
Abstract
Purpose
To identify whether biochemical pregnancy (BP) and spontaneous abortion (SA) cases have the same clinical characteristics in assisted reproductive therapy (ART), and to assess its predictive value for the subsequent cycles.
Methods
Retrospectively reviewed 12,174 cycles in the first in vitro fertilization and embryo transfer (IVF-ET) cycle from January 2009 to December 2012 of Peking University Third Hospital Reproductive Medical Center. Besides those patients who reached ongoing pregnancy stage, 7,598 cases were divided into three groups: group 1, lack of pregnancy (n = 6,651); group 2, BP (n = 520); and group 3, SA (n = 427). We compared the basic status of patients of the three groups, including ages, body mass index, basic hormone levels, controlled ovarian hyperstimulation protocols, amount of gonadotropin use, and endometrium thickness. The reproductive outcome of the next embryo transfer cycles of the three groups was analyzed.
Results
520 patients ended as BP, and 427 patients ended as SA. The age, primary infertility proportion, body mass index, basic FSH level and basic E2 level were similar among groups. Endometrial thickness, controlled ovarian hyperstimulation protocol, Gn dosage, average oocyte retrieval and ET numbers were also similar. Multivariate analysis showed that only the age (P = 0.037, OR 1.060, 95 % CI 1.001–1.120) and endometrium thickness on hCG administration day (P = 0.029, OR 1.136, 95 % CI 1.013–1.275) may result in the differences between BP and SA groups. In the subsequent ET cycles, the total BP rate was 4.37 %, clinical pregnancy rate was 37.28 %, and miscarriage rate was 8.18 %. The clinical pregnancy rates were similar among groups. However, BP group still had the highest BP rate (P < 0.05, 7.97 vs. 4.01 % and 5.28 %), BP and SA group had higher miscarriage rate (P < 0.05, 11.76 % and 14.75 vs. 7.41 %).
Conclusion
BP and SA in first IVF cycles had negative predictive value for subsequent ART outcomes.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Biochemical pregnancies (BPs) are pregnancies identified by a positive urine/serum hCG without a gestational sac that can be detected by ultrasound. In assisted reproductive therapy (ART), BP occurs when beta hCG levels increase post-embryo transfer, but later decrease and no gestational sac is detected. Despite the improvement of clinical pregnancy rate following in vitro fertilization and embryo transfer (IVF-ET), about 15–20 % of hCG positive cycles following IVF-ET result in BPs [1]. Various factors affecting early implantation may cause BPs, but it is unclear to what extent they should be included in the diagnostic criteria of spontaneous abortion (SA) and whether they have prognostic impact.
Studies showed that factors such as age, the oocyte and embryo quality, endometrium receptivity and infertile factors may have something to do with the occurrence of biochemical pregnancy post-ART [2–6]. There has been disagreement about the predictive value of BP in subsequent cycles [7–11].
The objective of this study was to identify whether BP and SA have the same clinical characteristics in patients that received embryo transfer, and thereby determine whether BP should be classified as spontaneous abortion, and to assess its predictive value for the subsequent cycles.
Materials and methods
Study objects
We reviewed 12,174 cycles in the first in vitro fertilization and embryo transfer (IVF-ET) cycle from January 2009 to December 2012 at Peking University Third Hospital Reproductive Medical Center. Enter criteria include that patients be younger than or equal to 38 years old, oocyte retrieval number between 5 and 20, and at least one good-quality embryo were transferred per cycle; excluding cases with a recurrent spontaneous abortion history (n = 104), and heterotopic and ectopic pregnancy cycles. Besides those patients who reached ongoing pregnancy stage, there were 7,598 cycles which were admitted in our study groups. Cases were divided into three groups: group 1, lack of pregnancy (n = 6,651); group 2, biochemical pregnancy (BP) (n = 520); and group 3, spontaneous abortion (SA) (n = 427) (Fig. 1).

Patients selection of study groups
Treatment protocol
Long agonist, antagonist and short agonist protocols for ovarian stimulation were performed as described elsewhere [12]. Human chorionic gonadotrophin (HCG) was administered when more than two follicles reached 18 mm, which was followed by oocyte retrieval 36–37 h later.
Embryo culturing was done using G5TM (Vitrolife; Göteborg, Sweden), Global (IVF Online; Toronto, Canada). Embryos were classified according to the number of blastomeres, percentage of fragmentation and blastomere appearances as type I, II, III or IV on first and third days. All embryos were transferred on third day following oocyte pickup. Regular luteal supports were given either 60 mg progesterone i.m. or vaginal progesterone (Crinone 8 % vaginal gel, Merck-Serono) daily [13].
A biochemical pregnancy (BP) was defined as HCG ≥25 IU/I that resolved spontaneously in the absence of ultrasound evidence of either an intrauterine or an ectopic pregnancy on 12–14 days after ET. A clinical pregnancy was determined by detection of embryo sac. The clinical SA group included all intrauterine pregnancies that were confirmed by ultrasound, but did not progress beyond the first trimester.
Study methods and statistical analysis
We compared the basic status of patients of the three groups, including patients’ ages, body mass index (BMI), infertile type and basic hormone levels. Controlled ovarian hyperstimulation (COH) protocols, amount of gonadotropin use, endometrium thickness and type on hCG administration day, numbers of oocytes retrieved and average ET, and clinical outcomes (concluding biochemical pregnancy, clinical pregnancies, early onset abortion rates) were also compared among groups. The reproductive outcome of the next IVF cycles of the three groups was analyzed.
Measurements are presented as mean ± standard deviation. For statistical analysis, we used the Statistical Package for Social Sciences (SPSS, version 16.0, SPSS Inc, Chicago, IL) for Windows. Univariate was done by student’s t test and Chi-square test (Fisher’s exact test), and multivariate analysis was done by logistic regression. A P value <0.05 was considered statistically significant.
Results
-
1.
A comparison of characteristics of the patients with different clinical outcomes in first cycles.
520 patients ended as biochemical pregnancy (4.31 %, 520/12,070), and 427 patients ended as SA (3.54 %, 427/12,070). The primary infertility proportion, body mass index, basic FSH and E2 levels were similar among groups. When divided into subgroups by 35 years, the age constituent ratios had no differences (Table 1).
-
2.
A comparison of COH of patients with different clinical outcomes in first IVF cycles.
All three groups had similar endometrial thickness ratios, and endometrial type proportion had no significant difference. COH protocol proportion and Gn dosage were similar among groups. All groups had similar average oocyte retrieval and ET numbers (Table 2).
-
3.
Multivariate analysis of the factors that may influence BP and SA occurrences by logistic regression.
The result showed only the age (P = 0.037, OR 1.060, 95 % CI 1.001–1.120) and endometrium thickness on hCG administration day (P = 0.029, OR 1.136, 95 % CI 1.013–1.275) can result in the differences between BP and SA groups (Table 3).
-
4.
The clinical outcomes of the subsequent IVF cycles for patients of the three groups.
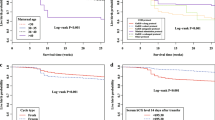
The numbers of subsequent ET cycles of the three groups were 5,066, 439, and 303, respectively. The average endometrium thickness and ET numbers were also similar among the three groups. The total biochemical pregnancy rate (4.37 %) and clinical pregnancy rate (37.28 %) were similar irrespective of the outcome achieved in the first cycle, and the miscarriage rate was 8.18 %. The clinical pregnancy rate and ectopic pregnancy rate were similar among groups (P > 0.05). However, group 2 still had the highest biochemical pregnancy rate [P < 0.05, 7.97 % (group 2) vs. 4.01 % (group 1) and 5.28 % (group 3)], group 2 and 3 had higher miscarriage rate than group 1 [P < 0.05, 11.76 % (group 2), 14.75 % (group 3) vs. 7.41 % (group 1)] (Table 4).
Discussion
Biochemical pregnancies are a relatively frequent phenomenon observed in assisted reproduction. The etiology of BP is not well understood, although either a problem of endometrial receptivity or an embryo of lower quality seems to be the most plausible cause [14]. Patients who resulted in BP usually have undergone a longer monitoring and treatment process. Clinical practices have suggested that more attention be paid to BP. Also here has been disagreement about whether BP should be considered an occurrence of SA.
Several factors are known to be associated with the pregnancy rate following IVF treatment including patients’ age, and elevated basic E2 level [13]. A Chinese study [15] showed that age and previous abortions are important factors that may contribute to the occurrences of BP in FET treatment cycles. Many studies focused on the endometrial receptivity that interfered with the BP occurrence in ART. Dickey [4] had reported that thin endometrium was associated with an increased risk of biochemical pregnancy following ART. Abdallah [5] had reported endometrial polyps smaller than 2 cm increase the risk of BPs in IVF cycles. A Chinese study [16] analyzed the clinical characteristics of BP and intrauterine pregnancy patients post-IUI, and found that endometrium receptivity was an important cause of BP occurrence. Yamada [17] and Fukui [18] had reported in recurrent spontaneous abortions and implantation failures cases, peripheral blood NK cell subsets percentage variation would lower endometrium receptivity.
Our study did not find significant differences of clinical characteristics among groups. The age, secondary infertility proportion, body mass index, basic FSH level and E2 level were similar among groups. The COH protocols proportion and endometrium thickness were also similar among the three groups. Multivariate analysis between BP and SA groups in our data showed only the age (P = 0.037, OR 1.060, 95 % CI 1.001–1.120) and endometrium thickness on hCG administration day (P = 0.029, OR 1.136, 95 % CI 1.013–1.275) can result in the differences between BP and SA groups.
Taylor [2] and Cai et al. [5] had reported that BP occurrence is related to embryo quality. In China, a study [19] analyzed the oocyte and embryo quality of 94 cases of BP and 177 cases of singleton pregnancy, which showed that the decrease of oocyte quality was an important cause of biochemical pregnancy. Others [4, 14] suggested that it is not embryo quality that leads to higher biochemical pregnancy rate. Our study included cycles in which at least one good-quality embryo was transferred.
There are several articles on how BP can predict subsequent cycles. Haas [20] reported BP and SA were positive markers for success in subsequent cycles in patients with repeated IVF failures. In the first three cycles, it did not significantly alter the chances to conceive (16.9 % patients with BP and/or SA in the previous cycle vs. 16.5 % patients with no previous pregnancy). From cycle 4 onwards, the presence of a previous abortion (either BP or SA) was associated with better ongoing pregnancy rate (23.0 vs. 11.2 %, P < 0.001). There are also articles showed BPs’ negative predictive value for subsequent cycles. Christiansen [11] had reported in patients with a history of only BPs, 27.1 % of all pregnancies were ectopic pregnancies whereas among recurrent miscarriage patients, the rates of ectopics were only 3.6 % (P < 0.0001). Serra [10] had reported a study which showed that previous BPs worsened the probability of having an initial ongoing pregnancy in the next cycles. In China, a study [21] showed that lymphocyte immunotherapy—a routine method for SA treatment—was a safe and effective treatment method for recurrent BP, which could result in a live birth rate as high as 71.1 %.
Our study so far has the biggest case sample to analyze BP’s and SA’s predicable value for next ET cycles. In the subsequent cycles of patients of non-pregnancy, BP and SA groups, the total biochemical pregnancy rate (4.37 %) and clinical pregnancy rate (37.28 %) were similar irrespective of the outcome achieved in the first cycle, and the miscarriage rate was 8.18 %. The clinical pregnancy rate and ectopic pregnancy rate were similar among groups (P > 0.05). But BP group still had the highest biochemical pregnancy rate, while BP and SA group patients had higher miscarriage rate than non-pregnancy group (P < 0.05). For prognostic value,a previous BP and SA in first IVF cycles do not seem to affect the chance of getting pregnant, but they worsen the outcomes in the next cycles by increasing the BP and SA occurrences. This result suggests that in clinical treatment, we need to tell those patients whose initial ART outcome is BP or SA that they may have a greater chance of a negative outcome in their subsequent cycles. They may need to have medical intervention to enhance their endometrium receptivity to improve the ART outcome.
In conclusion, BP and SA in first IVF cycles had similar negative predictive value for subsequent ART outcomes. BP cases will have higher BP and SA rates, while SA cases will have higher SA rate in next cycles.
References
Annan JJ, Gudi A, Bhide P et al (2013) Biochemical pregnancy during assisted conception: a little bit pregnant. J Clin Med Res 5(4):269–274
Taylor T, Eliott G, Wright J et al. (2004) Biochemical pregnancy occur more frequently when transferred embryo quality is diminished on day 3 irrespective to overall embryo quality: the role of positive selection. In: Abstracts of the 20th Annual Meeting of the ESHRE, Berlin, Germany, 27–30 June 2004, O-203
Dor J, Seidman DS, Ben-Shlomo I et al (1996) Cumulative pregnancy rate following in vitro fertilization: the significance of age and infertility aetiology. Hum Reprod 11:425–428
Dickey RP, Olar TT, Taylor SN et al (1993) Relationship of biochemical pregnancy to pre-ovulatory endometrial thickness and pattern in patients undergoing ovulation induction. Hum Reprod 8(2):327–330
Cai QF, Wan F, Huang R et al (2011) Factors predicting the cumulative outcome of IVF/ICSI treatment: a multivariable analysis of 2450 patients. Hum Reprod 26(9):2532–2540
Abdallah RT, Singer T, Huang J et al. (2010) Endometrial polyps smaller than 2 cm increase the risk of biochemical pregnancy in in-vitro fertilization (IVF) cycles. Fertil Steril S243:P-522
Kalu E, Thum MY, Abdalla H (2011) Prognostic value of first IVF cycle on success of a subsequent cycle. J Assist Reprod Genet 28(4):379–382
Bates GW Jr, Ginsburg ES (2002) Early pregnancy loss in in vitro fertilization (IVF) is a positive predictor of subsequent IVF success. Fertil Steril 77(2):337–341
Sneeringer R, Klipstein S, Ryley DA et al (2008) Pregnancy loss in the first in vitro fertilization cycle is not predictive of subsequent delivery in women over 40 years. Fertil Steril 89(2):364–367
Serra VS, Vidal C, Bellver J et al. (2006) Biochemical pregnancy: Clinical significance in assisted reproduction. Fertil Steril S145:P-87
Christiansen OB (2011) Biochemical pregnancies—shall they count in the recurrent miscarriage diagnosis? Symp Abstr/J Reprod Immunol 90(131–163):S45
Sunkara SK, Coomarasamy A, Khalaf Y et al (2007) A three-arm randomised controlled trial comparing Gonadotrophin releasing hormone (GnRH) agonist long regimen versus GnRH agonist short regimen versus GnRH antagonist regimen in women with a history of poor ovarian response undergoing in vitro fertilisation (IVF) treatment: poor responders intervention trial (PRINT). Reprod Health 4:12
Kara M, Aydin T, Aran T et al (2013) Comparison of GnRH agonist and antagonist protocols in normoresponder patients who had IVF-ICSI. Arch Gynecol Obstet 288(6):1413–1416
Troncoso C, Bosch E, Rubio C et al (2003) The origin of biochemical pregnancies: lessons learned from preimplantation genetic diagnosis. Fertil Steril 79(2):449–450
Long W, Yin TL, Zhao QH et al (2011) An analysis of biochemical pregnancy rate and its causes in frozen-thawed embryo transfer cycles (Electronic Edition). Chin J Clin 5(17):5154–5157
Zou L, Peng CL, Ma TZ et al (2014) The analysis on related factors of 53 intrauterine insemination cycles terminated in biochemical pregnancy or clinical pregnancy. Chin J Fam Plan Gynecotokol 6(1):58–60
Yamada H, Morikawa M, Kato EH et al (2003) Pre-conceptional natural killer cell activity and percentage as predictors of biochemical pregnancy and spontaneousabortion with normal chromosome karyotype. Am J Reprod Immunol 50(4):351–354
Fukui A, Kwak-Kim J, Ntrivalas E et al (2008) Intracellular cytokine expression of peripheral blood natural killer cell subsets in women with recurrent spontaneous abortions and implantation failures. Fertil Steril 89(1):157–165
Lin L, Quan S, Chen LN et al (2010) The Effects of oocyte and embryo quality on the occurrence of biochemical pregnancy. Guangdong Med J 31(19):2496–2498
Haas J, Lerner-Geva L, Yerushalmi GM et al (2012) Previous abortion is a positive predictor for ongoing pregnancy in the next cycle in women with repeated IVF failures. Reprod Biomed Online 25(4):339–344
Han LF, Zhang L, Jing WN et al (2006) An analysis of lymphocyte immune therapy on 38 cases of repeated biochemical pregnancy. J Pract Obstet Gynecol 22(5):316–317
Acknowledgments
We appreciate Dr. Lixue Chen for statistic support and Dr. Hai Na for his assistance in revision of the article.
Conflict of interest
The manuscript has been seen and approved by all authors and has no conflicts of interest for any of the authors.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Yang, R., Yang, S., Li, R. et al. Biochemical pregnancy and spontaneous abortion in first IVF cycles are negative predictors for subsequent cycles: an over 10,000 cases cohort study. Arch Gynecol Obstet 292, 453–458 (2015). https://doi.org/10.1007/s00404-015-3639-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00404-015-3639-8