebust R, Lammiman MJ (1999) Proliferation, differentiation and apoptosis in villous trophoblast at 13–41 weeks of gestation (including observations on annulate lamellae and nuclear pore complexes). Placenta 20:407–422
McAleer MF, Tuan RS (2001) Metallothionein protects against severe oxidative stress-induced apoptosis of human trophoblastic cells. In Vitro Mol Toxicol 14:219–231
McLean M, Bowman M, Clifton V, Smith R, Grossman AB (2000) Expression of the heme oxygenase-carbon monoxide signalling system in human placenta. J Clin Endocrinol Metab 85:2345–2349
Mihm MJ, Coyle CM, Schanbacher BL, Weinstein DM, Bauer JA (2001a) Peroxynitrite induced nitration and inactivation of myofibrillar creatine kinase in experimental heart failure. Cardiovasc Res 49:798–807
Mihm MJ, Yu F, Carnes CA, Reiser PJ, McCarthy PM, Van Wagoner DR, Bauer JA (2001b) Impaired myofibrillar energetics and oxidative injury during human atrial fibrillation. Circulation 104:174–180
Moncada S, Palmer RM, Higgs EA (1991) Nitric oxide: physiology, pathophysiology, and pharmacology. Pharmacol Rev 43:109–142
Morris JM, Gopaul NK, Endresen MJ, Knight M, Linton EA, Dhir S, Anggard EE, Redman CW (1998) Circulating markers of oxidative stress are raised in normal pregnancy and pre-eclampsia. Br J Obstet Gynaecol 105:1195–1199
Mudgett JS, Ding J, Guh-Siesel L, Chartrain NA, Yang L, Gopal S, Shen MM (2000) Essential role for p38alpha mitogen-activated protein kinase in placental angiogenesis. Proc Natl Acad Sci U S A 97:10454–10459
Mutlu-Turkoglu U, Aykac-Toker G, Ibrahimoglu L, Ademoglu E, Uysal M (1999) Plasma nitric oxide metabolites and lipid peroxide levels in preeclamptic pregnant women before and after delivery. Gynecol Obstet Invest 48:247–250
Myatt L, Brewer A, Brockman DE (1991) The action of nitric oxide in the perfused human fetal-placental circulation. Am J Obstet Gynecol 164:687–692
Myatt L, Rosenfield RB, Eis AL, Brockman DE, Greer I, Lyall F (1996) Nitrotyrosine residues in placenta. Evidence of peroxynitrite formation and action. Hypertension 28:488–493
Myatt L, Eis AL, Brockman DE, Greer IA, Lyall F (1997a) Endothelial nitric oxide synthase in placental villous tissue from normal, pre-eclamptic and intrauterine growth restricted pregnancies. Hum Reprod 12:167–172
Myatt L, Eis AL, Brockman DE, Kossenjans W, Greer I, Lyall F (1997b) Inducible (type II) nitric oxide synthase in human placental villous tissue of normotensive, pre-eclamptic and intrauterine growth-restricted pregnancies. Placenta 18:261–268
Myatt L, Eis AL, Brockman DE, Kossenjans W, Greer IA, Lyall F (1997c) Differential localization of superoxide dismutase isoforms in placental villous tissue of normotensive, pre-eclamptic, and intrauterine growth-restricted pregnancies. J Histochem Cytochem 45:1433–1438
Ohyama K, Yuan B, Bessho T, Yamakawa T (2001) Progressive apoptosis in chorion laeve trophoblast cells of human fetal membrane tissues during in vitro incubation is suppressed by antioxidative reagents. Eur J Biochem 268:6182–6189
Partridge CA, Blumenstock FA, Malik AB (1992) Pulmonary microvascular endothelial cells constitutively release xanthine oxidase. Arch Biochem Biophys 294:184–187
Poranen AK, Ekblad U, Uotila P, Ahotupa M (1998) The effect of vitamin C and E on placental lipid peroxidation and antioxidative enzymes in perfused placenta. Acta Obstet Gynecol Scand 77:372–376
Radi R, Beckman JS, Bush KM, Freeman BA (1991) Peroxynitrite-induced membrane lipid peroxidation: the cytotoxic potential of superoxide and nitric oxide. Arch Biochem Biophys 288:481–487
Radi R, Rodriguez M, Castro L, Telleri R (1994) Inhibition of mitochondrial electron transport by peroxynitrite. Arch Biochem Biophys 308:89–95
Read MA, Leitch IM, Giles WB, Bisits AM, Boura AL, Walters WA (1999) U46619-mediated vasoconstriction of the fetal placental vasculature in vitro in normal and hypertensive pregnancies. J Hypertens 17:389–396
Redman CW, Sargent IL (2000) Placental debris, oxidative stress and pre-eclampsia. Placenta 21:597–602
Robinson VK, Sato E, Nelson DK, Camhi SL, Robbins RA, Hoyt JC (2001) Peroxynitrite inhibits inducible (type 2) nitric oxide synthase in murine lung epithelial cells in vitro. Free Radic Biol Med 30:986–991
Rosen P, Nawroth PP, King G, Moller W, Tritschler HJ, Packer L (2001) The role of oxidative stress in the onset and progression of diabetes and its complications: a summary of a Congress Series sponsored by UNESCO-MCBN, the American Diabetes Association and the German Diabetes Society. Diabetes Metab Res Rev 17:189–212
Sen DK, Kaufmann P, Schweikhart G (1979) Classification of human placental villi. II. Morphometry. Cell Tissue Res 200:425–434
Shibata E, Ejima K, Nanri H, Toki N, Koyama C, Ikeda M, Kashimura M (2001) Enhanced protein levels of protein thiol/disulphide oxidoreductases in placentae from pre-eclamptic subjects. Placenta 22:566–572
Shore VH, Wang TH, Wang CL, Torry RJ, Caudle MR, Torry DS (1997) Vascular endothelial growth factor, placenta growth factor and their receptors in isolated human trophoblast. Placenta 18:657–665
Sikkema JM, van Rijn BB, Franx A, Bruinse HW, de Roos R, Stroes ES, van Faassen EE (2001) Placental superoxide is increased in pre-eclampsia. Placenta 22:304–308
Smith SC, Baker PN, Symonds EM (1997a) Increased placental apoptosis in intrauterine growth restriction. Am J Obstet Gynecol 177:1395–1401
Smith SC, Baker PN, Symonds EM (1997b) Placental apoptosis in normal human pregnancy. Am J Obstet Gynecol 177:57–65
Smith SC, Guilbert LJ, Yui J, Baker PN, Davidge ST (1999) The role of reactive nitrogen/oxygen intermediates in cytokine-induced trophoblast apoptosis. Placenta 20:309–315
Souren JE, Van Der Mast C, Van Wijk R (1997) NADPH-oxidase-dependent superoxide production by myocyte-derived H9c2 cells: influence of ischemia, heat shock, cycloheximide and cytochalasin D. J Mol Cell Cardiol 29:2803–2812
Spranger M, Kiprianova I, Krempien S, Schwab S (1998) Reoxygenation increases the release of reactive oxygen intermediates in murine microglia. J Cereb Blood Flow Metab 18:670–674
Tames F, Mackness M, Arrol S, Laing I, Durrington P (1992) Non-enzymatic glycation of apolipoprotein B in the sera of diabetic and non-diabetic subjects. Atherosclerosis 93:237–244
Taylor CM, Stevens H, Anthony FW, Wheeler T (1997) Influence of hypoxia on vascular endothelial growth factor and chorionic gonadotrophin production in the trophoblast-derived cell lines: JEG, JAr and BeWo. Placenta 18:451–458
Terada LS, Beehler CJ, Banerjee A, Brown JM, Grosso MA, Harken AH, McCord JM, Repine JE (1988) Hyperoxia and self- or neutrophil-generated O2 metabolites inactivate xanthine oxidase. J Appl Physiol 65:2349–2353
Torres M (2003) Mitogen-activated protein kinase pathways in redox signaling. Front Biosci 8:d369–d391
Turko IV, Marcondes S, Murad F (2001) Diabetes-associated nitration of tyrosine and inactivation of succinyl-CoA:3-oxoacid CoA-transferase. Am J Physiol Heart Circ Physiol 281:H2289–H2294
van Kreel BK, van Dijk JP (1977) Transport of uric acid and hypoxanthine across the isolated guinea pig placenta. Biol Neonate 32:260–265
Vaughan JE, Walsh SW (2002) Oxidative stress reproduces placental abnormalities of preeclampsia. Hypertens Pregnancy 21:205–223
Villa LM, Salas E, Darley-Usmar VM, Radomski MW, Moncada S (1994) Peroxynitrite induces both vasodilatation and impaired vascular relaxation in the isolated perfused rat heart. Proc Natl Acad Sci U S A 91:12383–12387
Vuorela P, Hatva E, Lymboussaki A, Kaipainen A, Joukov V, Persico MG, Alitalo K, Halmesmaki E (1997) Expression of vascular endothelial growth factor and placenta growth factor in human placenta. Biol Reprod 56:489–494
Wajner M, Harkness RA (1989) Distribution of xanthine dehydrogenase and oxidase activities in human and rabbit tissues. Biochim Biophys Acta 991:79–84
Walsh SW, Vaughan JE, Wang Y, Roberts LJ II (2000) Placental isoprostane is significantly increased in preeclampsia. FASEB J 14:1289–1296
Wang Y, Walsh SW (1996a) Antioxidant activities and mRNA expression of superoxide dismutase, catalase, and glutathione peroxidase in normal and preeclamptic placentas. J Soc Gynecol Investig 3:179–184
Wang Y, Walsh SW (1996b) TNF alpha concentrations and mRNA expression are increased in preeclamptic placentas. J Reprod Immunol 32:157–169
Wang Y, Walsh SW (1998) Placental mitochondria as a source of oxidative stress in pre-eclampsia. Placenta 19:581–586
Wang Y, Walsh SW (2001) Increased superoxide generation is associated with decreased superoxide dismutase activity and mRNA expression in placental trophoblast cells in pre-eclampsia. Placenta 22:206–212
Wang P, Zweier JL (1996) Measurement of nitric oxide and peroxynitrite generation in the postischemic heart. Evidence for peroxynitrite-mediated reperfusion injury. J Biol Chem 271:29223–29230
Wang Y, Gu Y, Philibert L, Lucas MJ (2001) Neutrophil activation induced by placental factors in normal and pre-eclamptic pregnancies in vitro. Placenta 22:560–565
Watson AL, Skepper JN, Jauniaux E, Burton GJ (1998) Susceptibility of human placental syncytiotrophoblastic mitochondria to oxygen-mediated damage in relation to gestational age. J Clin Endocrinol Metab 83:1697–1705
Waypa GB, Chandel NS, Schumacker PT (2001) Model for hypoxic pulmonary vasoconstriction involving mitochondrial oxygen sensing. Circ Res 88:1259–1266
Wice B, Menton D, Geuze H, Schwartz AL (1990) Modulators of cyclic AMP metabolism induce syncytiotrophoblast formation in vitro. Exp Cell Res 186:306–316
Wilkes BM, Mento PF, Hollander AM (1994) Reduced thromboxane receptor affinity and vasoconstrictor responses in placentae from diabetic pregnancies. Placenta 15:845–855
Wisdom SJ, Wilson R, McKillop JH, Walker JJ (1991) Antioxidant systems in normal pregnancy and in pregnancy-induced hypertension. Am J Obstet Gynecol 165:1701–1704
Yang J, Boerm M, McCarty M, Bucana C, Fidler IJ, Zhuang Y, Su B (2000) Mekk3 is essential for early embryonic cardiovascular development. Nat Genet 24:309–313
Yoshiki N, Kubota T, Aso T (2000) Expression and localization of heme oxygenase in human placental villi. Biochem Biophys Res Commun 276:1136–1142
Zhang J, Dawson VL, Dawson TM, Snyder SH (1994) Nitric oxide activation of poly(ADP-ribose) synthetase in neurotoxicity. Science 263:687–689
Zou MH, Leist M, Ullrich V (1999) Selective nitration of prostacyclin synthase and defective vasorelaxation in atherosclerotic bovine coronary arteries. Am J Pathol 154:1359–1365
Zulueta JJ, Yu FS, Hertig IA, Thannickal VJ, Hassoun PM (1995) Release of hydrogen peroxide in response to hypoxia-reoxygenation: role of an NAD(P)H oxidase-like enzyme in endothelial cell plasma membrane. Am J Respir Cell Mol Biol 12:41–49
Zusterzeel PL, Peters WH, De Bruyn MA, Knapen MF, Merkus HM, Steegers EA (1999) Glutathione S-transferase isoenzymes in decidua and placenta of preeclamptic pregnancies. Obstet Gynecol 94:1033–1038
Zusterzeel PL, Rutten H, Roelofs HM, Peters WH, Steegers EA (2001a) Protein carbonyls in decidua and placenta of pre-eclamptic women as markers for oxidative stress. Placenta 22:213–219
Zusterzeel PL, Wanten GJ, Peters WH, Merkus HM, Steegers EA (2001b) Neutrophil oxygen radical production in pre-eclampsia with HELLP syndrome. Eur J Obstet Gynecol Reprod Biol 99:213–218
Zweier JL, Fertmann J, Wei G (2001) Nitric oxide and peroxynitrite in postischemic myocardium. Antioxid Redox Signal 3:11–22
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Myatt, L., Cui, X. Oxidative stress in the placenta. Histochem Cell Biol 122, 369–382 (2004). https://doi.org/10.1007/s00418-004-0677-x
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00418-004-0677-x