
Abstract
Background
Photorefraction can be carried out in both eyes simultaneously from a distance and is therefore suitable for examination of children. This study evaluated the accuracy of a commercially available photorefractometer (PowerRefractor, Plusoptix, Erlangen, Germany) and investigated whether the working distance relaxes the accommodation sufficiently without cycloplegia.
Methods
Photorefractometer readings were compared to cycloplegic retinoscopy. Because of the limited working range the group of patients consisted of low and moderate ametropic eyes within a spherical power of −7.0 to +5.0 D. One hundred and ninety-two eyes from 104 patients (2–81 years) were photorefracted under cycloplegia. A subgroup of 83 eyes from 46 patients was additionally refracted without cycloplegia.
Results
Under cycloplegia, the PowerRefractor measured the spherical equivalent slightly below that of cycloplegic retinoscopy (too much minus). The mean difference in spherical equivalent was −0.12±0.91 D (SD). The mean difference of cylindrical power was −0.17±0.73 D. The mean weighted axis difference was 0.61±0.71 D which is comparable to an axis deviation of 18° at a cylinder power of 1.00 D. Without cycloplegia, the mean difference of the spherical equivalent was −0.73±1.25 D. The mean difference of cylindrical power was −0.20±0.65 D. The mean weighted axis difference was 0.44±0.58 D which is comparable to an axis deviation of 13° at a cylinder power of 1.00 D.
Conclusions
Without cycloplegia, the spherical equivalent of the PowerRefractor tends to be underestimated due to uncontrolled accommodation, especially in children. Cycloplegia improves the accuracy in evaluating the spherical equivalent, but decreases the accuracy of cylinder power and axis.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Photorefraction was developed as a screening tool to rule out amblyogenic ametropia in children. Several studies evaluated photorefractive devices including the PowerRefractor for their effectiveness in detecting anisometropia, hyperopia, myopia and astigmatism [2, 11, 21]. Due to the large working distance, photorefraction is suitable for examination of children and disabled patients. They do not have to put their head close to a device and feel threatened by the examiner. Furthermore, the distance may relax accommodation and gain higher accuracy when investigating hyperopia in children. Sparing cycloplegia would simplify screening for this amblyogenic factor. Photorefraction also allows examination of both eyes simultaneously. This accelerates the measurement procedure and should provide the exact amount of anisometropia as another amblyogenic factor. However, photorefraction suffered from poor accuracy and limited working range. Several attempts were made to increase the accuracy since its first description in 1974 [9]. In the latest generation, three meridians of the eye are measured to enhance axis determination and gain accuracy in the assessment of cylinder power. This is important because astigmatism, especially in the oblique axis, is a further amblyogenic factor.
In photorefraction, light from illumination sources near the aperture of the camera lens is reflected from the eye into the camera. The pattern of light is imaged through the camera and varies with the eye’s refractive error and pupil size. Under consideration of the pupil size, the refractive error can be calculated on the pattern size and intensity distribution.
This study evaluated the accuracy of a new commercially available photorefractometer (PowerRefractor; Plusoptix, Erlangen, Germany). We also wanted to investigate whether the working distance relaxes the accommodation sufficiently without cycloplegia.
Materials and methods
Subjects
Patients were recruited at the ward and outpatient department of an university eye hospital. All of them were informed and consented their participation in the study. According to the recommendations of the manufacturer the eyes did not exceed a maximum spherical range of −7.00 to +5.00 D and a cylinder range of −7.00 to +5.00 D. All patients underwent a complete ophthalmologic examination, including a cover test and determination of central fixation by funduscopy. Eyes with eccentric fixation or opacities of the optical media or any affection of the retina were excluded from the study. Therefore in some subjects only one eye was suitable for statistical analysis.
The accuracy of the video autorefractor was studied in two groups of patients:
-
Group 1: 192 eyes of 104 patients were photorefracted in cycloplegia. The median age of the subjects was 43 years (range 2–81 years). The median spherical equivalent was +0.75±4.75 D (SD), (range −7.50 to +4.75 D). The mean cylinder power was −0.72±0.62 D (range 0 to −5.75 D).
-
Group 2: As a subgroup of group 1, 83 eyes of 46 patients were photorefracted without cycloplegia in addition to the cycloplegic examination. The median age of the subjects was 13 years (range 2–73 years). Their median spherical equivalent was +1.00±1.87 D (range −6.50 to +4.75 D). The mean cylinder power was −0.68±0.71 D (range 0 to −3.75 D).
All measurements were performed within one session in the following order:
-
1.
Photorefraction without cycloplegia
-
2.
Cycloplegic retinoscopy
-
3.
Cycloplegic photorefraction
The short time interval between all measurements should minimize errors from the well-known diurnal changes of ametropia [6, 18]. Cycloplegia was obtained by instilling one drop of cyclopentolate 1% in each eye. After 10 min a second drop was given. After another 20 min, standard retinoscopy and measurement with the photorefractometer was carried out within a few minutes. Patients with dark irides were given one more dose if it was judged that cycloplegia was incomplete on the basis of pupil activity and variability in the retinoscopic neutral point. In children under 3 years of age (n=5), cyclopentolate 0.5% or tropicamide 0.5% was used in the same manner described. A recent investigation [23] did not reveal any statistically or clinically significant difference between cycloplegic measurements using cyclopentolate or tropicamide.
Photorefraction and characteristics of the PowerRefractor
The PowerRefractor version we used consists of a small camera mounted on a portable computer (200 MHz Pentium) with integrated keyboard and flat-screen (TFT display, 752×400 dpi). The device formerly distributed by MultiChannelSystems is now available at PlusOptix (Erlangen, Germany), which continues to develop hardware and software.
The refractor is based on an advanced eccentric photorefraction technique. As further improvement of the earlier two-flash photorefractometers, the measurement has been extended in a third meridian: six blocks of infrared light emitting diodes (LEDs) are placed around the lens of an infrared digital video camera. The patient’s fixation is directed toward the camera by the circling light from LED blocks.
The examiner sits behind the device, adjusts the mobile camera to the face of the patient at a distance of 1 m and monitors the results on the screen. When young children are measured, the infant is held upright on the mother’s lap. The examiner can attract the interest of the child by making noise or showing toys. Older children should be placed on a chair with a back-rest to avoid them getting out of focus by moving backwards and forwards. Parents may fix the head of the child for the short period of measurement if there is still too much movement.
Dim room light leads to mydriasis. Both eyes of the subject are illuminated in three meridians (30°, 90° and 150°) in rapid succession. Opposite blocks of LEDs illuminate each meridian two times and create crescents in the pupil. The first Purkinje light reflex from the surface of the cornea is visible near the middle of each pupil. Other light sources in the room can disturb the measurement by causing additional light effects in the eye and should be eliminated.
The patient’s eye is shown on a computer screen in real time at a processing frequency of 25 Hz. Lack of fixation as determined by the Hirschberg test or pupil margins obscured by inadequate lid apertures are noticed immediately. In the case of ptosis, the patient or an assistant may lift the eyelid. In strabismic patients, each eye has to be measured separately while covering the other eye. Opacities of the cornea, the lens or of the vitreous body become obvious as dark shadows in the illuminated pupil.
Refractive results are automatically calculated based upon the slope of the light intensity distribution of the crescents within the pupil. Measurements are taken continuously, and the refraction is displayed in red or green color below the image of the corresponding eye. Red color signals an uncertain result, green color signals high consistency of values. Hints are given automatically when the eye is out of focus, the pupil is to small or the room light might be not adequate. In addition, pupil size and interpupillary distance are shown on the screen.
The user can interrupt the measurement when high reliability of the result is signalized. The first result fulfilling this criterion was taken for the analysis. Eyes are to be excluded when the measurement did not reach this level of certainty. All examinations were performed by a single operator who was unaware of the prior refractive history and the retinoscopic results.
Retinoscopy
When cycloplegia was complete, streak retinoscopy was performed in all subjects by one examiner using handheld corrective lenses. The axis was determined by directing the streak to a TABO scheme at the wall. The investigator was unaware of the prior refractive history and the results found with the photorefractor. The results of cycloplegic retinoscopy were compared to the photorefractive results in both groups of patients.
Criteria for the accuracy of measurement
The following comparison criteria have been established by Rassow and Wesemann [16, 20, 24, 27] since 1984. They allow a direct comparison of the PowerRefractor with autorefractors tested in previous studies.
The difference in the spherical equivalent (DSE) was calculated as
S and C denote the spherical and the cylinder powers. The subscript “t” (test) and “c” (comparison) denote the instrument under test (PowerRefractor) and the comparison technique (cycloplegic retinoscopy). A negative DSE indicates a minus overcorrection of the tested instrument.
The difference of the cylindrical powers (DC) was calculated as
The weighted axes difference (DA) was evaluated by a formula in which the difference between the two cylinder axes (test and comparison, measured in degrees) is weighted with the cylinder power measured with the comparison method.
The formula allows a comparison of axis values, even when actual cylinder powers are different. Cc is taken as weighting factor, since it is assumed to be more accurate then the cylinder power of the tested instrument. Geometrically, DA is the length of the difference vector between both methods given that the cylinder power found with the PowerRefractor is equal to the cylinder power found with retinoscopy. The resulting number has the dimension “diopter”. A value of DA=0.5 D is equal to an axes difference of 14.5° given a cylinder power found with the comparison method of 1.0 D.
A similar way of statistical analysis of angular data is provided by the J-vector method [15]. As in the DA calculation, astigmatism is represented in a rectangular vector form. The principle is based on the Jackson crossed cylinder (JCC). The astigmatic values are resolved into the sum of two other JCC lenses, one with power J0 at axis α=0° and the other with power J45 at α=45° [21].
Since the J vectors are given in rectangular coordinates, the difference vector (ΔJ) is easily computed by subtracting corresponding values along each of the coordinate axes separately. Thus, the cylinder power of the test and comparison measurement are considered.
The following quality criterion is the total cylindrical difference (TCD). It is mathematically equivalent to the J-vector method and represents the length of the difference vector between the cylindrical corrections measured with the test and comparison method. Because different units are used between the both methods, the J-vector method corresponds to 1/2 TCD [20].
The difference in the total refraction (DTR) is a measure of blur strength, and incorporates the difference of spherical power, cylindrical power and axis deviation. The DTR was firstly defined by Grimm in 1981 [7].
Results
Accuracy in ametropic patients under cycloplegia
Difference of spherical equivalents
The difference in the SE between PowerRefractor and cycloplegic retinoscopy is shown in Fig. 1a. The central column of the frequency distribution indicates that nearly 30% of the SEs differed by less than ±0.25 D. The other columns show how often larger errors occurred. A second peak occurs at −2.00 D. Sixteen percent of the results differed more than −1.00 D and less than −2.00 D. The maximal differences were −2.63 and +4.50 D. In average, the PowerRefractor delivered a SE that is very close to that obtained by retinoscopy under cycloplegia (DSEmean=−0.12±0.91 D SD). In total 78% of the results differed less than 1.00 D, 4% differed more than 3.00 D from the retinoscopic findings.

Frequency distribution of the differences between photorefraction and retinoscopy (group 1, both measurements under cycloplegia); a difference of the spherical equivalents; b difference of the cylinder powers; c weighted axes difference. Each bar represents the percentage of results differing less than the amount displayed on the x-axis. For example, in a the central column of the frequency distribution indicates that nearly 30% of the SEs differed by less than ±0.25 D. At −2.00 D 16% of the results differed more than −1.00 D and less than −2.00 D.
Difference of cylindrical powers
The cylinder powers determined by the PowerRefractor and retinoscopy were very similar. Forty-seven percent differed by less than ±0.25 D. The distribution in Fig. 1b is almost symmetric and shows few higher cylinder power differences. The mean difference was −0.17±0.73 D. Ninety percent of the results differed less than 1.00 D, 1% more than 3.00 D from the retinoscopic result.
Weighted axes difference
The accuracy of the axis was evaluated in the cases in which a cylinder power of 0.25 D or greater had been determined with the autorefractometer and with retinoscopy. This occurred in 160 of 192 eyes. The mean axes difference was 0.61±0.71 D (Fig. 1c). In a few cases, large differences were found. The largest was 4.43 D (cylinder power −2.25 D, axis deviation 80°). In 85% the difference was below 1.00 D, in 5% over 3.00 D compared to retinoscopy.
Total cylindrical difference
The mean total cylindrical difference was 0.85±0.66 D. The largest difference was 4.82 D, the smallest 0.03 D.
Difference of total refraction
The mean difference of total refraction was 1.16±0.72 D. The largest difference was 5.15 D, the smallest 0.04 D.
Accuracy in ametropic patients without cycloplegia
Difference in spherical equivalents
The DSE distribution in Fig. 2a is not symmetric. It shows a shift towards negative values. The SE measured with the photorefractor was accurate to ±0.50 D in 37% of all cases. In 69%, the DSE was less than 1.00 D, in 17% it was more than 3.00 D. The mean DSE was −0.73±1.25 D (range +1.50 to −4.00 D).

Frequency distribution of the differences between photorefraction and retinoscopy (group 2, photorefraction without cycloplegia); a difference of the spherical equivalents; b difference of the cylinder powers; c weighted axes difference. The percentage of minus-overcorrected cases (DSE <0 in a) is much larger than in Fig. 1a. The distributions in b and c are more narrow compared to those in Fig. 1b and 1c.
Difference of cylindrical powers
The accuracy in measuring cylinder power was similar to the measurement under cycloplegia (Fig. 2b). The mean difference was −0.20±0.65 D. Ninety-three percent of the results differed less than 1.00 D, 2% more than 3.00 D from the retinoscopic result.
Weighted axes difference
Sixty-five eyes showed a cylinder power of 0.25 D or greater and were included in the analysis. The mean DA was 0.44±0.58 D (Fig. 2c). The largest difference was 3.60 D (cylinder power −2.50 D, axis deviation 46°). Ninety-two percent of the results differed less than 1.00 D, 3% more than 3.00 D from the retinoscopic result.
Total cylindrical difference
The mean total cylindrical difference was 0.73±0.66 D. The largest difference was 3.26 D, the smallest 0.02 D.
Difference of total refraction
The mean difference of total refraction was 1.39±0.99 D. The largest difference was 4.03 D, the smallest 0.04 D.
Accuracy indices
Table 1 summarizes the data presented in the histograms (Figs 1 and 2). It indicates how often the differences were smaller than a selected criterion value. This is a measure for the percentage of correct (result test=result comparison) or almost correct results (result test−result comparison<selected criterion value). Data found with seven other table-top refractors of an earlier generation [24] and recent studies with the Nikon Retinomax [27] and Welch Allyn SureSight [20] are presented for comparison.
Accuracy of cycloplegic measurements
The percentage of almost correct results found with the PowerRefractor in cycloplegic eyes (first row) lies below the range found with the handheld SureSight under cycloplegia [20] (row 3), the handheld Retinomax under cycloplegia [27] (row 5) and seven different table-top autorefractometers without cycloplegia [24] (row 7). The four quality criteria for the PowerRefractor varied from 45% to 66%. This indicates that the present version of the photorefractor is less accurate than other autorefractors.
Accuracy of non-cycloplegic measurements
The accuracy of the SE was substantially lower without cycloplegia (second row). The number of correct or almost correct spherical results dropped from 52% to 37%. The accuracy of the cylinder power was higher compared to the results under cycloplegia (82% versus 66%). The results of DA were also better than under cycloplegia. This indicates a higher accuracy in measuring the axis of the astigmatism. This may be explained by disturbing peripheral aberrations that occur in wide pupils of cycloplegic eyes or the higher risk of measuring outside the optical axis.
Further analysis of the cylindrical differences
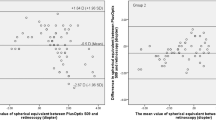
Results of the J-vector analysis of all patients in group 2 are shown in Fig. 3. The two-dimensional scatterplots visualize the distribution of the ΔJ vectors calculated for all eyes. All difference vectors start at the origin. For clarity, only the endpoint of each vector (the tip of the vector) is denoted by a black diamond; the entire vector is not shown. As cylindrical differences were measured in the conventional way and not in the JCC units, both axes in Fig. 3 are scaled in units of 2ΔJ.

Two-dimensional polar plot of the vector differences 2ΔJ between the cylindrical corrections (group 2). Upper panel: photorefractor without cycloplegia. Lower panel: both measurements under cycloplegia. ΔJ was calculated for each eye. All vectors start at the origin. For clarity, only the endpoint of each vector is shown. The distance of each diamond from the origin indicates the discrepancy between the two methods. All data inside the circle denote measurements in which the TCD was smaller than our criterion difference of 0.63 D.
The distance of each diamond from the origin characterizes the discrepancy between PowerRefractor and retinoscopy. Diamonds lying exactly at the origin indicate measurements in which cylinder power and axis obtained with both measurement techniques were identical. All vectors whose endpoints lie within the circle have a length of TCD <0.63 D. In contrast to the TCD values listed in Table 1, Fig. 3 contains all results, even those without a cylinder power measured in the test or comparison method. Thus the values confining to the quality criterion ≤0.63 D differ. The scatterplot depicted in Fig. 3a represents the ΔJ vectors from the results of the PowerRefractor taken without cycloplegia. A few data points lie far off the circle indicating a considerable discrepancy between both measurements.
In Fig. 3b the same eyes of Fig. 3a were measured with cycloplegia. The number of large differences (points outside the circle) has increased. Our quality criterion (TCD ≤0.63 D) is met by 65% of all measurements in Fig. 3a and 57% in Fig. 3b. The decreasing percentage indicates that the discrepancy between PowerRefractor and retinoscopy increases with cycloplegia.
Influence of accommodation in patients with and without cycloplegia
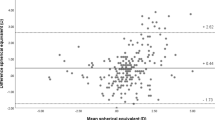
The individual SEs measured by the PowerRefractor in group 2 are plotted against results obtained by cycloplegic retinoscopy in Fig. 4a and b. The upper panel shows the data points obtained under cycloplegia. The lower panel represents the results found without cycloplegia. All patients were divided into three subgroups. The first subgroup (triangles) comprises “children” (aged 3–20 years). Squares denote “young adults” (aged 21–40 years). Diamonds denote “older adults” (aged 41–73 years).

Individual SEs measured by the photorefractor versus cycloplegic retinoscopy (group 2). Upper panel: both measurements under cycloplegia. Lower panel: photorefractor without cycloplegia. The cycloplegic results agree well with retinoscopy. All data points lie close to the diagonal line that indicates perfect agreement. Without cycloplegia, many data points lie below the diagonal DSE=0 D line, indicating a minus overcorrection. The accommodating patients are mainly children (triangles) and young adults (squares). The additional dotted line at −1 D shows the autorefractor reading that would be expected when patients accommodate at a distance of 1 m.
In the range SE ±4.00 D, the data points in the upper panel (Fig. 4a) scatter almost equally around the diagonal line that represents ideal agreement. This illustrates that the SEs found with the photorefractor under cycloplegia were similar to the values obtained with cycloplegic retinoscopy. Outside this range, the SE of the photorefraction is systematically below that of cycloplegic retinoscopy.
Without cycloplegia, many data points obtained by the PowerRefractor fall below the diagonal line. These data points indicate a minus overcorrection by the photorefractor. It is obvious from Fig. 4b that minus-overcorrected results are much more frequent in emmetropic and hyperopic patients. Almost 50% of all children (triangles) with a hyperopia ≥1.0 D were minus overcorrected by more than −2.0 D. Eleven of 44 children eyes showed a minus overcorrection of −2.0 to −4.0 D. The mean SE of the children investigated with cycloplegia was 0.96 D higher than without.
The data of the emmetropic and hyperopic young adults also lie consistently below the diagonal line. The mean SE of this subgroup was 0.60 D higher with cycloplegia than without. The older adults, however, show no significant differences with and without cycloplegia.
Discussion
This investigation has shown that autorefraction using the PowerRefractor without cycloplegia leads to a considerable shift towards myopic values in young subjects due to accommodation. Accurate evaluation of refractive errors requires that accommodation is stable and known at the time of measurement. This essential control is typically attempted by one of three methods: (1) by providing a distant accommodative stimulus, such as an acuity chart; (2) by providing only neutral or ineffective accommodative stimuli; or (3) by paralyzing the ciliary muscle with cycloplegic drugs.
-
1.
Providing a distant accommodative stimulus does not expose the true amount of hyperopia. An acuity chart at a distance of 5 m pretends an accommodation of 0.2 D (1/5 m). If a hyperopic eye of for instance +6.0 D accommodates exactly onto the acuity chart the amount of accommodation is 6.2 D. However, the actual refraction at this moment is −0.2 D and the true refraction is unknown.
-
2.
Under dark room, stimulus-free conditions a myopic shift to tonic accommodation occurs. It is the equilibrium established between sympathetic and parasympathetic tone. Tonic accommodation varies by as much as 4.00 D between subjects and is greatest in hyperopic individuals [12]. Mohindra [13] has developed a technique in which the light source of a retinoscope is the only visible stimulus in a darkened room. This fixation target has been shown by Rosenfield [17] and Owens et al. [14] to provide a poor stimulus for accommodation. Choi et al. [5] did not reveal any difference whether children fixated the camera of the PowerRefractor at a 1-m distance or a target at a 3-m distance. They concluded that the camera was not a significant stimulus to accommodation.
-
3.
Paralyzing the ciliary muscle with cycloplegic drugs is the most effective but also an invasive way to suppress accommodation. “Cycloplegic retinoscopy using cyclopentolate is the gold standard by which other methods are compared.” [23].
The working distance of the PowerRefractor is 1.0 m. Patients with myopia of −1.0 D or more are not stimulated to accommodate because their far point is at 1.0-m distance or closer. If patients with myopia less than −1.0 D, emmetropia or hyperopia accommodate exactly onto the target, the instrument will detect a spherical equivalent of −1.0 D (dotted line in Fig. 4b) regardless of the real ametropia. This state of pseudomyopia is denoted as fixation myopia [20]. Its amount is not known prior to the measurement. It can assume any value between the real ametropia and the accommodated state reciprocal to the target distance (in this case −1.0 D). This problem has been reported from other studies using photorefraction without cycloplegia [1, 8]. Due to presbyopia, accommodation did not occur in the older patients (represented as diamonds in Fig. 4b). However, some of the young hyperopic subjects in our investigation did not accommodate as well (triangles on the diagonal line of Fig. 4b). Some accommodated up to 4.0 D. This variability of accommodation in young patients may be explained by the attention of the subject, the accommodative stimulus of the environment behind the camera or by the well-known lag of accommodation in hyperopic children [2]. Pseudomyopia does not only occur in autorefractors operating from a distance but also in table-top devices using fogging techniques. In these systems operating at short distance, the reason for minus overcorrection is different. It is caused by the subjective feeling of nearness and affects both hyperopes and myopes.
Under cycloplegia, the PowerRefractor yielded good spherical readings in a range of about ±4.0 D but tended to underestimate higher ametropia. This phenomenon is typical for photorefraction [3, 4, 10, 11, 19, 26]. Outside a range of −7.0 to +5.0 D, it can even erroneously yield emmetropia [21].
Since cycloplegia produces mydriasis as well, accuracy of refraction with and without cycloplegia is also influenced by the pupil diameter. Howland [10] and Bobier et al. [3, 4] analyzed this optical parameter and considered it in mathematical formula.
The PowerRefractor assessed cylinder power and axis more precise when the pupils of the eyes were unaltered by cycloplegic drugs. An explanation may be peripheral aberrations of cycloplegic pupils that disturb the measurement. Accordingly, it might be advantageous to analyze only the central region of the dilated pupil by software modification. Inaccuracy in determination of cylinder power and axis has been described for two-flash photorefractors [22, 25]. Our investigation using a “three-flash” device also revealed inaccuracy.
Table 1 shows a comparison with previous investigations of other, non-photorefractive devices. In order to facilitate comparison, we tried to adapt as much as possible of their study designs. However, the selection of subjects concerning age and frequency of refractive errors was different and limits comparability. The selection in the evaluation of the SureSight [20] was quite similar to our study. In the Retinomax evaluation [27], only adults were examined without cycloplegia. This may be an explanation of the high frequency (88%) of eyes within 0.5 D of the DSE. The authors stated that accommodation was predominantly a problem of small children.
A potentially weak point of studies investigating both eyes of subjects is a possible intercorrelation of both eyes, since refraction is often similar in both eyes. One way to avoid this statistical problem is to analyze only one eye of the subjects. However, including both eyes yields a higher statistical power.
In conclusion, this investigation has shown that results obtained with the PowerRefractor are dependent on whether cycloplegia has been applied or not. In young patients uncontrolled accommodation is the main factor influencing the spherical equivalent. In order to reduce this error, measurements should be performed under cycloplegia. This, however, leads to reduced precision in determination of cylinder power and axis. Thus, cylinder power and axis should be examined prior to cycloplegia. For ophthalmologists unskilled in retinoscopy the PowerRefractor is a useful tool for estimating the refraction in patients repelling conventional autorefraction.
References
Althaus K, Bischoff P (1994) Videorefraktionsmessung im ersten Lebensjahr. Klin Monatsbl Augenheilkd 205:133–137
Atkinson J, Braddick OJ, Bobier B, Anker S, Ehrlich D, King J, Watson P, Moore A (1996) Two infant vision screening programmes: prediction and prevention of strabismus and amblyopia from photo- and videorefractive screening. Eye 10:189–198
Bobier WR, Braddick OJ (1985) Eccentric photorefraction: optical analysis and empirical measures. Am J Optom Physiol Opt 62:614–620
Bobier WR, Campbell MCW, McCreary CR, Power AM, Yang KC (1992) Geometrical optical analysis of photorefractive methods. Ophthal Physiol Opt 12:147–152
Choi M, Weiss S, Schaeffel F, Seidemann A, Howland HC, Wilhelm B, Wilhelm H (2000) Laboratory, clinical, and kindergarten test of a new eccentric infrared photorefractor (PowerRefractor). Optom Vis Sci 77:537–548
Cronje S, Harris WF (1997) Short-term keratometric variation in the human eye. Optom Vis Sci 74:420–424
Grimm W (1981) Automatische objective Refraktionsbestimmung. DOZ 37:23–34
Hodi S, Wood ICJ (1994) Comparison of the techniques of videorefraction and static retinoscopy in the measurement of refractive error in infants. Ophthal Physiol Opt 14:20–24
Howland HC, Howland B (1974) Photorefraction: a technique for study of refractive state at a distance. J Opt Soc Am 64:240–249
Howland HC (1985) Optics of photoretinoscopy: results from ray tracing. Am J Optom Physiol Opt 62:621–625
Hsu-Winges C, Hamer RD, Norcia AM, Wesemann H, Chan C (1989) Polaroid photorefractive screening of infants. J Pediatr Ophthalmol Strabismus 26:254–260
McBrien NA, Millodot M (1987) The relationship between clinically measured tonic accommodation and refractive error. Invest Ophthalmol Vis Sci 28:997–1004
Mohindra I (1975) A technique for infant vision examination. Am J Optom Physiol Opt 52:867–870
Owens DA, Mohindra I, Held R (1980) The effectiveness of a retinoscope beam as an accommodative stimulus. Invest Ophthalmol Vis Sci 19:942–949
Raasch TW, Schechtman KB, Davis LJ, Zadnik K (2001) Repeatability of subjective refraction in myopic and keratoconic subjects; results of vector analysis; CLEK Study Group. Ophthalmic Physiol Opt 21:376–383
Rassow B, Wesemann W (1984) Automatic infrared refractors–1984b. Ophthalmology 91(suppl):10–26
Rosenfield M (1989) Evaluation of clinical techniques to measure tonic accommodation. Optom Vis Sci 66:809–814
Rosenfield M, Chiu NN (1995) Repeatability of subjective and objective refraction. Optom Vis Sci 72:577–579
Schimitzek T, Krzizok T (2001) Messungenauigkeit der Videorefraktometrie bei höheren Ametropien. Klin Monatsbl Augenheilkd 218:438–444
Schimitzek T, Wesemann W (2002) Clinical evaluation of refraction using handheld wavefront autorefractor in young and adult patients. J Cataract Refract Surg 28:1655–1666
Schimitzek T, Haase W (2002) Efficiency of a video-autorefractometer used as a screening device for amblyogenic factors. Graefe’s Arch Clin Exp Ophthalmol 240:710–716
Thompson A, Li T, Peck LB, Howland HC, Counts R, Bobier WR (1996) accuracy and precision of the Tomey ViVA infrared photorefractor. Optom Vis Sci 73:644–652
Twelker JD, Mutti DO (2001) Retinoscopy in infants using a near noncycloplegic technique, cycloplegia with tropicamide 1%, and cycloplegia with cyclopentolate 1%. Optom Vis Sci 78:215–222
Wesemann W, Rassow B (1987) Automatic infrared refractors—a comparative study. Am J Optom Physiol Opt 64:627–638
Wesemann W, Norcia AM, Allen D (1991) Theory of eccentric photorefraction (photoretinoscopy): astigmatic eyes. J Opt Soc Am 8:2038–2047
Wesemann W, Wesemann H (1994) Photorefraction—an objective refraction technique for small children. In: Schulz E (ed) Symposium (to honor Professor Dr. Wolfgang Haase on his 60th birthday) on visual development and “update” in strabismus. Strabismus 2:147–168
Wesemann W, Dick B (2000) Accuracy and accommodation capability of a handheld autorefractor. J Cataract Refract Surg 26:62–70
Acknowledgements
The authors have no financial interest in any of the products mentioned in the manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Schimitzek, T., Lagrèze, W.A. Accuracy of a new photorefractometer in young and adult patients. Graefe's Arch Clin Exp Ophthalmol 243, 637–645 (2005). https://doi.org/10.1007/s00417-004-1056-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00417-004-1056-y