
Abstract
Purpose
The purpose of this study is to investigate optic nerve head using spectral domain optical coherence tomography (SD-OCT) in children with large cupping.
Methods
111 eyes (4–10 years) were divided into three groups according to the cup to disc ratio: group 1, ≤0.3; group 2, 0.4–0.6; and group 3, ≥0.7. The rim area, disc area, average cup to disc ratio, vertical cup to disc ratio, and cup volume were investigated using SD-OCT (Cirrus HD-OCT, Carl Zeiss, Jena, Germany), and the axial length and anterior chamber depth (ACD) were measured by IOL master (IOL master 500, Carl Zeiss, Jena, Germany). Next, we compared ocular biometry and SD-OCT between the three groups.
Results
The mean age of group1 was 6.48 ± 1.42 years, 7.00 ± 1.75 years in group 2, and 6.63 ± 1.82 years in group 3 (p = 0.370). A significant difference was seen in the spherical equivalent between the groups (p = 0.001). Group 2 had the most myopic refractive errors. As the cup to disc ratio increases, disc area, average cup to disc ratio, vertical cup to disc ratio, and cup volume increase significantly. When the results of ocular biometry and SD-OCT are adjusted for axial length, only disc area showed a significant correlation with cup to disc ratio (ACD: p = 0.473, rim area: p = 0.639, disc area: p = 0.005, and cup volume: p = 0.325).
Conclusion
Axial length is the key factor determining disc size, which in turn is important for determining cup to disc ratio. Normal children with large cupping should be examined for axial length, myopic refractive errors, and disc size.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Glaucoma causes progressive visual field loss and is a cause of irreversible blindness. Various examinations, such as tonometry, optic disc photography, visual field test, retinal nerve fiber layer (RNFL) photography, and RNFL analysis can be used to diagnose glaucoma. Early glaucoma is detected by careful examination, including RNFL photography, visual field tests, and optic disc photography; however, it is not easy to perform these visual field tests in children. Thus, cup to disc ratio using optic disc photography or a direct ophthalmoscope is important for diagnosing pediatric glaucoma. It is difficult to diagnose pediatric glaucoma in children with large cupping and normal intraocular pressure. RNFL analysis using optical coherence tomography is regarded as a sensitive diagnostic test for the diagnosis of juvenile glaucoma [1].
Optic disc morphology is influenced by several factors, including axial length, race, and age. Black children have larger RNFL thickness and larger cup to disc area ratio compared to white children [2]. Optic discs with larger vertical diameters have considerably greater vertical cup to disc ratio [3]. Although changes associated with aging may be one of the factors influencing cup to disc ratio, this influence is minimal [4]. Axial length is highly correlated with optic disc morphology; rim measurements decrease and cup measurements increase with increase in axial length [5].
In children, Huynh et al. [6] investigated optic disc parameters measured by time domain optical coherence tomography (OCT) and reported that axial length appeared to be a stronger determinant of disc and rim size than refraction, and optic disc area increased significantly with axial length. However, they did not exclude glaucoma suspect children with high intraocular pressure, retinal nerve fiber layer defect and pathologic disc cupping. Moreover, optic nerve head parameter measurements provided by time domain OCT and spectral domain OCT show significant differences and cannot be considered interchangeable [7]. Thus, we investigated ocular biometries using spectral domain OCT that could be related to cup to disc ratio in normal children with large cupping.
Materials and methods
Informed consent form was obtained from parents of the children, and this research study was reviewed and approved by the Institutional Review Board (IRB) of Kim’s Eye Hospital. Children (4–10 years) were prospectively enrolled from Kim’s Eye Hospital for this study. All children underwent full ophthalmologic examinations, including best corrected visual acuity, cycloplegic refraction, slit-lamp examination, alternate cover test, and careful fundus examination. Exclusion criteria included best corrected visual acuity worse than 20/25, intraocular pressure ≥21 mmHg, pathological disc and cup such as morning glory disc syndrome, optic nerve hypoplasia and tilted disc syndrome, abnormal findings on retinal nerve fiber layer (RNFL) photography, family history of glaucoma, abnormal prenatal history, abnormal developmental history and children who did not cooperate.
Optic disc photographs were taken using a Kowa nonmyd 7 fundus camera (Kowa, Tokyo, Japan) with a Nikon d70s digital camera (Nikon, Tokyo, Japan). All disc photographs were taken by experienced examiners. Optic disc images were captured using an image capture program provided by Kowa. Two specialists were enrolled to determine vertical cup to disc ratio. We used the average cup to disc ratio from the two observers, and cup to disc ratio measurement differences of >0.2 between the two observers were not included. Children were divided into three groups according to their cup to disc ratio: group 1: cup to disc ratio ≤0.3, group 2: 0.4–0.6, and group 3: ≥ 0.7. Ages of the three groups were matched.
Spherical equivalent (SE) was measured under cycloplegic refraction. Spectral domain optical coherence tomography (Cirrus HD-OCT, Carl Zeiss, Jena, Germany) and IOL master (IOL master 500, Carl Zeiss, Jena, Germany) were performed. Patients were scanned with Cirrus optical coherence tomography (OCT) (software ver. 5.0.1, Carl Zeiss Meditec). The OCT scans were performed with Fast RNFL thickness protocols using internal fixation. Spectral domain OCT gave RNFL thickness, rim area, disc area, average cup to disc ratio, vertical cup to disc ratio, and cup volume (Fig. 1). We only used data with a signal strength higher than 6. The optical biometries including axial length (mm) and anterior chamber depth (ACD) were obtained from the IOL master.

The optic disc analysis and retinal nerve fiber layer were measured by spectral domain optical coherence tomography. The result of a 7-year-old girl who had 0.8 cup to disc ratio under fundus examination was shown
Statistical analyses were performed using SPSS ver. 14.0. An analysis of variance (ANOVA) test was used to analyze statistical differences of ocular biometries between groups. The inter-group analysis was done using the Tukey post-hoc test. Analysis of covariance (ANCOVA) test was used to evaluate the difference between cup to disc ratio and ocular biometries in order to exclude the effect of axial length on ocular biometries. The correlation between the cup to disc ratio and ocular biometries was analyzed using Spearman’s nonparametric correlation.
Results
111 eyes of 56 children were enrolled in the study. Table 1 shows the group data. The mean age of the groups was 6.48 ± 1.42 years in group 1, 7.00 ± 1.75 years in group 2, and 6.63 ± 1.82 years in group 3 (p = 0.370). Significant difference was seen in the SE between the groups (p = 0.001) (Tables 1 and 2). Group 2 had the most myopic refractive errors; however, the difference between group 2 and 3 was not significant (p = 0.925, Tukey post-hoc test). According to refractive errors, axial length and ACD were shortest in group 1 (p < 0.0001). With respect to OCT measurement, no difference was seen in the RNFL thickness between the groups (p = 0.741). Disc area, meaning total disc size, was the smallest in group 1; however, rim area was the smallest in the group 3.
Biometry and OCT measurement
Cup to disc ratio significantly correlated with ocular biometries including axial length, spherical equivalent, and ACD. ACD was correlated with cup to disc ratio (r = 0.435, p < 0.001) Among the biometries, axial length and ACD showed a positive correlation with cup to disc ratio and SE revealed a negative correlation (Fig. 2).

The correlation between cup to disc ratio and ocular biometries including axial length (mm), spherical equivalent (diopter) and anterior chamber depth (mm)
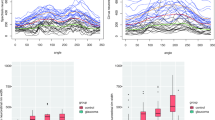
As cup to disc ratio increased, disc area, average cup to disc ratio, vertical cup to disc ratio, and cup volume also increased significantly. Only rim area had a negative correlation with cup to disc ratio. There were no correlations between average RNFL thickness and cup to disc ratio (p = 0.741) (Fig. 3). ANCOVA analysis was performed because the effect of axial length on cup to disc ratio was well-known. When the results of ocular biometry, except SE, were adjusted for axial length, only the disc area showed a significant correlation with cup to disc ratio (ACD: p = 0.473, rim area: p = 0.639, disc area: p = 0.005, and cup volume: p = 0.325)

The correlation between cup to disc ratio in the fundus photography and OCT parameters (average RNFL thickness (μm), rim area (mm2), disc area (mm2) and cup volume (mm3))
Discussion
This study revealed that children with large cupping tends to have a long axial length, more myopic refractive errors, small rim area, and large disc area with large cup volume.
The present study showed that children with large cupping have more myopic refractive errors than children with normal cupping. There is a controversy regarding the relationship between refractive errors and cup to disc ratio; Varma et al. [9] reported that refractive errors in black and white individuals were not associated with any significant differences in the size and topography of normal optic discs. However, a study of refractive errors on optic disc topographic parameters based on Asian Malay ethnic populations showed highly myopic eyes (SE < −6.0 diopters) had greater disc area, rim area, and rim volume, whereas hyperopic eyes (SE >0.5 diopters) had significantly smaller disc area, rim area, and cross-sectional RNFL area [9]. Wang’s study also suggested that highly hyperopic eyes have significantly smaller optic discs and highly myopic eyes have significantly larger optic discs than emmetropic eyes [10]. Therefore, there is racial difference with respect to the correlation between refractive errors and optic disc morphology. In the present study, ACD was highly correlated with cup to disc ratio (r = 0.435, p < 0.001) because ACD and axial length are highly correlated as measured by IOL master [11]. This correlation may occur in normal eyes.
In terms of OCT parameters, RNFL thickness was not significantly different between groups. Turk reported the average peripapillary RNFL thickness was 106.45 ± 9.41 μm and the RNFL thickness of children determined using OCT was not correlated with age, SE, or axial length [12]. Although the present results were slightly different than Turk’s results (from 97.08 ± 11.75 μm to 99.56 ± 9.27 μm), no correlation between RNFL thickness and axial length was observed in our study.
The cup to disc ratio can be primarily dependent on axial length. Savini et al. [13] reported that not only optic disc area but also rim area decreased with increase in axial length. However, Leung et al. [14] suggested that disc area increased with increase in axial length and negative SE on OCT measurement. In the present study, all parameters, including rim area, disc area, and cup volume were significantly different between the groups; however, there were no differences in the rim area and cup volume when the parameters were adjusted for axial length. Therefore, axial length could be the most important factor deciding cup size and we should consider axial length and SE for patients with large cupping. These relationships show the similarity to adult population [15]. SE is also the significant predictor of RNFL thickness [16].
Disc size is a major determinant of other disc parameters, and the size of both the rim and cup parameters are highly dependent on the disc size [17]. Cup area can be determined using disc area and rim area; the disc area is calculated by subtracting the rim area from cup area. Therefore, disc area may increases when rim area decreases or cup area increases. The present result corresponds well with the hypothesis demonstrating that cup size had a positive correlation with disc area (r = 0.483) and a negative correlation with rim area (r = −0.54). As a result, children with large cupping may relate to a large disc area and small rim area. Moreover, the disc area showed a significant positive correlation with horizontal cup disc ratio, vertical cup disc ratio, and cup disc area ratio [18]. Therefore, the cup to disc ratio increases with increase in the disc area. Our results also reveal a similar outcome where cup to disc ratio had a positive correlation with disc area.
In conclusion, when it comes to optic disc parameters using spectral domain OCT, axial length is a key factor determining disc size, which is an important factor for determining cup to disc ratio. When results are adjusted for axial length, only cup to disc ratio had a positive correlation with disc area. Therefore, normal children with large cupping should be reviewed for axial length, myopic refractive errors, and disc size.
References
Mrugacz M, Bakunowicz-Lazarczyk A (2005) Optical coherence tomography measurement of the retinal nerve fiber layer in normal and juvenile glaucomatous eyes. Ophthalmologica 219:80–85
El-Dairi M, Holgado S, Asrani S, Freedman SF (2011) Optical coherence tomography (OCT) measurements in black and white children with large cup-to-disc ratios. Exp Eye Res 93:299–307
Healey PR, Mitchell P, Smith W, Wang JJ (1997) Relationship between cup-disc ratio and optic disc diameter: the Blue Mountains Eye Study. Aust N Z J Ophthalmol 25(Suppl 1):S99–S101
Healey PR, Mitchell P, Smith W, Wang JJ (1997) The influence of age and intraocular pressure on the optic cup in a normal population. J Glaucoma 6:274–278
Rao HL, Kumar AU, Babu JG, Kumar A, Senthil S, Garudadri CS (2011) Predictors of normal optic nerve head, retinal nerve fiber layer, and macular parameters measured by spectral domain optical coherence tomography. Invest Ophthalmol Vis Sci 52:1103–1110
Huynh SC, Wang XY, Rochtchina E, Crowston JG, Mitchell P (2006) Distribution of optic disc parameters measured by OCT: findings from a population-based study of 6-year-old Australian children. Invest Ophthalmol Vis Sci 47:3276–3285
Savini G, Barboni P, Carbonelli M, Sbreglia A, Deluigi G, Parisi V (2012) Comparison of optic nerve head parameter measurements obtained by time-domain and spectral-domain optical coherence tomography. J Glaucoma. doi:10.1097/IJG.0b013e31824c9423
Varma R, Tielsch JM, Quigley HA, Hilton SC, Katz J, Spaeth GL, Sommer A (1994) Race-, age-, gender-, and refractive error-related differences in the normal optic disc. Arch Ophthalmol 112:1068–76
Wu RY, Wong TY, Zheng YF, Cheung CY, Perera SA, Saw SM, Aung T (2011) Influence of refractive error on optic disc topographic parameters: the singapore malay eye study. Am J Ophthalmol 152:81–86
Wang Y, Xu L, Zhang L, Yang H, Ma Y, Jonas JB (2006) Optic disc size in a population based study in northern China: the Beijing Eye Study. Br J Ophthalmol 90:353–356
Wissa AR, Wahba SS, Roshdy MM (2012) Agreement and relationship between ultrasonic and partial coherence interferometry measurements of axial length and anterior chamber depth. Clin Ophthalmol 6:193–198
Turk A, Ceylan OM, Arici C, Keskin S, Erdurman C, Durukan AH, Mutlu FM, Altinsoy HI (2012) Evaluation of the nerve fiber layer and macula in the eyes of healthy children using spectral-domain optical coherence tomography. Am J Ophthalmol 153:552–559
Savini G, Barboni P, Parisi V, Carbonelli M (2012) The influence of axial length on retinal nerve fibre layer thickness and optic-disc size measurements by spectral-domain OCT. Br J Ophthalmol 96:57–61
Leung CK, Cheng AC, Chong KK, Leung KS, Mohamed S, Lau CS, Cheung CY, Chu GC, Lai RY, Pang CC, Lam DS (2007) Optic disc measurements in myopia with optical coherence tomography and confocal scanning laser ophthalmoscopy. Invest Ophthalmol Vis Sci 48:3178–3183
Cheung CY, Chen D, Wong TY, Tham YC, Wu R, Zheng Y, Cheng CY, Saw SM, Baskaran M, Leung CK, Aung T (2011) Determinants of quantitative optic nerve measurements using spectral domain optical coherence tomography in a population-based sample of non-glaucomatous subjects. Invest Ophthalmol Vis Sci 52(13):9629–9635
Tsai DC, Huang N, Hwu JJ, Jueng RN, Chou P (2012) Estimating retinal nerve fiber layer thickness in normal schoolchildren with spectral-domain optical coherence tomography. Jpn J Ophthalmol 56(4):362–370
Moghimi S, Hosseini H, Riddle J, Lee GY, Bitrian E, Giaconi J, Caprioli J, Nouri-Mahdavi K (2012) Measurement of optic disc size and rim area with spectral-domain OCT and scanning laser ophthalmoscopy. Invest Ophthalmol Vis Sci 53(8):4519–4530
Mansoori T, Viswanath K, Balakrishna N (2011) Optic disc topography in normal Indian eyes using spectral domain optical coherence tomography. Indian J Ophthalmol 59:23–27
Financial interest
None of the authors have any proprietary/financial interest to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Jung, J.J., Baek, SH. & Kim, U.S. Biometry and spectral domain optical coherence tomography parameters in children with large cupping. Graefes Arch Clin Exp Ophthalmol 251, 2213–2217 (2013). https://doi.org/10.1007/s00417-013-2340-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00417-013-2340-5