
Abstract
Emotional processing may be abnormal in amyotrophic lateral sclerosis (ALS). Our aim was to explore functional anatomical correlates in the processing of aversive information in ALS patients. We examined the performance of nine non-demented ALS patients and 10 healthy controls on two functional MRI (fMRI) tasks, consisting of an emotional attribution task and a memory recognition task of unpleasant versus neutral stimuli. During the emotional decision task, subjects were asked to select one of three unpleasant or neutral words. During the memory task, subjects were asked to recognize words presented during the previous task. Controls showed, as expected, greater activation in the right middle frontal gyrus during selection of unpleasant than neutral words, and a greater activation mainly in right-sided cerebral areas during the emotional recognition task. Conversely, patients showed a general increase in activation of the left hemisphere, and reduced activation in right hemisphere in both emotional tasks. Such findings may suggest extra-motor neurodegeneration involving key circuits of emotions, mostly negative, commonly involved in FTD.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Evidence of extra-motor cerebral dysfunction in amyotrophic lateral sclerosis (ALS) comes from both structural and functional imaging studies. A series of functional imaging studies using PET and fMRI have shown a pattern of predominant frontotemporal dysfunction in non-demented ALS patients with verbal fluency deficits [1–3]. Thalamic and hippocampal system degeneration has also been demonstrated [1, 2]. Mezzapesa et al. [4] showed significant grey matter reduction in temporal and frontal lobes bilaterally, with a prevalence of right hemisphere involvement in ALS patients. Evidence of white matter involvement has also been found in frontotemporal regions, predominantly in patients with verbal fluency deficits [5]. Neuropsychological deficits, found as independent from level of disability[6], are now well-established, including frontotemporal dementia (FTD) in 5–15% of cases [7] and mild cognitive impairment, mainly evident in executive functions [8, 9], in up to 35% of non-demented ALS patients. Behavioural abnormalities and difficulties with social judgement have been described recently as frequent in these patients [10, 11]. Gibbons et al. [12] described a behavioural spectrum that ranges from no changes to behaviours similar to those seen in FTD, such as disinhibition, behavioural stereotypes, compulsions and reduction in response to pain. Similarly, changes in emotional control in ALS have been frequently described as a common symptom [13]. Recent studies have also described changes in emotional perception, i.e. emotional facial expression recognition, both in ALS and FTD patients [14, 15]. Papps et al. [16] found a selective failure in memory for emotional material in ALS, while Lulé et al. [17] found altered emotional responses to a picture test with respect to positive valence and decreased excitability for extremely emotional stimuli. In a more recent fMRI study, the same authors [18] found that ALS patients showed increased activation in the right supramarginal area and a reduced response in extrastriate visual areas when presented with emotional stimuli depicting social interaction and facial expression. Thus, compared to healthy controls, ALS patients showed enhanced (i.e. altered) sensitivity to social-emotional cues.
The aim of this study was to use fMRI to further investigate the brain regions mediating emotional processing of words, using a protocol which involved the explicit evaluation of emotional valence and subsequent recognition of unpleasant and neutral words. The finding of such dysfunction may also imply relevant issues for clinicians.
Methods and materials
Patients and controls
Ten patients with sporadic ALS were recruited from the Motor Neuron Disease Centre of the University of Padova. All of them met the criteria for probable or definite ALS (Revised El Escorial Criteria) [19]. Physical disability was measured using the ALS/FRS-r [20]. Patients were excluded a priori if their severity of upper limb involvement prevented them from undertaking the manual task, and if the severity of bulbar symptoms made it uncomfortable for them to breath whilst lying supine in the MRI scanner. A score higher than clinical cut-off for suspected presence of depression on BDI [21] was a further exclusion criteria, as well as the presence of frontotemporal lobar degeneration according to Neary’s criteria [22]. A patient was excluded after the performance in the scan because of excessive movement. Finally, nine ALS patients were tested (7 males; mean age 51.67 ± 11.45; range 32–63 years; mean education 8.89 years). Ten healthy comparable controls were recruited. Detailed data are shown in Table 1. All subjects were fluent in Italian, were right-handed as determined by the Edinburgh Handedness Inventory [23], and had normal visual acuity (measured by a Snellen Test); none had a history of previous significant head injury or cerebrovascular disease.
Neuropsychological and psychopathological measures
The ALS and control groups underwent a battery of neuropsychological tests focusing on executive and memory functions. Most tests were controlled for individual variations due to dysarthria and motor dysfunction [9] (detailed data and references are reported in Table 2). Patients’ and controls’ affective status was assessed with the Beck Depression Inventory (BDI) [21] and State-Trait Anxiety Inventory (STAI-Y1) [36]. Emotional Lability Questionnaire (ELQ) [14] was used to assess the presence of pathological laughing, crying or smiling.
The Kolmogorov–Smirnov test was applied in order to decide whether a parametric or non-parametric test was to be used: simple comparison between patients' and controls' scores were conducted using a parametric t test or non-parametric equivalents (Mann-Witney U tests). Significance was determined for p < 0.05. Measures are reported in Table 2.
Procedure
An adapted version of the emotional paradigm described by Tabert et al. [35] was employed. Neuropsychological profile, depressive symptoms and neurological condition, were investigated a few days (1-3 days) before the fMRI scan. Anxiety level was assessed with STAI-Y1 [36], both immediately before and immediately after fMRI scanning. On the day before the fMRI measurement, all subjects practiced a simulation of the two tasks outside the scanner using a different set of negative and neutral words. Written informed consent was obtained by all participants in accordance with the Declaration of Helsinki. The study protocol was approved by the Ethics Committee of the University of Padova.
Words selection process
The words were selected from the ‘Dictionary of word frequency in spoken Italian’ [37] which includes 10,561 words that have been rated for frequency in Italian spoken. We selected a large group of words (161) with similar length and high frequency. A group of 50 volunteers (32 males) rated these words on concreteness [from 1 (low concreteness) to 7 (high concreteness)] and unpleasantness [from 1 (unpleasant) to 7 (neutral)]. For the current study, we selected 30 words from those rated as the most unpleasant, and 30 words from those rated as the most neutral. Selected words did not differ in word length, frequency and concreteness (p > 0.05).
fMRI emotional decision task
Each word set was presented in eight alternating unpleasant and neutral blocks (4 cycles). Each block began with a 2-s written instruction (‘negative words’ or ‘neutral words’). Five word set trials were presented during each block, each appearing for 4 s with a 2-s inter-stimulus interval (ISI). During each ISI, a centrally placed fixation cross replaced the word set. A 30-s resting baseline preceded the first block of trials, and an 11-s resting period separated all subsequent blocks of trials. During each trial, a word set was projected to the centre of the subject’s field of view via a computer-controlled projection system that presented stimuli to a rear-projection screen. Subjects viewed stimuli projected onto the screen via a 4 × 10 cm2 mirror attached to a head coil and positioned about 6 cm from and directly above the subject’s eyes. Each word appeared twice over the course of the scan within a unique word set. Word sets were presented in a fixed pseudo-randomized order across the blocks with the condition that a word would not reappear until all words had been presented once. The position of a word within a word set was counterbalanced across presentation. The sequence of blocks of unpleasant and neutral trials was counterbalanced across subjects by reversing the trial order for four of the nine subjects. During the unpleasant blocks, subjects were instructed to select the most unpleasant word from the three negative words presented on each words set using their right hand. Subjects were instructed to base their decision on their personal knowledge of and experience with the concept. Similarly, during neutral blocks, subjects selected the word they deemed to be the most neutral (i.e., non emotional) from each word set using their right hand.
fMRI recognition memory task
Sixty additional new words were selected from the total sample to serve as distractors in the memory task (30 unpleasant and 30 neutral), matched for length and frequency. Together, 120 words (60 previously seen and 60 not previously seen) were presented on 12 alternating unpleasant and neutral blocks (6 cycles). Each block consisted of a fixed random sequence of 10 words, with a 0.50 probability of being a previously seen word. Each word was presented for 2 s and was immediately followed by the next word. A 20-s resting period preceded the first block and separate successive blocks in counterbalanced order.
Imaging acquisition and post processing of fMRI data
Images were acquired using a 1.5 T Philips MRI scanner, using a T2*-weighted block-design matrix. Echo-planar images (EPI) were acquired in a single session for each paradigm from 14 axial planes (thickness = 5 mm; inter-slice gap = 1 mm; matrix size 64 × 64; TR = 2 s), parallel to the AC–PC line. For the emotional-decision paradigm 188 images were acquired for the entire session. Each activation block consisted of 15 contiguous images and was repeated four times in each session (60 total images each for neutral and unpleasant stimuli); resting periods comprised eight images, and were repeated for a total of seven times. For the memory-decision paradigm 242 images were acquired for the entire session. Each activation block consisted of 10 contiguous images and was repeated six times in each session (60 total images each for neutral and unpleasant stimuli); resting periods comprised 10 images, and were repeated for a total of 11 times. The first 12 images of both tasks were discarded as ‘dummy scans’. Pre-processing steps comprised slice acquisition time correction, within-subject image realignment, spatial normalization to the MNI template (voxel size: 4 × 4 × 4 mm) and spatial smoothing using a Gaussian kernel (12-mm full-width at half-maximum). Data sets were rejected if head displacement was greater than 2 mm in any direction. The time series was high-pass filtered to remove low frequency noise. Changes in blood oxygenation level-dependent (BOLD) contrast associated with the performance of the cognitive tasks were assessed on a pixel-by-pixel basis using the general linear model and the theory of Gaussian fields. Significant hemodynamic changes for each contrast were assessed using t statistical parametric maps (SPMt). The intragroup activations and comparisons between groups were investigated using a random-effect analysis, with a one-sample or two-sample t test. Data processing and analysis were accomplished using Statistical Parametric Mapping (SPM2) software [38]. p value threshold was ≤0.05 corrected for multiple comparisons; extent threshold ≥5 contiguous voxels.
Results
Psychopathological and neuropsychological tests
There was no evidence of a significant difference between groups on anxiety state ratings and no significant increase in ratings from pre- to post-scanning. A significant difference between groups emerged for BDI scores indicating that the patient group showed more depressive symptomology than controls (t = 5.670; p = 0.001). However, all subjects' BDI scores were below the clinical cut-off (score greater than 16), indicating that no individual patient nor control subject was clinically depressed. There was no significant difference between groups in the Emotional Lability Questionnaire or on any neuropsychological test; data are presented in Tables 1 and 2.
Behavioural data
Subjects attended to the stimuli and responded to every trial as instructed for the entire duration of the scans. All subjects found the unpleasant word sets to be highly unpleasant, particularly when compared with the neutral word sets. During the memory recognition task, healthy subjects recognized significantly more unpleasant than neutral words: they detected 73% of the unpleasant words and 52% of neutral words, demonstrating a significant memory enhancement for unpleasant words (t = 2.270; p = 0.036). Conversely, our patients recognized 62% of the unpleasant and 50% of the neutral words presented, which was not significant (t = 1.534; p = 0.144). Data are shown in Table 3.
fMRI emotional decision task
Within subjects analyses
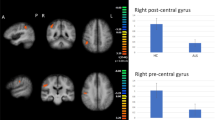
Unpleasant versus neutral words: the control group exhibited greater activation for unpleasant words versus neutral word stimuli in the left inferior parietal lobule (BA 40), right anterior cingulate gyrus (BA 32), and right middle frontal gyrus (MFG; BA 6). The ALS group revealed greater activation in the left-sided inferior frontal gyrus (BA 47), left precuneus (BA 7) and right anterior cingulate gyrus (BA 32). Data are shown in Fig. 1 and Table 4.

Brain areas more activated in healthy subjects (a) and ALS patients (b) during the emotional decision task (unpleasant vs. neutral words). Significant activations are overlaid onto two sagittal (left and right anatomical coordinates) standard MNI brain images, (areas are discussed in text; statistical parameters are reported in the text)
Between subjects analyses
Unpleasant versus neutral words: controls displayed greater activation as compared with patients in right MFG (BA 6). Conversely, patients showed significantly greater activation on left inferior frontal gyrus (BA 47) during unpleasant stimuli decision in comparison with controls. Data are shown in Table 5.
Unpleasant words versus rest: controls revealed greater activation in the right MFG (BA 9, 46) than patients when compared with rest. Conversely, patients showed greater activation in the left MFG (BA 10) in the same analyses.
Neutral words versus rest: a greater activation was shown in controls compared to patients in the left precentral gyrus (BA 6), right cerebellum and right parietal lobule (BA 39, 40). Patients displayed greater left MFG (BA 10, 11) activation in such analyses. (see Table 5).
fMRI memory recognition task
Within subjects analyses
Unpleasant words versus neutral words: the control group showed greater activation for unpleasant words versus neutral word stimuli in the bilateral insula (BA 13,) and right superior parietal lobule (BA 7). The ALS group revealed greater activation in the left middle frontal gyrus (BA 9), left inferior frontal gyrus (BA 47), left superior parietal lobule (BA 7), right anterior cingulate (BA 13), and right superior parietal lobule (BA 7). (Fig. 2; Table 4).

Brain areas more activated in healthy subjects (a) and ALS patients (b) during the memory recognition task (unpleasant vs. neutral words). Significant activations are overlaid onto two sagittal (left and right anatomical coordinates) standard MNI brain images, (areas are discussed in text; statistical parameters are reported in the text)
Between-subjects analyses
Unpleasant versus neutral words: The control group displayed significantly greater activation in the right superior parietal lobule (BA 7) for unpleasant stimuli in comparison with ALS subjects.
Unpleasant words versus rest: Controls revealed significantly greater activation of the right posterior cingulate (PC) gyrus in comparison with patients.
Neutral words versus rest: The control group displayed significantly greater activation in the right PC gyrus (BA10, BA11) for neutral stimuli in comparison with ALS subjects. Data are shown in Table 5.
Discussion
This study demonstrates a differential task-related activation in the neural networks underlying decision making (decision among unpleasant words and decision among neutral words) and recognition for emotional material (identification of known unpleasant or neutral stimuli vs. new unpleasant or neutral stimuli) in patients with ALS compared to healthy controls.
According to the literature [39, 40], in our control group, fMRI showed greater activation for unpleasant versus neutral words in the right hemisphere during the emotional decision and memory recognition tasks. On the contrary, while performing the same tasks, patients included in the study mainly revealed activation for negative words on the left hemisphere. The between-groups analysis confirmed significantly greater activation in left-sided inferior frontal gyrus of patients, while controls displayed significantly greater activation, as expected, in right-sided MFG, a cerebral region typically involved in language-related functions and particularly in emotional word processing [39, 41]. Findings of unpleasant words activation versus rest in patients compared to controls corroborated such lateralization (controls showed greater activation in the right MFG than patients; patients displayed greater activation in the left MFG than controls for same unpleasant words' selection). The between-subjects analysis for the unpleasant versus neutral words recognition confirmed significantly greater activation in controls compared to patients, in the right-sided superior parietal lobule, typically involved in mnesic functions. Moreover, greater activation for control subjects compared to ALS patients, in the right PC gyrus both for recognition of unpleasant and neutral stimuli when compared to rest was found. The PC gyrus has been implicated in the interaction of emotional and memory-related processes and receives strong afferent input from regions of the brain related to emotion and social behaviour (including the anterior cingulate, orbitofrontal and dorsolateral cortex, and the superior temporal sulcus) [41, 42].
A shortcoming of our study is that the fMRI parameters we adopted (i.e. the smoothing with a 12 mm Gaussian kernel) may not be ideal to distinguish activation in subcortical structures, presumably involved in emotional processing, in addition to the cortical areas mentioned above.
To summarize, our ALS patients showed an abnormal lateralization in emotional processing, mainly for unpleasant words, in terms of an increased brain activation in the left hemisphere and a reduced brain activation in the right hemisphere, compared to controls. This lateralization may indicate compensatory cognitive or neuroplastic changes. Dysfunction of frontal networks have been repeatedly observed in ALS [8], and classically includes frontal lobe atrophy and frontotemporal cortical hypometabolism that extends to the anterior cingulate gyrus [3]. However, the more lateralized right-sided reduced activation in ALS is more consistent with lateralized atrophy registered by some studies [4]. Murphy et al. [43] suggested the right hemispheric atrophy as a type of biomarker linked to behavioural abnormalities among patients with ALS. Patients with right hemisphere deficits exhibit an indifferent reaction, tending to deny the extent of their disabilities; this is a common trait observed in patients with ALS with behavioural disturbances [6, 10]. A recent conceptualization postulates that both hemispheres process emotions, but each hemisphere is specialized for a particular type of emotion, mainly in the frontal cortex. In one formulation of this approach, the left hemisphere is dominant for positive emotions whereas the right hemisphere is dominant for negative emotions [44]. This suggests that the abnormal functioning of the right hemisphere that we found in ALS may lead to difficulties in processing negative emotions. This was further supported by the behavioural data in which our ALS patients did not show the enhanced memory for the unpleasant versus neutral words in contrast to controls, indicating some dysfunction in emotional processing. Whether such changes in emotional processing underlie the behavioural symptoms which appeared prevalent in ALS, such as apathy, warrant further study. However, such dysfunction may imply neurodegeneration in key circuits related to emotional processing, mainly in the right hemisphere, supporting Murphy et al.'s [43] suggestion and confirming extra-motor involvement in ALS. Moreover, such findings further support the hypothesis of a link between ALS and FTD patients who present with widespread impairment in recognition of emotions, most marked for negative emotions [15].
The potential clinical implications on cognitive affective impairment in patients with ALS might have also a major importance and should be taken into account when patient care or experimental trials are planned, focusing on the patient's ability to evaluate emotional consequences and implications of therapeutic approaches, for them and their families.
References
Kew JJ, Goldstein LH, Leigh PN, Abrahams S, Cosgrave N, Passingham RE, Frackowiak RS, Brooks DJ (1993) The relationship between abnormalities of cognitive function and cerebral activation in amyotrophic lateral sclerosis. A neuropsychological and positron emission tomography study. Brain 116:1399–1423
Abrahams S, Goldstein LH, Kew JJ, Brooks DJ, Lloyd CM, Frith CD, Leigh PN (1996) Frontal lobe dysfunction in amyotrophic lateral sclerosis. A PET study. Brain 119:2105–2120
Abrahams S, Goldstein LH, Simmons A, Brammer M, Williams SC, Giampietro V, Leigh PN (2004) Word retrieval in amyotrophic lateral sclerosis: a functional magnetic resonance imaging study. Brain 127:1507–1517
Mezzapesa DM, Ceccarelli A, Dicuonzo F, Carella A, De Caro MF, Lopez M, Samarelli V, Livrea P, Simone IL (2007) Whole-Brain and regional brain atrophy in Amyotrophic Lateral Sclerosis. Am J Neuroradiol 28:255–259
Abrahams S, Goldstein LH, Suckling J, Ng V, Simmons A, Chitnis X, Atkins L, Williams SC, Leigh PN (2005) Frontotemporal white matter changes in amyotrophic lateral sclerosis. J Neurol 252:321–331
Abrahams S, Leigh PN, Goldstein LH (2005) Cognitive change in ALS: a prospective study. Neurology 64:1222–1226
Phukan J, Pender NP, Hardiman O (2007) Cognitive impairment in amyotrophic lateral sclerosis. Lancet Neurol 6:944–1003
Abrahams S, Goldstein LH, Al-Chalabi A, Pickering A, Morris RG, Passingham RE, Brooks DJ, Leigh PN (1997) Relation between cognitive dysfunction and pseudobulbar palsy in amyotrophic lateral sclerosis. J Neurol Neurosurg Psychiatry 62:464–472
Abrahams S, Leigh PN, Harvey A, Vythelingum GN, Grisé D, Goldstein LH (2000) Verbal fluency and executive dysfunction in amyotrophic lateral sclerosis (ALS). Neuropsychologia 38:734–747
Grossaman A, Wooley-Levine S, Bradley W, Milller R (2007) Detecting neurobehavioral changes in amyotrophic lateral sclerosis. Amyotroph Lateral Scler 8:56–61
Flaherty-Craig CV, Simmons Z (2004) Deficient social judgement in non-bulbar amyotrophic lateral sclerosis. Neurology 62:323–324
Gibbons ZC, Richardson A, Neary D, Snowden JS (2008) Behaviour in amyotrophic lateral sclerosis. Amyotroph Lateral Scler 9:67–74
Palmieri A, Abrahams S, Sorarù G, Mattiuzzi L, D’Ascenzo C, Pegoraro E, Angelini C (2009) Emotional Lability in MND: relationship to cognition and psychopathology and impact on caregivers. J Neurol Sci 278:16–20
Zimmerman EK, Eslinger PIJ, Simmons Z, Barrett AM (2007) Emotional perception deficits in amyotrophic lateral sclerosis. Cogn Behav Neurol 20:79–82
Snowden JS, Austin NA, Sembi S, Thompson JC, Craufurd D, Neary D (2008) Emotion recognition in Huntington’s disease and frontotemporal dementia. Neuropsychologia 46:2638–2649
Papps B, Abrahams S, Wicks P, Leigh PN, Goldstein LH (2005) Changes in memory for emotional material in amyotrophic lateral sclerosis. Neuropsychologia 43:1107–1114
Lulé D, Kurt A, Jurgens R, Kassubek J, Diekmann V, Kraft E, Neumann N, Ludolph AC, Birbaumer N, Anders S (2005) Emotional responding in amyotrophic lateral sclerosis. J Neurol 252:1517–1524
Lulé D, Diekmann V, Anders S, Kassubek J, Kübler A, Ludolph AC, Birbaumer N (2007) Brain responses to emotional stimuli in patients with amyotrophic lateral sclerosis (ALS). J Neurol 254:519–527
Brooks BR, Miller RG, Swash M, Munsat TL (2000) EL Escorial revisited: revised criteria for the diagnosis of amyotrophic lateral sclerosis. World Federation of Neurology Research Group on Motor Neuron Disease. Amyotroph Lateral Scler Other Motor Disord 1:293–299
Cederbaum JM, Stambler N, Malta E, Fuller C, Hilt D, Thurmond B, Nakanishi A (1999) BDNF ALS study group (Phase III). The ALSFRS-R: a revised als functional rating scale that incorporates assessments of respiratory function. J Neurol Sci 169:13–21
Beck Depression Inventory manual. 2nd edn. San Antonio: Psychological Corporation (1996). (Italian version: Manuale. Ghisi M, Flebus GB, Montano A, Sanavio E, Sica Firenze C: O. S.,2006)
Neary D, Snowden JS, Gustafson L, Passant U, Stuss D, Black S, Freedman M, Kertesz A, Robert PH, Albert M, Boone K, Miller BL, Cummings J, Benson DF (1998) Frontototemporal lobar degeneration: a consensus on clinical diagnostic criteria. Neurology 51:1546–1554
Williams SM (1986) Factor analyses of the Edinburgh handedness Inventory. Cortex 22:325–326
Folstein MF, Folstein SE, McHugh PR (1975) Mini Mental State: a practical method for grading the cognitive state of patiens for the clinician. J Psychiatr Res 12:189–190
Sartori G, Colombo L, Vallar G, Rusconi M L, Pinarello A (1997) T.I.B. Test di intelligenza breve per la valutazione del quoziente intellettivo attuale e pre-morboso. Giornale dell’ordine Nazionale Degli Psicologi
Raven JC (1965) RCPM: guide to using the coloured progressive matrices. Psychological Corp, New York
Spinnler H, Tognoni G (1987) Standardizzazione taratura italiana dei test neuropsicologici. Italian J Neurol Sci 8(Suppl):1–120
Nelson HE (1976) Modified Card Sorting Test. Firenze, Italy: O.S., Firenze (2003)
Reitan RM (1998) Validity of the trail making test as an indicator of organic brain damage. Percept Mot Skills 8:271–276
Sánchez-Cubillo I, Periáñez JA, Adrover-Roig D, Rodríguez-Sánchez JM, Ríos-Lago M, Tirapu J, Barceló F (2009) Construct validity of the Trail Making Test: role of task-switching, working memory, inhibition/interference control, and visuomotor abilities. J Int Neuropsychol Soc 15:438–450
Wechsler D (1998) Wechsler Adult Intelligence Scale Revised (WAIS-R). Versione Italiana a cura di Laicardi e Orsini. O.S., Firenze, Firenze, Italy
Warrington EK (1984) Recognition memory test. NFER-Nelson, Windsor
Kaplan EF, Goodglass H, Weintraub S (1983) The Boston Naming Test: The experimental edition. Boston: Kapan and Gooodglass (2nd edn Philadelphia: Lea & Fabiger)
Osterrieth PA (1944) Le test de copie d’une figure complex: contribution a l’etude de la perception et de la memoire. Arch Psichol 30:286–356
Tabert MH, Borod JC, Tang CY, Lange G, Wei TC, Johnson R, Nusbaum AO, Buchsbaum MS (2001) Differential amygdala activation during emotional decision and recognition memory tasks using unpleasent words: an fMRI study. Neuropsychologia 39:556–573
Spielberger CD, Gursuch RL, Lushene RE (1989) State-Trait Anxiety Inventory-Y Form. Italian Edition by Pedrabissi L and Santinello M. Firenze, Italy: O.S., Firenze
De Mauro T, Mancini F, Vedovelli M, Voghera M (1993) Lessico di frequenza d’uso dell’italiano parlato. Etas Libri, Milano
Friston KJ, Holmes AP, Worsley KJ, Poline J-P, Frith CD, Frackowiak RSJ (1995) Statistical parametric maps infunctional imaging: a general linear approach. Hum Brain Map 2:189–210
Cunningham WA, Raye CL, Johnson MK (2004) Implicit and explicit evaluation: fMRI correlates of valence, emotional intensity, and control in the processing of attitudes. J Cogn Neurosci 16:1717–1729
Kuchinke L, Jacobs AM, Võ ML, Conrad M, Grubich C, Herrmann M (2006) Modulation of prefrontal cortex activation by emotional words in recognition memory. Neuroreport 17:1037–1041
Fossati P, Hevenor SJ, Graham SJ, Grady C, Keightley ML, Craik F, Mayberg H (2003) In search of the emotional self: an FMRI study using positive and negative emotional words. Am J Psychiatry 160:1938–1945
Maddock RJ, Garrett AS, Buonocore MH (2003) Posterior Cingulate Cortex Activation by Emotional Words: fMRI evidence from a valence decision task. Hum Brain Map 41:18–30
Murphy JM, Roland GH, Langmore S, Kramer JH, Miller BL, Lomen-Hoerth C (2007) Continuum of frontal lobe impairment in Amyotrophic Lateral Sclerosis. Arch Neurol 64:530–534
Gur RC, Skolnick BE, Gur RE (1994) Effect of emotional discrimination tasks on cerebral blood flow: regional activation and its relation to performance. Brain Cogn 25:271–286
Acknowledgments
We acknowledge patients and their caregivers for their efforts to participate the study. This study was supported by ASLA Onlus (to G.S. and A.P.).
Conflict of interest statement
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Palmieri, A., Naccarato, M., Abrahams, S. et al. Right hemisphere dysfunction and emotional processing in ALS: an fMRI study. J Neurol 257, 1970–1978 (2010). https://doi.org/10.1007/s00415-010-5640-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00415-010-5640-2