
Abstract
Background
To ascertain the morphological changes in the edge structure of femtosecond laser-derived capsulotomy specimens using varying patient interfaces and different laser pulse energies.
Methods
In this experimental clinical study femtosecond laser-assisted capsulotomies were performed in 30 eyes using the LenSx femtosecond laser (LenSx, Alcon, Fort Worth, TX, USA). Surgery was performed using either a rigid curved contact interface (group 1, 15 eyes) or a curved interface with a soft contact lens between cornea and interface (group 2, 15 eyes). The laser pulse-energy was set to 15 μJ in group 1 and to 5 μJ in group 2. After the removal of the anterior capsule, half of the specimens from each group underwent either further staining for light microscopy (LM) or scanning electron microscopy (SEM). Cell configuration, capsule shape, and edge abnormalities were analysed on a morphological basis.
Results
LM showed continuous anterior capsular incisions with a prominent demarcation line along the cutting edge, as well as tags and bridges, which were more pronounced in group 1. SEM revealed further smaller microgrooves and sawtooth patterns in both groups, and a more regular demarcation line configuration in group 2.
Conclusion
A soft contact lens interface with a subsequent laser pulse energy of 5 μJ resulted in fewer tags and bridges, smoother edges, and a more regular and thinner demarcation line on specimens edges of femtosecond laser-performed capsulotomies compared to a rigid curved 15 μJ interface application.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Several studies on cataract and refractive lens-based surgery have demonstrated that femtosecond laser-assisted capsulotomies have precise, predictable, and repeatable dimensions, and superior centration, and furthermore improve the safety of hydrodissection, nuclear fragmentation, and cortical clean-up compared to manually performed capsulotomies [2, 9, 10]. This can potentially optimize the refractive predictability and thus the optical performance of intraocular lenses [6, 7].
Friedman et al. previously demonstrated that decreasing laser pulse energy leads to an increase in the strength of capsulotomies [3]. Furthermore, their scanning electron microscopy (SEM) analyses describe the appearance of microgrooves on the capsule edges produced by the laser. We have already demonstrated in a previous study that femtosecond laser-assisted capsulotomies show a prominent demarcation line, probably due to the laser pulse energy. This hypothesis was substantiated by the fact that in manually performed anterior capsulotomies no such demarcation line was observed [8].
Therefore, the purpose of this study is to evaluate morphological changes on the microanatomical level in femtosecond laser-derived anterior human lens capsulotomy specimens after using two different patient interfaces and different laser pulse energy settings.
Methods
The experimental study was approved by the ethics committee of the Goethe-University, Frankfurt am Main, Germany, and was conducted according to the Declaration of Helsinki. Thirty capsulotomy specimens were collected during femtosecond laser-assisted cataract surgery. Only completely extracted and mounted specimens were used for the experimental study. The femtosecond laser capsulotomy procedures were performed using the LenSx laser (Alcon Laboratories Inc., Fort Worth, TX, USA) under topical anaesthesia with Conjucain (oxybuprocainhydrochloride, 4.0 mg/ml) EDO eye drops (Dr. Mann Pharma GmbH, Berlin, Germany) by the same surgeon (TK). The LenSx laser is a 50 kHz femtosecond infrared laser with a pulse width of 600–800 fs, a central laser wavelength of 1,030 nm and a maximum pulse energy of 15 μJ. Laser pulse energy settings for performing the anterior capsulotomies were 15 μJ in 15 eyes (group 1) and 5 μJ in 15 eyes (group 2). The depth and coordinates of the capsulotomies were determined by the laser system’s live optical coherence tomography (OCT). In both groups, the diameter of the capsulotomy was set to 5 mm.
The patient interface in group 1 consisted of a curved applanation lens, suction ring, and tubing. The 5 μJ capsulotomies (group 2) were performed with an updated interface using an extended suction skirt and an additional soft contact lens between the applanation lens and the cornea, which allows for a decrease of laser pulse energy while maintaining the ability to perform capsulotomies (Fig. 1). The recommended manufacturer’s specification for this interface setting in regards to the laser pulse energy is 5 μJ. It is noteworthy that the applanation lenses for both interfaces have a diameter of 10.8 mm and a curvature of 8.3 mm (no change in specifications). After docking was performed in both groups, the cornea was applanated and suction was activated. After laser treatment, undocking was performed and the interface was removed. In group 2, the contact lens was also removed after the laser procedure before continuing surgery.

Interface and soft contact lens, which is put on the interface’s surface for applanation in study group 2
Histological analyses
All specimens were immediately fixated in 4.5 % formalin after anterior capsule extraction. For light microscopy (LM) Masson Goldner trichrome staining was performed in anterior capsule specimens as previously described by our study group [8]. Briefly, all the specimens were deparaffinised, rehydrated in alcohol, differentiated in phosphomolybdic–phosphotungstic and acetic acid, washed in distilled water, and finally embedded in xylole. Images of stained specimens were captured and analysed with the Leica/Reichert Univar Microscope with Leica DFC 280 Camera System (Leica Microsystems Imaging Solutions Ltd., UK) using different magnifications.
Scanning electron microscopy (SEM)
SEM images of the complete capsulotomies were captured with the Hitachi S-500 SEM (Hitachi High-Technologies Corporation, Japan) after fixation, with a further focus on four randomized areas within all specimens. To perform SEM, all specimens were coated with 25 nm of gold and examined with the scanning electron microscope at 30 KV. An experienced cataract surgeon (TK) evaluated the morphological behaviour of the cut edges.
Results
The femtosecond laser performed capsulotomies were uneventful in both groups. No visible tears or incomplete procedures were documented.
Group 1, 15 μJ
The mean time to create capsulotomies in group one was 2.5 (± 0.6) seconds. Intraoperative OCT showed visible folds in the posterior corneal surface during interface suction. In LM, irregularities of the cell’s configuration with partly destroyed nuclei were observed in the peripheral part of the anterior capsule. The demarcation line seen in this group had a width of between 30 and 80 μm, with some foothills up to 200 μm (Fig. 2a and b). Furthermore, the capsulotomies showed multiple tags, bridges, and stray impressions, even at some distance away from the cutting edge. The tags had variable distances (Fig. 3). Sawtooth patterns and microgrooves could be seen with increasing magnifications (Fig. 4).

a,b Demarcation line along the cutting edge of the femtosecond laser acquired capsulotomies using 15 μJ with partially high dimensions. Light microscopy, 10× (a) and 20× (b) magnification, Masson Goldner trichrome staining

Visible laser spots with straying and tags along the cutting edge using 15 μJ. Light microscopy, 20× magnification, Masson Goldner trichrome staining

Cellular irregularities and sawtooth pattern along the cutting edge using 15 μJ. Light microscopy, 20× magnification, Masson Goldner trichrome staining
In SEM analyses, edges with a sawtooth pattern and microgrooves were observed. Individual capsule fibers could not be identified (Fig. 5). At 10,000× magnification, frayed tissue was clearly visible. Here a “valleys and mountains” configuration could be seen. Tags were clearly visible on multiple spots along the cut (Fig. 6).

Tissue-destroying process of the femtosecond laser with visible demarcation line using 15 μJ. Scanning electron microscopy, 3,000× magnification

Tissue-destroying process of the femtosecond laser with distinctive sawtooth pattern but no fibers visible using 15 μJ. Scanning electron microscopy, 10,000× magnification
Group 2, 5 μJ
The mean time to create capsulotomies in group 2 was 2.7 (± 0.5) seconds. OCT showed no visible posterior corneal folds during interface suction. In LM analyses, the mentioned demarcation line was also observed but in smaller dimensions without outliers (<40 μm, Fig. 7a and b). By using a lower energy setting, specimens showed slightly different findings in the SEM analysis as observed in group 1. The edges still had irregularities and tags, but these were distinctly lower than those created by the higher laser pulse energy settings (Fig. 8). After increasing the magnification scale, edges were subjectively smoother and individual fibers were visible. When using a magnification of 10,000×, differences between the “highest and lowest” points in the valleys and mountains were not as large as those seen in the 15-μJ group. Interestingly, even the sawtooth pattern wasn’t as distinct as in group 1 (Fig. 9).

a,b Demarcation line with smaller expansions along the cutting edge of the femtosecond laser acquired capsulotomies using 5 μJ. Light microscopy, 20× magnification (a, b), Masson Goldner trichrome staining

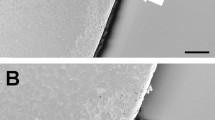
Tissue-destroying process of the femtosecond laser with a smoother cutting line and no sawtooth pattern or fibers visible using 5 μJ. Scanning electron microscopy, 1,000× magnification

Tissue-destroying process with a smoother cutting line femtosecond laser using 5 μJ. Scanning electron microscopy, 10,000× magnification
Discussion
Analyses of femtosecond laser lens surgery have been, up to now, mainly focused on clinical outcomes or on the macroscopic shape and centration of capsulorhexes as well as the postoperative capsular bag tensile strengths [1, 3, 5–7, 11]. The present experimental study evaluates the microanatomical structure of femtosecond laser-performed capsulotomies using different laser energy pulse settings.
Tags and bridges can occur as a result of minimal torsional movements of the eye, even with the eye fixated by the limbal–conjunctival suction of the patient interface used within the laser platform. Talamo et al. recently described changes between two interfaces, and stated that curved contact interfaces can lead to incomplete capsulotomy during laser cataract surgery [12]. They showed that eye drifts were lower when using a liquid optical immersion interface.
As previously pointed out, the design of the patient interface could be a reason for the tissue damage in the anterior capsule, with consecutive further damage to surrounding structures during femtosecond laser-assisted lens surgery [4, 8]. The most likely reason for the straying is the design of the patient interface itself [4, 12]. In our trial, two different interfaces were used: a rigid curved patient interface which directly applanates the cornea (group 1), and a curved interface using a soft contact lens between the interface and the corneal surface. In group 1, corneal folds were observed when pressing the cornea against the rigid surface. Such folds may not affect the laser focusing inside the stroma, which is why this effect should not be a significant issue when corneal cuts are performed. However, because the beam is focused several millimeters posterior to the cornea in femtosecond laser-assisted lens surgery, the effect of the corneal folds might be important. A possible result of this could be damage to the surrounding structures in the patient’s eye, such as iris micro-injuries in small pupils. By using an modified patient interface (group 2, 5 μJ) in our study, no posterior corneal folds were visible in intraoperative OCT. Laser pulse energy settings were set according to the manufacturer’s advice for clinical application: 15 μJ for the interface without soft contact lens, and 5 μJ for the interface with soft contact lens respectively.
Our fine structural analysis showed, in both settings, a certain amount of straying of the laser spots, as well as tags and bridges at the edges of the capsulotomies and a demarcation line along the cut which indeed confirms the effect of the laser on the surrounding tissue as recently described by our study group [8]. By using a lower laser pulse energy and a soft contact lens supported interface, the demarcation line and, therefore, the impact on surrounding tissue could be reduced.
This demarcation line could be the result of the expanding cavitation bubbles that might lead to the displacement of cells and the destruction of cell nuclei close to the cutting edge, and might also have an effect on capsulotomy strength. Interestingly, the use of a lower energy setting (5 μJ) still showed a demarcation line, but with smaller expansions. Furthermore, a more regular shape with slightly smoother edges was documented using 5 μJ. Friedman and Palanker also showed that reducing the laser pulse energy levels could lead to a stronger capsulotomy [3, 9].
The work of Trivedi demonstrates that the manual technique produces the most extensible capsulotomy [13], whereas Auffarth described that femtosecond laser-assisted capsulotomy resulted in a significantly stronger anterior capsule opening than the standard manually performed ones [1]. All of these studies were performed using a porcine model. Our aim was not to focus on capsulotomy strength but on microanatomical changes. In our human experimental setting, two different energy pulse levels were used, with slightly different morphological outcomes.
Femtosecond laser technology is constantly improving, and seems to be a promising and safe procedure in refractive and cataract lens surgery. Nevertheless, some side-effects from the laser beams on the human tissue have to be considered when recommending this procedure.
Further studies looking at the relationship between laser pulse energy, spot size, and the different patient interface designs and, on the other hand, the long-term analysis of human capsular bags after IOL implantations, will help to better elucidate the optimal parameters for laser capsulotomy creation and the effect on posterior capsule opacification following femtosecond laser application to the human lens.
References
Auffarth GU, Reddy KP, Ritter R, Holzer MP, Rabsilber TM (2013) Comparison of the maximum applicable stretch force after femtosecond laser-assisted and manual anterior capsulotomy. J Cataract Refract Surg 39:105–109
Bali SJ, Hodge C, Lawless M, Roberts TV, Sutton G (2012) Early experience with the femtosecond laser for cataract surgery. Ophthalmology 119:891–899
Friedman NJ, Palanker DV, Schuele G, Andersen D, Marcellino G, Seibel BS, Batlle J, Feliz R, Talamo JH, Blumenkranz MS, Culbertson WW (2011) Femtosecond laser capsulotomy. J Cataract Refract Surg 37:1189–1198
Kohnen T (2013) Interface for femtosecond laser-assisted lens surgery. J Cataract Refract Surg 39:491–492
Kranitz K, Mihaltz K, Sandor GL, Takacs A, Knorz MC, Nagy ZZ (2012) Intraocular lens tilt and decentration measured by Scheimpflug camera following manual or femtosecond laser-created continuous circular capsulotomy. J Refract Surg 28:259–263
Lawless M, Bali SJ, Hodge C, Roberts TV, Chan C, Sutton G (2012) Outcomes of femtosecond laser cataract surgery with a diffractive multifocal intraocular lens. J Refract Surg 28:859–864
Nagy ZZ (2012) Advanced technology IOLs in cataract surgery: pearls for successful femtosecond cataract surgery. Int Ophthalmol Clin 52:103–114
Ostovic M, Klaproth OK, Hengerer FH, Mayer WJ, Kohnen T (2013) Light microscopy and scanning electron microscopy analysis of rigid curved interface femtosecond laser-assisted and manual anterior capsulotomy. J Cataract Refract Surg 39:1587–1592
Palanker DV, Blumenkranz MS, Andersen D, Wiltberger M, Marcellino G, Gooding P, Angeley D, Schuele G, Woodley B, Simoneau M, Friedman NJ, Seibel B, Batlle J, Feliz R, Talamo J, Culbertson W (2010) Femtosecond laser-assisted cataract surgery with integrated optical coherence tomography. Sci Transl Med 2:58ra85
Roberts TV, Lawless M, Bali SJ, Hodge C, Sutton G (2013) Surgical outcomes and safety of femtosecond laser cataract surgery: a prospective study of 1500 consecutive cases. Ophthalmology 120:227–233
Szigeti A, Kranitz K, Takacs AI, Mihaltz K, Knorz MC, Nagy ZZ (2012) Comparison of long-term visual outcome and IOL position with a single-optic accommodating IOL after 5.5- or 6.0-mm femtosecond laser capsulotomy. J Refract Surg 28:609–613
Talamo JH, Gooding P, Angeley D, Culbertson WW, Schuele G, Andersen D, Marcellino G, Essock-Burns E, Batlle J, Feliz R, Friedman NJ, Palanker D (2013) Optical patient interface in femtosecond laser-assisted cataract surgery: contact corneal applanation versus liquid immersion. J Cataract Refract Surg 39:501–510
Trivedi RH, Wilson ME Jr, Bartholomew LR (2006) Extensibility and scanning electron microscopy evaluation of 5 pediatric anterior capsulotomy techniques in a porcine model. J Cataract Refract Surg 32:1206–1213
Financial disclosure
Oliver Klaproth received travel reimbursements and/or lecture fees from the following companies: Alcon, Rayner and Oculus.
Thomas Kohnen received travel reimbursements, grant support and/or lecture fees from the following companies: Alcon, Abbott, Bausch & Lomb, Carl Zeiss Meditec, Neoptics, Rayner, Schwind. He is consultant to Alcon, Carl Zeiss Meditec, Diomed, Rayner, and Schwind.
Conflict of interest
All authors certify that there exists no actual or potential conflict of interest in relation to this article.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kohnen, T., Klaproth, O.K., Ostovic, M. et al. Morphological changes in the edge structures following femtosecond laser capsulotomy with varied patient interfaces and different energy settings. Graefes Arch Clin Exp Ophthalmol 252, 293–298 (2014). https://doi.org/10.1007/s00417-013-2547-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00417-013-2547-5