
Abstract
Purpose
To report the anatomical characteristics of wide-based foveal pit and its possible associations with macular diseases.
Methods
Wide-based foveal pit was defined as a foveal base width (FBW) larger than the mean value plus one standard deviation of the normal population. Eyes with a wide-based foveal pit were retrospectively collected as the study group, and age- and sex-matched subjects with a normal FBW were recruited as the control group. FBW, area of foveal avascular zone (FAZ), and retinal artery trajectory (RAT) were compared between the two groups. The characteristics of the fellow eyes in the study group were also described.
Results
Fifty-two eyes from 52 patients were identified as having a wide-based foveal pit; 43 (82.7%) were female. Both their FBW (474.7 ± 84.6 μm) and area of FAZ (0.50 ± 0.11 mm2) were significantly larger than in the control group (297.6 ± 42.3 μm and 0.29 ± 0.10 mm2, respectively; p < 0.001 for both), and they also had a wider RAT than the control group (p < 0.001). During follow-up, three eyes had developed idiopathic epiretinal membrane. As for their fellow eyes, they either also had a wide-based foveal pit (11 eyes) or had various macular diseases including idiopathic epiretinal membrane (27 eyes), macular hole (5 eyes), and others (16 eyes).
Conclusions
Eyes with a wide-based foveal pit had a large FAZ and a wide RAT, and they might have a predisposition to idiopathic epiretinal membrane formation. Their fellow eyes also had a predisposition to epiretinal membrane and macular hole.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.

Introduction
The fovea is a pitted structure in the center of the macula. At the center of the fovea lies the foveola, which is 0.35 mm in size with a depressed center known as the umbo. Histologically, the foveola lacks inner retinal layers, and is also devoid of vasculature. Photoreceptors, specifically cone cells, are densely packed in the foveola [1]. Due to the depletion of inner retinal layers, light is less scattered during transmission, which in turn gives rise to the high spatial resolution of vision in this area.
The invention of optical coherence tomography (OCT) permitted easier assessment of the structure of the retina and facilitated inspection of the contour of the foveal pit [2, 3]. The different contours of the foveal pit have given rise to a variety of methods to describe the foveal pit contour. All such methods—from measuring the dimensions of the base, slope and shoulder to using mathematic approaches to fit the foveal pit contour into reverse Gaussian equations—have demonstrated the complexity of outlining the foveal pit [4, 5]. Given the many different descriptions, controversy remains as to whether we can define certain parameters to differentiate normal foveal contours from pathological ones. Clinically, we have noticed that eyes with a wide-based foveal pit have normal vision without metamorphopsia, but their fellow eyes had either a similar wide-based foveal pit or various kinds of macular diseases. Therefore, we believed this type of foveal contour merited further study.
A previous study has shown that as compared with the normal fellow eye, patients with macular hole have a widened retinal artery trajectory (RAT), the curve composed of the optic nerve center and the paths of both major temporal retinal arteries [6]. The possible mechanism could be the tangential tractional forces on the vitreomacular interface. We speculated that eyes with a wide foveal base might also have an abnormal RAT. In this proof-of-principle study, we collected information on eyes with a wide-based foveal pit as well as their fellow eyes; we described their anatomical characteristics and compared them with normal subjects.
Material and methods
Study subjects
We retrospectively reviewed consecutive patients who had received macular OCT and OCT angiography (OCTA) using Optovue Avanti RTVue XR OCT (Optovue, Inc., Fremont, CA, USA) in single ophthalmologist’s clinic (Y-T Hsieh) at the National Taiwan University Hospital between November 2016 and August 2018. During the first stage, we chose 50 male and 50 female patients with normal macular structures and foveal contours to represent the normal population. These subjects primarily received OCT for preoperative evaluation for cataract surgery, refractive surgery, or routine check-up during the study period. Those with any of the following characteristics were excluded: (1) irregular or asymmetric foveal contour, (2) retinal tissue loss at the fovea or parafoveal area, (3) any vitreomacular or choroidal diseases noted on OCT or fundus photography, (4) presence of posterior staphyloma, (5) symptoms of metamorphopsia and (6) incomplete data for the axial length, fundus images or B-scan and en face angiography images on OCT. We then measured the foveal base width (FBW), which was defined as the distance between two intersections of internal limiting membrane (ILM) and a line parallel to the underlying retinal pigment epithelium layer at 10 μm above the lowest point of the foveal pit in the B-scan OCT image (Fig. 1). We used both the horizontal and vertical sections of B-scan OCT for measurement, and recorded the mean value as the FBW. Only one eye was randomly selected from each subject for calculation. Of the 100 normal eyes, the mean FBW was 321.8 ± 67.8 μm. We then defined a wide-based foveal pit as a FBW larger than the mean value plus one standard deviation of normal population, which was 390 μm.

Measurement of the width of the foveal pit. We drew a line parallel to the retinal pigment epithelial layer (dotted black line) at the level of 10 μm above the deepest point of the foveal pit, then measured the distance between its intersections with the retinal inner surface as the width of the foveal pit (638 μm in this example)
During the second stage, we retrospectively collected eyes with a wide-based foveal pit measured during the same period. The exclusion criteria were the same as for the normal population in the first stage. For subjects whose eyes both matched the criteria for wide-based foveal pit, only one eye was enrolled in the study group. We also collected information on the fellow eyes of the study group for analysis. As for the control group, we recruited age- and sex-matched subjects (same sex, age difference < 5 years) who had a FBW equal to or smaller than 390 μm measured during the same period. We collected the demographics and clinical characteristics, including age, sex, axial length, status of posterior vitreous detachment, and any macular diseases noted on OCT or fundus images. The horizontal and vertical B-scan OCT images and the en face angiography images of the macula were obtained for analysis. We obtained the fundus images using either color fundus photography, fundus auto-fluorescence, or infrared fundus image obtained from the OCT machine.
This study was approved by the Ethics Committee and Institutional Review Board of National Taiwan University Hospital (No.: 201908068RINC) and adhered to the Declaration of Helsinki.
Parameters of the foveal pit
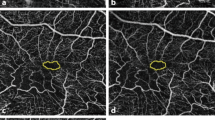
The parameters of the foveal pit included the FBW and the area of the foveal avascular zone (FAZ). The method of measurement of FBW has been described above. The FAZ was outlined as the region without vasculature in the en face OCTA image, and the area of the FAZ was calculated using the built-in algorithm of the Optovue Avanti RTVue XR OCT.
Retinal artery trajectory
We measured RAT using a modified version of the method proposed by Yoshihara et al. [6]. First, we rotated the fundus images 90 degrees clockwise for right eyes and 90 degrees counterclockwise for left eyes using ImageJ (version 1.47, National Institutes of Health, Bethesda, MD, USA; available at: http://imagej.nih.gov/ij/). We then manually dotted along the arterial arcades, placing the first dot at the site where the retinal artery emanates from the optic disc. We labeled each fundus photograph with 20 to 24 dots and generated the x-y coordination with the “invert Y coordinate” function of ImageJ. We then fit those coordinates to the best fit curve with a second-degree polynomial equation. The coefficient of the second-degree polynomial represents the width of the artery curve, with a larger coefficient representing a narrower curve (Fig. 2). All RAT measurements were performed by the same person (I-H Ma), and repeated measurements of RAT were done in seven eyes at different times to verify the measurement bias.

Measurement of the retinal artery trajectory (RAT) from color fundus photography. We manually placed 20 to 24 dots along the arcade arteries, with the first at the site where the retinal artery emanates from the optic disc (sample blue dots shown). These dots then fitted to the best fit curve with a second-degree polynomial equation using the “invert Y coordinate” function of ImageJ (lower part)
Statistical analysis
We used paired t tests to compare continuous variables (axial length, FBW, area of FAZ, and RAT) between the study group and their fellow eyes, as well as between the study group and their paired matches in the control group. We also used paired t tests to examine the difference between repeated measurements of RAT. A p value of less than 0.05 was statistically significant. A Bland-Altman plot was drawn to present the intersessional variation of RAT measurement.
Results
Demographics
We enrolled a total of 52 eyes with a wide-based foveal pit from 52 patients in the study group. The mean age was 63.4 ± 9.3 years, and 43 of the participants (83%) were female. The mean axial length was 23.9 ± 1.85 mm and 38 eyes (73%) had complete posterior vitreous detachment. The control group contained 52 eyes in 52 patients who were matched to the study group by age and sex. No statistically significant differences in age or axial length between the study group and the control group were noted (p = 0.87 and p = 0.38 respectively) (Table 1).
Parameters of foveal pit and RAT
The mean FBW in the wide-based group was 474.7 ± 84.6 μm, which was significantly larger than that in the control group (297.6 ± 42.3 μm, p < 0.001). The mean FAZ area was 0.50 ± 0.11 mm2 in those with a wide-based foveal pit, which was also significantly larger than that in the control group (0.29 ± 0.10 mm2, p < 0.001). As for the RAT, the mean coefficient was 0.18 ± 0.11 in the study group and 0.31 ± 0.14 in the control group (p < 0.001), indicating that those with a wide-based foveal pit had a wider RAT than did the normal controls (Table 1). The intersessional variability of RAT was small as demonstrated in the Bland-Altman plot (Fig. 3).

Bland-Altman plot for repeated mesurements of retinal artery trajectory.

Sequential optical coherent tomography scans of three cases with a wide-based foveal pit showed idiopathic epiretinal membrane formation during the follow-up examinations. a, c, e At baseline; b 12 months later of a; d 12 months later of c; f 18 months later of e
Development of idiopathic epiretinal membrane
Three eyes with a wide-based foveal pit developed idiopathic epiretinal membrane (ERM) after a follow-up period of 12 months (2 patients) and 18 months (1 patient), respectively (Fig. 4). In one case, the ERM was only visible on B-scan OCT with mild disturbance of the foveal pattern; the other two eyes developed ERM, which also narrowed the RAT with a noticeable increase of the coefficient from 0.38 to 0.57 in one, and from 1.35 to 1.53 in the other. As for their fellow eyes, ERM had been noted in two of them at enrollment.
Clinical characteristics of fellow eyes
Of the 52 fellow eyes in the study group, many had various macular diseases including ERM (27 eyes), macular hole (MH) (5 eyes), retinal vein occlusion (RVO) (5 eyes), retinal pigment epithelium detachment (4 eyes), choroidal neovascularization (3 eyes), central serous chorioretinopathy (2 eyes), choroidal hemangioma (1 eye), and polypoidal choroidal vasculopathy (1 eye). Eleven fellow eyes also had a wide-based foveal pit, including all fellow eyes without vitreoretinal disease (4 eyes). For the fellow eyes with ERM, the mean coefficient of RAT was 0.30, similar to that in the control group (0.35). On the other hand, the mean coefficient of RAT was 0.14 in the fellow eyes with MH and 0.21 in those with RVO, similar to that in eyes with a wide-based foveal pit (0.18) (Table 2).
Discussion
In this proof-of-principle study, we described a specific type of foveal shape: wide-based foveal pit. To define a wide-based foveal pit, we have enrolled 100 normal subjects to calculate the distribution of FBW in the normal population. Then we used the mean value plus one standard deviation as the cut-off point for the lower limit of FBW in a wide-based foveal pit. Because the contour of the foveal pit varies widely in the normal population, clinicians usually treat the wide-based foveal pit as a normal variant, especially as such eyes usually have normal vision without metamorphopsia. However, we found some of them developed idiopathic ERM later, and their fellow eyes either also had a wide-based foveal pit or had macular diseases including idiopathic ERM, MH, and RVO. Thus, we think that both eyes of the same individual might have had similar foveal contours originally [7], but later some of them evolved into having some macular disease. Rather than a normal variant, we hypothesize that the wide foveal base represents a pathological change that predisposes the eye to certain macular diseases.
The reported prevalence of ERM ranges 2–18% in general populations of different regions and ethnicities [8,9,10]. Age-stratified results revealed a higher prevalence of ERM formation in the elderly, with a prevalence ranging 15.1–35.7% in those older than 70 years [8, 10]. In our study group, the mean age was 63.2 years while the proportion of ERM in the fellow eyes was 51.9%, a rate much higher than that in the general population. The prevalence of MH in the fellow eyes (9.6%) was also much higher than that in the normal population (0.02–0.8%) according to several large population-based studies [9, 11]. Although our study did not include the general population, such results still suggest some correlation between wide-based foveal pit and these diseases. Furthermore, we also found that females predominated in eyes with a wide-based foveal pit (82.7% female vs. 17.3% male), which is an interesting finding because females also reportedly predominate in cases of idiopathic ERM, MH, and RVO [12,13,14]. This result implies that the macula of females may have characteristics that act as common predisposing factors for wide-based foveal pit and certain macular diseases including idiopathic ERM, MH and RVO.
Eyes with a wide-based foveal pit had not only a large FAZ but also a wide RAT. This result implies that some centrifugal force may exist in these eyes that results in both a wide foveal base and a wide RAT. The relationships among ERM, MH, wide RAT and a wide-based foveal pit are intriguing and closely related. Yoshihara et al. [6] reported an association of MH with a wider RAT. They believe that a tangential force may widen the major retinal vessels and the central foveal area. As a consequence, a wide RAT would result in the formation of MH. Our study results support their theory; we found an association of wide-based foveal pit with a wide RAT, and that fellow eyes had a predisposition to MH. We propose that the tangential centrifugal force on the vitreomacular interface will exert tangential traction on the retinal arcade vessels and lead to the widening of RAT; it will also exert tangential traction on the central macula, which will widen the foveal base. Over time, the centrifugal force continues to drag the macula and MH may eventually develop.
ERM is composed of glia, fibrocytes, myofibrocytes, retinal pigment epithelium, and sometimes hyalocytes [15]. Two types of pathogenesis for ERM have been proposed: one states that ERM comes from cellular growth and collagen deposition along the cleft of the ILM; and the other states that ERM develops along the posterior scaffold of the hyaloid membrane, so that ERM can be detected in eyes with either a detached or attached posterior hyaloid [16,17,18]. Our study results support the former type of pathogenesis for ERM. We propose that, in eyes with a wide-based foveal pit and a wide RAT, the centrifugal force on the macular surface may also disrupt the ILM over the macula, which results in trivial and clinically undetectable ILM deficits. Such deficits may then give rise to glial cell proliferation and ERM formation. After its formation, the contractile characteristic of ERM will result in a centripetal force on the macula, which will narrow the RAT. We observed this result in our finding that three eyes with a wide-based foveal pit developed ERM during the follow-up period and, as we expected, the RAT was narrowed after the formation of ERM. According to the above findings, we further propose that ERM formation may act as a natural protection mechanism against MH formation in eyes with centrifugal traction on the macula. In the absence of ERM formation over the fovea in eyes with a wide-based foveal pit, the centrifugal force may persist and MH may eventually develop. Our study results support this assertion in that the fellow eyes with MH had a similar RAT as the eyes with a wide-based foveal pit, while the fellow eyes with ERM had a much narrower RAT. We will continue to follow the patients with a wide-based foveal pit to monitor for any subsequent MH formation or more ERM formation.
In this study, we used the en face OCTA images to measure the area of FAZ. We measured from the ILM to the outer plexiform layer, including the superficial, intermediate, and deep retinal capillary plexus in normal structures. We found that the mean FAZ was significantly different among eyes with a wide-based foveal pit, those with different diseases, and those of normal controls. Eyes with ERM had the smallest FAZ, while those with MH or RVO had a larger FAZ, which was similar to the eyes with a wide-based foveal pit. Previous studies have demonstrated that during ocular development, the formation of the FAZ precedes the formation of the foveal pit [19, 20]. The model of foveal pit development suggests that intraocular pressure and retinal stretching during ocular growth will widen the foveal pit. Having less retinal tissue, the FAZ is more susceptible to further stretching than is the vascularized retina, and it is therefore more deformable. Thus, a larger FAZ was usually associated with a wider and thinner fovea [21, 22]. These findings further supported our proposal that a large centrifugal stretching force during ocular development will result in RAT widening, FAZ enlargement, and the subsequent widening of the foveal pit. As time progresses, MH may then develop; otherwise, glial proliferation and ERM formation may be induced with subsequent narrowing of the RAT and FAZ, which may protect against MH formation.
If our hypothesis about the centrifugal force at macula stands, other characteristics of the foveal pit may also be involved, such as the slope or the radius, etc. However, we only measured the FBW and area of FAZ in this study because they are more easily measured and understood. Several methods have been proposed to define the foveal contour [4, 5, 7], but they are rather complicated and none of them have been recognized as the standard for foveal contour measurement. Further studies are needed to discover new parameters of foveal contour and to explore their relationships with macular structural diseases.
In addition to ERM and MH, we also found an association of wide-based foveal pit with RVO in the fellow eyes. It has been reported that patients with unilateral RVO had enlarged FAZs in both the RVO eye and the non-RVO eye, when compared with normal controls [23]. The authors proposed that the eyes without RVO may also have parafoveal capillary dropout, which resulted in FAZ enlargement. However, our study results indicate a possible association of RVO with widening of the foveal pit and anatomical FAZ enlargement, not capillary dropout in the fellow eye. Further studies are needed to elucidate the underlying mechanism for the association between wide-based foveal pit and RVO.
The major limitation of this study is that this is not a population-based study. We collected cases of the study group as well as the control group from patients who visited our clinic for various reasons, and this selection process may have resulted in selection bias and overestimation of the prevalence of macular diseases in the fellow eyes. However, many of the cases with wide-based foveal pit in this study were found during routine OCT examination before refractive surgery or cataract surgery, which made the study population not limited to diseased people. Besides, this is a cross-sectional study, so that is why we do not claim the prevalence, but only report a potential predisposition to certain associated diseases. Further population-based longitudinal studies are needed to examine our findings and demonstrate our hypothesis. Nevertheless, the strength of this study is that the cases in the control group were matched to those in the study group by age and sex, and all cases were of Chinese ethnicity. In this way the confounding effect of age, sex and race could be reduced.
In conclusion, we described the anatomical and clinical characteristics of a special type of foveal contour, the wide-based foveal pit. Eyes with a wide-based foveal pit also had a large FAZ and a wide RAT, and females dominated in these subjects. Some eyes with a wide-based foveal pit developed idiopathic ERM at the follow-up examinations. The fellow eyes, in addition, had a predisposition to epiretinal membrane and macular hole. We propose that the anatomical characteristics of wide-based foveal pit are associated with the formation of idiopathic ERM and MH.
Data availability
Yi-Ting Hsieh had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. The data can be made available upon formal request.
References
Yuodelis C, Hendrickson A (1986) A qualitative and quantitative analysis of the human fovea during development. Vision Res 26:847–855
Wagner-Schuman M, Dubis AM, Nordgren RN, Lei Y, Odell D, Chiao H, Weh E, Fischer W, Sulai Y, Dubra A, Carroll J (2011) Race- and sex-related differences in retinal thickness and foveal pit morphology. Invest Ophthalmol Vis Sci 52:625–634. https://doi.org/10.1167/iovs.10-5886
Dubis AM, McAllister JT, Carroll J (2009) Reconstructing foveal pit morphology from optical coherence tomography imaging. Br J Ophthalmol 93:1223–1227. https://doi.org/10.1136/bjo.2008.150110
Liu L, Marsh-Tootle W, Harb EN, Hou W, Zhang Q, Anderson HA, Norton TT, Weise KK, Gwiazda JE, Hyman L, Group C (2016) A sloped piecemeal Gaussian model for characterising foveal pit shape. Ophthalmic Physiol Opt 36:615–631. https://doi.org/10.1111/opo.12321
Moore BA, Yoo I, Tyrrell LP, Benes B, Fernandez-Juricic E (2016) FOVEA: a new program to standardize the measurement of foveal pit morphology. PeerJ 4:e1785. https://doi.org/10.7717/peerj.1785
Yoshihara N, Sakamoto T, Yamashita T, Yamashita T, Yamakiri K, Sonoda S, Ishibashi T (2015) Wider retinal artery trajectories in eyes with macular hole than in fellow eyes of patients with unilateral idiopathic macular hole. PLoS One 10:e0122876. https://doi.org/10.1371/journal.pone.0122876
Scheibe P, Zocher MT, Francke M, Rauscher FG (2016) Analysis of foveal characteristics and their asymmetries in the normal population. Exp Eye Res 148:1–11. https://doi.org/10.1016/j.exer.2016.05.013
Fraser-Bell S, Ying-Lai M, Klein R, Varma R, Los Angeles Latino Eye S (2004) Prevalence and associations of epiretinal membranes in latinos: the Los Angeles Latino Eye Study. Invest Ophthalmol Vis Sci 45:1732–1736
Klein R, Klein BE, Wang Q, Moss SE (1994) The epidemiology of epiretinal membranes. Trans Am Ophthalmol Soc 92:403–425 discussion 425-430
McCarty DJ, Mukesh BN, Chikani V, Wang JJ, Mitchell P, Taylor HR, McCarty CA (2005) Prevalence and associations of epiretinal membranes in the visual impairment project. Am J Ophthalmol 140:288–294. https://doi.org/10.1016/j.ajo.2005.03.032
Rahmani B, Tielsch JM, Katz J, Gottsch J, Quigley H, Javitt J, Sommer A (1996) The cause-specific prevalence of visual impairment in an urban population-the Baltimore Eye Survey. Ophthalmology 103: 1721-1726. Doi https://doi.org/10.1016/S0161-6420(96)30435-1
McCannel CA, Ensminger JL, Diehl NN, Hodge DN (2009) Population-based incidence of macular holes. Ophthalmology 116:1366–1369. https://doi.org/10.1016/j.ophtha.2009.01.052
Xiao W, Chen X, Yan W, Zhu Z, He M (2017) Prevalence and risk factors of epiretinal membranes: a systematic review and meta-analysis of population-based studies. BMJ Open 7:e014644. https://doi.org/10.1136/bmjopen-2016-014644
Park SJ, Choi NK, Park KH, Woo SJ (2014) Nationwide incidence of clinically diagnosed retinal vein occlusion in Korea, 2008 through 2011: preponderance of women and the impact of aging. Ophthalmology 121:1274–1280. https://doi.org/10.1016/j.ophtha.2013.12.024
Kampik A, Kenyon KR, Michels RG, Green WR, de la Cruz ZC (1981) Epiretinal and vitreous membranes. Comparative study of 56 cases. Arch Ophthalmol 99:1445–1454
Kishi S, Shimizu K (1994) Oval defect in detached posterior hyaloid membrane in idiopathic preretinal macular fibrosis. Am J Ophthalmol 118:451–456
Snead DR, James S, Snead MP (2008) Pathological changes in the vitreoretinal junction 1: epiretinal membrane formation. Eye (Lond) 22:1310–1317. https://doi.org/10.1038/eye.2008.36
Bovey EH, Uffer S (2008) Tearing and folding of the retinal internal limiting membrane associated with macular epiretinal membrane. Retina 28:433–440. https://doi.org/10.1097/IAE.0b013e318150d6cf
Provis JM, Sandercoe T, Hendrickson AE (2000) Astrocytes and blood vessels define the foveal rim during primate retinal development. Invest Ophthalmol Vis Sci 41:2827–2836
Springer AD, Hendrickson AE (2005) Development of the primate area of high acuity, 3: temporal relationships between pit formation, retinal elongation and cone packing. Vis Neurosci 22:171–185. https://doi.org/10.1017/S095252380522206X
Chui TY, Zhong Z, Song H, Burns SA (2012) Foveal avascular zone and its relationship to foveal pit shape. Optom Vis Sci 89:602–610. https://doi.org/10.1097/OPX.0b013e3182504227
Dubis AM, Hansen BR, Cooper RF, Beringer J, Dubra A, Carroll J (2012) Relationship between the foveal avascular zone and foveal pit morphology. Invest Ophthalmol Vis Sci 53:1628–1636. https://doi.org/10.1167/iovs.11-8488
Adhi M, Filho MA, Louzada RN, Kuehlewein L, de Carlo TE, Baumal CR, Witkin AJ, Sadda SR, Sarraf D, Reichel E, Duker JS, Waheed NK (2016) Retinal capillary network and foveal avascular zone in eyes with vein occlusion and fellow eyes analyzed with optical coherence tomography angiography. Invest Ophthalmol Vis Sci 57:OCT486–OCT494. https://doi.org/10.1167/iovs.15-18907
Code availability
ImageJ (version 1.47, National Institutes of Health, Bethesda, MD, USA; available at: http://imagej.nih.gov/ij/) was used for image analysis.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by I-Hsin Ma and Yi-Ting Hsieh. The first draft of the manuscript was written by I-Hsin Ma and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Ethics Committee and Institutional Review Board of National Taiwan University Hospital (No.: 201908068RINC) and adhered to the Declaration of Helsinki. Informed consent is waived due to the retrospective nature of the study and no identifiable details were present.
Consent for publication
Informed consent is waived due to the retrospective nature of the study and no identifiable details were present.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Ma, IH., Yang, CM. & Hsieh, YT. Wide-based foveal pit: a predisposition to idiopathic epiretinal membrane. Graefes Arch Clin Exp Ophthalmol 259, 2095–2102 (2021). https://doi.org/10.1007/s00417-021-05092-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00417-021-05092-5