
Abstract
Aim
To study the long-term visual result of photocoagulation of clinically significant macular edema (CSME) in diabetic patients in relation to baseline retinal vascular leakage assessed by vitreous fluorometry.
Methods
The study enrolled 36 eyes in 27 diabetic patients with CSME at baseline, all subsequently treated by photocoagulation. The diagnosis of CSME and treatment procedure followed the ETDRS criteria. The leakage through the retinal vessels was calculated as the blood–retinal barrier permeability. Five years after initial photocoagulation the patients were reexamined.
Results
The mean visual acuity decreased with 16 letters at follow-up, and in 15 eyes visual loss was substantial, with a decrease of 15 letters or more, corresponding to at least 3 lines. The baseline permeability was significantly higher in eyes with substantial visual loss than in eyes with more stable vision (14.2 nm/sec and 6.3 nm/sec respectively; p = 0.006), the corresponding odds ratio was 16.1 (95% CI: 1.8–146; p = 0.014). The level of retinopathy was significantly correlated to visual loss (Fisher’s exact test < 0.02).
Conclusion
Visual acuity decreased at follow-up, and a substantial visual loss of 3 or more lines in CSME was associated with higher retinal vascular leakage at baseline with an odds ratio of 16.1. For this relatively small sample, neither diabetes duration, age or HbA1c reached statistical significance, indicating that blood-retinal barrier permability is a strong predictor of the visual outcome. The results support the investigation of triamcinolone or VEGF inhibition in patients with severe leakage, and may help to identify patients in need for intravitreal injection.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
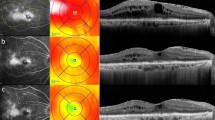
The severity of diabetic macular edema ranges from focal edema due to a few leaking microaneurisms to extensive leakage of retinal capillaries and breakdown of the blood-retinal barrier in the posterior pole [1, 2]. The Early Treatment of Diabetic Macular Edema Study (ETDRS) showed that photocoagulation is effective for clinically significantly diabetic macular edema (CSME) [3]. Thus funduscopic evaluation of the location and area of retinal thickening has become the principal guideline for intervention in clinical practice [4]. Later studies have used Optical Coherence Tomography (OCT) extensively both for quantitative and morphological evaluation [5, 6].
Due to lack of efficacy, in particular in severe diffuse edema, intravitreal injection of triamcinolone or VEGF inhibitors have been used in a number of smaller studies; both compounds have profound anti-permeability effects on the retinal vessels [6–10]. The future use of these agents awaits clinical trials and long-term experience, as recurrence is frequent and there is a risk of complications.
Fluorescein angiography, and to an increasing extent also retinal thickness measured by OCT, are used in clinical practice and in clinical studies. The focus on central retinal thickening with OCT does not take into account the large range of severity of the retinal edema, ranging from focal to diffuse and with or without intraretinal cysts and serous detachment [11]. In addition, changes in retinal thickness are probably not the most sensitive parameter, ignoring the basic feature of macular edema: the breakdown of the blood-retinal barrier.
Fluorescein leakage is an indicator of the tightness of the blood-retinal barrier, and the leakage can be quantified by vitreous fluorometry [12]. In a long-term follow-up of diabetic patients with mild edema at baseline, the blood-retinal barrier permeability was significantly increased in patients who progressed to photocoagulation compared to non-progressing patients, and the permeability was increased at least 1.5 years before the groups were different in retinal thickness as measured by OCT, indicating that permeability and retinal thickness do not follow the same time course and that permeability seems to be an early indicator of progression [13].
In our study, we have reevaluated fluorescein permeability as a prognostic factor for the long-term visual result after photocoagulation in patients with CSME at baseline.
Methods
Subjects
At baseline 61 eyes in 48 patients were enrolled, excluding eyes with edema graded to be less than CSME and also excluding eyes with vitreous liquification, as the blood-retinal barrier permeability cannot be calculated under this condition [14]. Baseline results from the study have been published earlier [15]. At follow-up 11 patients had died (14 eyes), three patients could not be located, and seven patients were unwilling to participate, mainly due to health problems. Age-related macular degeneration led to exclusion of one eye, leaving 36 eyes (27 patients) for follow-up. Mean follow-up was 5.5 years (range 3.6–7.75 years). At follow-up, visual acuity was performed using the ETDRS chart; vitreous fluorometry was possible in 22 eyes.
The study population at follow-up consisted of eight women and 19 men, of whom five had type I diabetes and 22 had type II diabetes.
Informed consent was obtained from all patients prior to entering the study, which was conducted according to the ICH-Guidelines for Good Clinical Practice (ICH GCP) and approved by the regional medical ethics committee.
Study design
A longitudinal study of the long-term result of macular photocoagulation for CSME to analyse the predictive value of blood-retinal barrier permeability on visual acuity.
Blood-retinal barrier permeability
Using vitreous fluorometry, the leakage of fluorescein into the vitreous was measured with a fluorometer (Ocumetric, Mountain View, CA, USA) at 30 and 60 minutes after fluorescein injection as described earlier. In brief, the permeability of the blood-retinal barrier was calculated after correction for light loss in the lens, plasma concentration of fluorescein and the diffusion coefficient for fluorescein in the vitreous [12, 14]. In healthy controls the permeability is 2 nm/sec [14, 16]. Vitreous liquefaction or posterior vitreous liquefaction interferes with the calculation of blood-retinal barrier permeability, and such eyes were excluded from the procedure [14].
Statistics
The change in visual acuity from baseline to follow-up was dichotomized to stable or substantial visual loss, the latter being defined as a loss of 15 letters or more on the ETDRS chart. If no other test is mentioned, the appropriate t-test was used to compare variables between groups. Blood-retinal barrier permeability was log-transformed for statistical analysis; results are given as back-transformed values. Due to the relatively small sample, the tests were repeated with non-parametric tests, leading to the same conclusion. The effect of covariates and calculation of odds ratio were performed with logistic regression. Data analysis was made using the SAS software package, version 8e (SAS Institute, Cary, NC, USA). The level of statistical significance for all tests was set at 5%.
Results
At baseline, the mean age of the patients was 58 years and the mean follow-up was 5.5 years (Table 1). The visual acuity at baseline was 78 ETDRS letters (snellen equivalent 0.8) decreasing to a mean 62 letters (Snellen equivalent 0.5) at late follow-up; one of the patients was blind (Table 2). In 15 out of 36 eyes the visual acuity at follow-up had declined substantially, and a loss of 15 letters or more (at least 3 lines) was found. The mean blood-retinal barrier permeability at baseline was 8.98 nm/sec (n = 36; range 1.55 to 60.11, Table 2).
The development of visual loss was associated with baseline permeability, as eyes with visual loss of 3 lines or more had a baseline permeability twice that of eyes without substantial visual loss (14.22 vs 6.27 nm/sec respectively, p = 0.006). In a logistic regression model, the possible influence of baseline covariates was tested; however, neither age, duration, HbA1c, baseline acuity or blood-pressure were significant, and the logistic regression confirmed the significant influence of baseline permeability with an odds ratio of 16.1 (Wald 95% confidence interval from 1.8 to 146, p = 0.014).
Baseline retinopathy was significantly larger in eyes with substantial visual loss (p < 0.02 Fisher’s exact test).
The blood-retinal barrier at follow-up was available in 22 eyes. The baseline permeability of these 22 eyes were 7.48 (95% confidence interval from 6.5 to 12.0), at follow-up the mean permeability was 8.42 (95% confidence interval from 5.2 to 13.5); the difference was far from significance (p = 0.5), indicating that the leakage had been stabilized. The change from baseline to follow-up was not significantly different for eyes with or without visual loss.
Discussion
Risk factors for progression of diabetic retinopathy and macular edema are HbA1c, duration of diabetes and blood-pressure [17]. In the present study, we have investigated baseline fluorescein leakage, a marker of blood-retinal barrier breakdown in relation to visual loss 5 years after initial photocoagulation. At follow-up the mean visual acuity had decreased in most patients, and a significant odds ratio of 16 was found for the risk of a substantial visual loss of 3 lines or more in patients with high baseline leakage. The predictive power was stronger than other parameters such as diabetes duration, HbA1c and blood-pressure.
Breakdown of the blood-retina barrier is the basic mechanism of edema formation in diabetes, due to changes in the proteins forming zonula occludents between endothelial cells. Breakdown in human diabetic patients occurs early, and could even be present before visible retinopathy, but the evidence is conflicting [16, 18]. With time, leakage does increase, and in a 4-year study of patients with no retinopathy at baseline the blood-retinal barrier permeability measured with vitreous fluorometry had increased significantly, in parallel with progression to retinopathy [19]. In patients with mild, clinically nonsignificant macular edema, blood-retinal barrier permeability seems to be increased more then 1 year before the retinal thickness changes, underlining the predictive value of vitreous fluorometry [13]. The long time span from increased leakage to increased retinal thickness indicates that there is no straightforward relationship between leakage and retinal thickening; leakage and retinal thickness are not necessarely the same, though they are certainly correlated [6, 9, 13]. The difference may partly be explained by the use of fluorescein as a marker of water movements. However, many other factors may be involved in the resulting retinal thickness for a given leakage, including blood-pressure in the retinal vasculature, tissue osmotic pressure and the role of aquaporins. These factors, including also tissue damage, may account for the lack of normalisation of retinal thickness in diffuse edema despite treatment [6].
The blood-retinal barrier permeability in the study did not show significant changes over time, in parallel with a previous study with follow-up at 6 months, though the short-term study found a difference in eyes with and without clinical resolution of the CSME [20]. The reason for a relatively stable permeability over time remains unclear, but it should be noted that HbA1c and blood-pressure were not improved, and that though photocoagulation seems to have decreased macular edema, the damage on retinal vessels and the blood-retinal barrier remains. The 14-year follow-up of the Wisconsin study was still able to detect the risk factors from baseline on progression of retinopathy and edema, indicating the effect of metabolic regulation over a long time-span [21].
The visual loss found in the present study might represent a cumulative effect of regulation, with no major changes in the retinal disease and leakage.
Current studies seem to indicate that treatment with intravitreal steroids or VEGF inhibition in diabetic macular edema are effective in some patients with diabetic macular edema. In view of residual edema, the need for multiple injections and risk for complications, evaluation of the blood-retinal barrier may be valuable for finding patients in need for such treatments due to poor outcome of photocoagulation, and probably also to specify inclusion criteria.
In conclusion, blood-retinal barrier permeability is a sensitive prognostic factor for long-term substantial visual loss of 3 lines or more after photocoagulation in CSME. Blood-retinal barrier permeability is also increased before CSME develops, and taken overall blood-retinal barrier permeability is an early and strong predictor of the visual outcome. Clinical studies as well as daily clinics should include evaluation of leakage before intravitreal and other invasive treatments, both to exclude patients with mild edema which could be treated by photocoagulation, and possibly also to establish untreatable cases.
References
Early treatment diabetic retinopathy study research group (1991) Classification of diabetic retinopathy from fluorescein angiograms. ETDRS report no.11. Ophthalmology 98:807–822
Early treatment diabetic retinopathy study research group (1995) Focal photocoagulation treatment of diabetic macular edema. Relationship of treatment effect to fluorescein angiographic and other retinal characteristics at baseline. ETDRS report no.19. Arch Ophthalmol 113:1144–1155
Early treatment diabetic retinopathy study research group (1985) Photocoagulation for diabetic macular edema. ETDRS report no.1. Arch Ophthalmol 103:1796–1806
Early treatment diabetic retinopathy study research group (1991) Grading diabetic retinopathy from stereoscopic color fundus photographs - an extension of the modified Airlie House classification. ETDRS report number 10. Ophthalmology 98:786–806
Strom C, Sander B, Larsen N, Larsen M, Lund-Andersen H (2002) Diabetic macular edema assessed with optical coherence tomography and stereo fundus photography. Invest Ophthalmol Vis Sci 43:241–245
Soliman W, Vinten M, Sander B, Soliman KA, Yehya S, Rahman MS, Larsen M (2008) Optical coherence tomography and vessel diameter changes after intravitreal bevacizumab in diabetic macular oedema. Acta Ophthalmol 86:364–371
Chew E, Strauber S, Beck R, Aiello LP, Antoszyk A, Bressler N, Browning D, Danis R, Fan J, Flaxel C, Friedman S, Glassman A, Kollman C, Lazarus H, Diabetic Retinopathy Clinical Researh Network (2007) Randomized trial of peribulbar triamcinolone acetonide with and without focal photocoagulation for mild diabetic macular edema: a pilot study. Ophthalmology 114:1190–1196
Shimura M, Nakazawa T, Yasuda K, Shiono T, Iida T, Sakamoto T, Nishida K (2008) Comparative theraphy evaluation of intravitreal bevacizumab and trimacinolone acetonide on persistent diffuse diabetic macular edema. Am J Ophthalmol 145:854–861
Vinten M, Larsen M, Lund-Andersen H, Sander B, la Cour M (2007) Short-term effects of intravitreal triamcinolone on retinal vascular leakage and trunk vessel diameters in diabetic macular oedema. Acta Ophthalmol 85:21–26
Audren F, Lecleire-Collet A, Erginay A, Haouchine B, Benosman R, Bergmann JF, Gaudric A, Massin P (2006) Intravitreal trimacinolone acetonide for diffuse diabetic macular edema: phase 2 trial comparing 4 mg vs 2 mg. Am J Ophthalmol 142:794–799
Soliman W, Sander B, Soliman KA, Yehya S, Rahamn MS, Larsen M (2008) The predictive value of optical coherence tomography after grid laser photocoagulation for diffuse diabetic macular oedema. Acta Ophthalmol 86:284–291
Sander B, Larsen M, Moldow B, Lund-Andersen H (2001) Diabetic macular edema: passive and active transport of fluorescein through the blood-retina barrier. Invest Ophthalmol Vis Sci 42:433–438
Sander B, Thornit DN, Colmorn L, Strom C, Girach A, Hubbard LD, Lund-Andersen H, Larsen M (2007) Progression of diabetic macular edema: correlation with blood retinal barrier permeability, retinal thickness, and retinal vessel diameter. Invest Ophthalmol Vis Sci 48:3983–3987
Moldow B, Sander B, Larsen M, Lund-Andersen H (1999) Effects of acetazolamide on passive and active transport of fluorescein across the normal BRB. Invest Ophthalmol Vis Sci 40:1770–1775
Sander B, Larsen M, Engler C, Strom C, Moldow B, Larsen N, Lund-Andersen H (2002) Diabetic macular oedema: a comparison of vitreous fluorometry, angiography, and retinopathy. Br J Ophthalmol 86:316–320
Sander B, Larsen M, Engler C, Lund-Andersen H, Parving HH (1994) Early changes in diabetic retinopathy: capillary loss and blood-retina barrier permeability in relation to metabolic control. Acta Ophthalmol 72:553–559
Klein R, Klein B, Moss S, Davis M, DeMets D (1984) The Wisconsin epidemiologic study of diabetic retinopathy. IV Diabetic retinopathy. Ophthalmology 91:1464–1474
Cunha-Vaz J (1983) Studies on the pathophysiology of diabetic retinopathy. The blood-retinal barrier in diabetes. Diabetes 32:20–27
Castillo A, Benitez del Castillo JM, Diaz D, Sayagues O, Ruibal JL, Garcia-Sanchez J (1996) Analysis of the blood-retinal barrier: its relation to clinical and metabolic factors and progression to retinopathy in juvenile diabetes. A 4-year follow-up. Graefes Arch Clin Exp Ophthalmol 234:246–250
Sander B, Larsen M, Engler C, Strøm C, Moldow B, Lund-Andersen H (2002) Diabetic macular oedema: the effect of photocoagulation on fluorescein transport across the blood-retinal barrier. Br J Ophthalmol 86:1139–1142
Klein R, Klein BE, Moss S, Cruickshanks KJ (1998) The Wisconsin epidemiologic study of diabetic retinopathy: XVII The 14-year incidence and progression of diabetic retinopathy and associated risk factors in type diabetes. Ophthalmology 105:1801–1815
Acknowledgements
The study was supported by the Danish Diabetes Foundation and the VELUX Foundation.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Sander, B., Hamann, P. & Larsen, M. A 5-year follow-up of photocoagulation in diabetic macular edema: the prognostic value of vascular leakage for visual loss. Graefes Arch Clin Exp Ophthalmol 246, 1535–1539 (2008). https://doi.org/10.1007/s00417-008-0892-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00417-008-0892-6