
Abstract
Background
Total knee arthroplasty (TKA) is an efficient and common procedure used to treat advanced osteoarthritis of the knee. Geriatric patients make up the majority of TKA patients. For the surgical management of bilateral knee arthritis, there is still debate regarding whether to do a simultaneous or staged TKA. We through this study have gathered data and aimed to assess the safety of simultaneous bilateral TKA in patients.
Materials and methods
We conducted a study according to the PRISMA guidelines by searching through various databases for the following search terms: total knee arthroplasty (TKA), complications following TKA, bilateral TKA, and bilateral vs. unilateral TKA. The search included case series and clinical trials and excluded review articles, yielding 24 articles from the original search. We extracted data upon the outcomes in patients undergoing simultaneous bilateral TKA. We performed additional bias assessments to validate our search algorithm and results.
Results
One hundred and three published articles were identified, and twenty-four that included a total of 2, 18,385 patients were included in the meta-analysis. 93,074 patients underwent simultaneous bilateral TKA and 125,311 patients underwent staged bilateral TKA. Simultaneous bilateral TKA was associated with significantly increased mortality rate (P < 0.00001, Odd’s ratio [OR] 1.86, 95% Confidence interval [CI] 1.53–2.26), increased incidence of pulmonary embolism (P < 0.00001, OR 1.58, 95% CI 1.30–1.91), deep venous thrombosis (P < 0.00001, OR 1.31, 95% CI 1.17–1.46), and neurological complications (P < 0.002, OR 1.44, 95% CI 1.14–1.82). There were no significant differences in cardiac complications between both the procedures (P = 0.60, OR 0.93, 95% CI 0.70–1.23).
Conclusion
Staged bilateral TKA is associated with less complication rates as compared to simultaneous bilateral TKA. Hence, patients should be counselled and selected based on the risks respective to each strategy.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Total knee arthroplasty (TKA) is an efficient and common procedure used to treat advanced osteoarthritis of the knee. Geriatric patients make up the majority of TKA patients, with insurance beneficiaries accounting for around 75% of TKA procedures [1]. According to Cram et al. [2], between 1991 and 2010 there was a 161% rise in yearly TKA volume. This rise is attributable to the elderly population’s improvement in function, independence, and pain as well as the growing acceptance of invasive therapy [3, 4]. For the surgical management of bilateral knee arthritis, there is still debate regarding whether to do a simultaneous or phased total knee arthroplasty. When the procedure is performed at the same time, there is a higher risk of significant complications or even death, according to various studies. However, some researchers are of the opinion that there is little to no evidence linking simultaneous TKA to an increase in risks or complications. There have been inconsistent findings when simultaneous bilateral TKA and staged bilateral TKA have been compared in a few randomized and nonrandomized controlled trials [5,6,7,8].
After having a complete knee arthroplasty, four out of five patients are satisfied with the results [6]. However, geriatric patients with comorbidities may have higher risks and expenditures, which could prevent them from having as many elective orthopaedic surgeries. Patients who are 85 years or older are 41% less likely than younger patients to undergo TKA [1]. Older patients who did not have surgery made up nearly half of those who were not given TKA [7]. Age has a variable impact on surgical outcomes, according to previous studies [7,8,9,10,11], and there is no clear relationship between age and TKA candidacy.
Because of ethical concerns, it is challenging to conduct a controlled randomized trial of patients with bilateral knee arthritis. Furthermore, because patients with higher comorbidity are frequently thought to be undesirable candidates for simultaneous TKA and are typically excluded from studies of those procedures, many of the research addressing the problems linked to bilateral TKA may have selection bias. Last but not least, and perhaps most significantly, the majority of the studies had rather small sample sizes and were likely underpowered to detect differences between the two treatments choices due to the relative rarity of serious complications following TKA.
Through meta-analysis, data can be gathered to address important issues like the safety of bilateral TKA in patients over 75 years of age. We gathered the available published data using stringent selection criteria to see if the occurrence of severe complications and mortality varied between bilateral and staged TKA. To assess the safety of simultaneous bilateral TKA compared with staged bilateral TKA in patients, all randomized and nonrandomized trials that compared the two procedures were considered. A more accurate method of patient selection would be made possible by a greater comprehension of the advantages and disadvantages of TKAs in this group. In order to clarify the effect of age on total knee arthroplasty, we systematically reviewed and evaluated studies that investigated the association of age on surgical outcomes.
Materials and methods
Study selection and information source
In this study, we adhered to the PRISMA 2020 guidelines and the Cochrane Handbook for systematic reviews and meta-analyses [12, 13]. We conducted a comprehensive literature search using EMBASE, PubMed (MEDLINE), Cochrane, and Google Scholar to find peer-reviewed articles on bilateral TKA. Additionally, we manually searched the references of relevant articles, tables of contents from major orthopedic journals (2010–2023), and bibliographies of key arthroplasty textbooks, including “The Adult Knee,” “Campbell’s Operative Orthopaedics,” and “Joint Replacement Arthroplasty.“
We screened study titles and abstracts for potential inclusion, considering all studies comparing the safety of simultaneous bilateral TKA with staged bilateral TKA, irrespective of diagnosis, surgical approach, or prosthesis type. For studies with overlapping patient populations, the one with the longest follow-up was selected. Data on population characteristics, interventions, and outcomes were extracted, though variables such as weight, race, BMI, comorbidities, prior knee surgeries, surgical methods, anesthesia techniques, perioperative antibiotics, thromboembolic prophylaxis, and postoperative rehabilitation details were inconsistently reported. Our primary outcomes were mortality and major complications, including deep vein thrombosis, pulmonary embolism, neurological complications, and cardiac issues.
Data extraction
Every relevant detail that was presented in the studies was extracted after an independent evaluation, including but not limited to demographics, prior procedures, and information on thromboembolic and infection prevention, patient satisfaction, functional outcome, and complication rate. In each report, details were obtained regarding the characteristics of the investigated population. The number of patients who underwent a simultaneous or staged procedure, as well as any complications that were indicated and the requirement for revision surgeries, were also noted.
Statistical analysis
Odd ratios (ORs) or standard mean differences (SMDs) with associated 95% confidence intervals (CI) were estimated and pooled across trials to evaluate the disparity between the 2 approaches, with a value of P < 0.05 being considered significant. Using a forest plot, the meta-analysis of relevant variables was graphically summarized.
Publication bias was assessed by ROBIS tool. All analyses were performed using the RevMan 5.3 software.
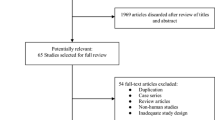
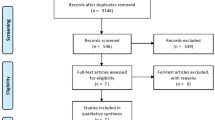
The last search was done in September 2023, and the following search terms were used: total knee arthroplasty (TKA), complications following TKA, bilateral TKA, and simultaneous bilateral vs. staged bilateral TKA. Additionally, we looked for any potentially pertinent studies using the “related articles” option. This method of searching produced 751 non-duplicated articles [Fig. 1].

PRISMA flowchart of the Meta-analysis
Results
In the search for research on the variables that affect Simultaneous bilateral TKA in patients, 848 citations were found; 751 citations were included after screening for duplicates. When inclusion and exclusion criteria were applied to abstracts, 648 articles were eliminated from the review. Following the application of inclusion and exclusion criteria to 103 full-length manuscripts, 24 articles were selected for review. Table 1 shows the relevant findings from these 24 publications.
The risk of bias was assessed using the ROBIS tool, and the findings revealed that the methods and outcomes of the literature search qualified for a low risk of bias [Table 2].
Eligible studies
A total of 24 articles were selected for inclusion in the meta-analysis [Table 1]. The published reports included information on 1, 86,054 patients. There were 2,18,385 patients included in the meta-analysis. 93,074 patients underwent simultaneous bilateral TKA, and 125,311 patients underwent staged bilateral TKA. Data on the rates of deep venous thrombosis in the two groups were provided by twelve articles [17, 18, 23,24,25,26,27,28,29,30,31, 35]. Thirteen articles reported on the prevalence of pulmonary embolism in the population under study [17, 18, 21, 23,24,25,26,27,28,29,30,31, 35]. The prevalence of cardiac complications was calculated using twelve trials [15,16,17,18, 24, 25, 27, 29, 30, 35,36,37]. Twenty studies provided data on the rate or prevalence of mortality in the sample [14, 15, 17, 18, 20,21,22,23,24,25,26,27,28,29,30, 32, 33, 35,36,37]. The two groups of patients were compared in terms of the prevalence of the five most serious complications: deep venous thrombosis, pulmonary embolism, cardiac events, neurological complications and mortality. The analysis revealed that, even though a large number of studies on this topic have been published, the overall conclusions are inconclusive. The reporting of the results, specifically the final odds ratio, varies significantly across the articles. The majority of the articles do not specify the exact age criteria for TKA.
Deep venous thrombosis
The risk of a deep venous thrombosis event was lower in patients after staged bilateral TKA, and this finding was statistically significant (P value < 0.00001, Odds ratio [OR] 1.31, 95% Confidence interval [CI] 1.17–1.46) [Fig. 2]. The pooled odds ratio was 1.31 overall. For a sample size of 1,33,000 patients the highest odds ratio was 3.74 in a study that did not have a significant impact on the overall result.

Forest plot for Deep venous thrombosis following simultaneous bilateral total knee arthroplasty
OR – Odd’s ratio, CI – Confidence interval, df – degree of freedom
Pulmonary embolism
Similar to the findings for deep venous thrombosis, the risk of pulmonary embolism was the higher in patients who had simultaneous bilateral TKA than in patients who had staged bilateral TKA (P value < 0.00001, OR 1.58, 95% CI 1.30–1.91) [Fig. 3]. Three of the articles made the most significant contributions to the overall calculation. After bilateral TKA, the highest odds ratio for pulmonary embolism was 12.05.

Forest plot for Pulmonary embolism following simultaneous bilateral total knee arthroplasty
OR – Odd’s ratio, CI – Confidence interval, df – degree of freedom
Cardiac complications
The likelihood of cardiac complications varied little between groups as well. The analysis of twelve articles revealed no increase in the prevalence of cardiac events in patients who underwent simultaneous bilateral TKA as compared to staged bilateral TKA (P value = 0.60, OR 0.93, 95% CI 0.70–1.23) [Fig. 4]. The highest odds ratio recorded was 1.64.

Forest plot for Cardiac complications following simultaneous bilateral total knee arthroplasty
OR – Odd’s ratio, CI – Confidence interval, df – degree of freedom
Mortality
The prevalence of mortality significant in the population that had undergone simultaneous bilateral TKA as compared to those who underwent staged bilateral TKA (P value < 0.00001, OR 1.86, 95% CI 1.53–2.26) [Fig. 5].

Forest plot for Mortality following simultaneous bilateral total knee arthroplasty
OR – Odd’s ratio, CI – Confidence interval, df – degree of freedom
Neurological complications
The prevalence of neurological complications were found to be higher in patients undergoing simultaneous bilateral TKA (P value < 0.002, OR 1.44, 95% CI 1.14–1.82) [Fig. 6].

Forest plot for Neurological complications following simultaneous bilateral total knee arthroplasty
OR – Odd’s ratio, CI – Confidence interval, df – degree of freedom
Discussion
TKA remains one of the most effective orthopaedic surgical procedures and is considered extremely safe. Although the majority of patients with knee arthritis undergo unilateral TKA, patients with symptomatic arthritis of both knees are not uncommon. The orthopaedic surgeon must then determine whether bilateral simultaneous TKA is a safe procedure to perform in this circumstance. Furthermore, the majority of patients suffering from knee arthritis are over the age of 60 years. Simultaneous Bilateral TKA in these patients is still being debated. There is a need to decide whether simultaneous TKA in patients is safe.
There are numerous benefits to performing simultaneous bilateral TKA in patients during a single anaesthetic session. Some of the benefits of this approach include patient convenience, a shorter length of stay in the hospital, and a potentially shorter period of rehabilitation and disability. On the other hand, some surgeons are hesitant to perform simultaneous bilateral TKA during a single anaesthetic session due to concerns about increased complications. When an orthopaedic surgeon searches the literature for information on the safety of simultaneous bilateral TKA, he or she may come across contradictory results. The apparent conflict noted in the literature could be caused by a number of factors. Because complications like pulmonary embolism are uncommon, the majority of studies have a type-II statistical error due to a small patient population. Furthermore, the effect of probable, and significant, selection bias cannot often be gleaned from these studies.
The investigators of a recent study attempted to overcome the aforementioned limitations by including a large patient sample [35]. In that study, patients who had simultaneous bilateral TKA had a higher incidence of pulmonary embolism than patients who had staged bilateral TKA. The incidence of pulmonary embolism in the first three months after arthroplasty was 1.45% in patients who had a single procedure compared to 0.77% in patients who had a staged bilateral TKA. Despite its strengths, this study suffered from the limitations inherent to analyses involving the Medicare database, as previously outlined. The Medicare database lacks important clinical information such as operative details. Hence, it was not possible for the investigators in that study to distinguish adequately between staged and simultaneous bilateral procedures.
As a result, this meta-analysis was carried out in order to combine data from a number of qualified studies in order to determine the prevalence of serious complications, including death, after bilateral TKA. The meta-analysis collected data and discovered that major complications such as pulmonary embolus, neurological events, deep venous thrombosis and death were significant after simultaneous bilateral TKA. The prevalence of cardiac complications appeared to be slightly lower after simultaneous bilateral TKA compared to staged bilateral TKA, but this difference was not statistically significant. This complication was not reported in all of the studies included in this meta-analysis. Although it was not a direct finding of this study, one could conclude that patients with concurrent cardiopulmonary conditions may not be good candidates for simultaneous bilateral TKA, even with recent advances in surgical and anaesthesia techniques.
Limitations
This study thoroughly examines the existing research on simultaneous bilateral TKA vs. staged bilateral TKA and the complications associated with the procedure. This study is unusual in its methodology and findings since, to our knowledge, there aren’t any reviews conducted in accordance with PRISMA standards that attempt to determine whether simultaneous bilateral TKA is safe patients. This study does, however, contain certain restrictions. Because of the difficulty in extracting the relevant information, this meta-analysis did not distinguish between simultaneous and staged bilateral total knee arthroplasty as a whole. Another potential limitation of this meta-analysis is related to the strict criteria for inclusion of randomized and comparative studies, as some potentially relevant studies may have been excluded. This step was necessary in order to eliminate important confounding variables. Finally, the meta-analysis was intended to evaluate the prevalence of major and life-threatening complications associated with simultaneous bilateral TKA. Hence, information on other complications such as periprosthetic infection or functional recovery was not sought. The majority of the studies did not provide information pertinent to these problems.
Based on our results, we recommend that the strategy for performing bilateral TKA should be carefully selected based on patient age, comorbidity profile and preference. Patients should be carefully counseled regarding the respective incidence of complications and consequent risks associated with each respective strategy. Further matched prospective studies comparing both clinical outcomes and patient reported outcomes following simultaneous bilateral TKA and staged bilateral TKA are required.
Conclusion
Staged bilateral TKA is associated with less complication rates as compared to simultaneous bilateral TKA. Hence, patients should be counselled and selected based on the risks respective to each strategy. However, there is a need for high-quality, prospective studies to better evaluate the clinical, functional and cost effectiveness of simultaneous bilateral TKA compared to staged bilateral TKA.
Data availability
This published article contains all the data generated or analyzed during this study.
References
Katz BPFD, Heck DA, Dittus RS, Paul JE et al (1996) Demographic variation in the rate of knee replacement: a multi-year analysis. Health Serv Res 31(2):125–140
Cram P, Lu X, Kates SL, Singh JA, Li Y, Wolf BR (2012) Total knee arthroplasty volume, utilization, and outcomes among Medicare beneficiaries, 1991–2010. JAMA 308(12):1227–1236
Kane RL, Saleh KJ, Wilt TJ, Bershadsky B (2005) The functional outcomes of total knee arthroplasty. J Bone Joint Surg Am 87(8):1719–1724
Skou ST, Roos EM, Laursen MB, Rathleff MS, Arendt-Nielsen L, Simonsen O et al (2015) A randomized, controlled trial of total knee replacement. N Engl J Med 373(17):1597–1606
Baker PN, van der Meulen JH, Lewsey J, Gregg PJ (2007) National Joint Registry for England and Wales. The role of pain and function in determining patient satisfaction after total knee replacement. Data from the National Joint Registry for England and Wales. J Bone Joint Surg (Br) 89(7):893–900
Hamel MB, Toth M, Legedza A, Rosen MP (2008) Joint replacement surgery in elderly patients with severe osteoarthritis of the hip or knee: decision making, postoperative recovery, and clinical outcomes. Arch Intern Med 168(13):1430–1440
Wilson M, Baig MK, Ashraf H (2005) Quality of life in octagenarians after coronary artery bypass grafting. Am J Cardiol 95(6):761–764
Finlayson EFZ, Birkmeyer JD (2007) Outcomes in octogenarians undergoing high risk caner operation: a national study. J Am Coll Surg 205(6):729–734
Alibakhshi A, Aminian A, Mirsharifi R, Jahangriri Y, Dashti H, Karimian F (2009) The effect of age on the outcome of esophageal cancer surgery. Ann Thorac Med 4(2):71–74
Oghalai J, Buxbaum JL, Pitts LH, Jackler RK (2003) The effect of age on acoustic neuroma surgery outcomes. Otol Neurotol 24(3):473–477
Yoshida GKT, Ishikawa Y, Matsumoto A, Ito Z, Tauchi R, Muramoto A et al (2013) The effects of surgery on locomotion in elderly patients with cervical spondylotic myelopathy. Eur Spine J 22(11):2545–2551
Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, page MJ, Welch VA (2019) Cochrane Handbook for Systematic Reviews of Interventions. 2nd edition. Chichester (UK): John Wiley & Sons
Soudry M, Binazzi R, Insall JN, Nordstrom TJ, Pellicci PM, Goulet JA (1985) Successive bilateral total knee replacement. J Bone Joint Surg Am 67:573–576
Mangaleshkar SR, Prasad PSV, Chugh S et al (2001) Staged bilateral total knee replacement—a safer approach in older patients. Knee 8:207–211
Ritter MA, Harty LD, Davis KE, Meding JB, Berend M (2003) Simultaneous bilateral, staged bilateral and unilateral total knee arthroplasty. A survival analysis. J Bone Joint Surg Am 85:1532–1537
Stubbs G, Pryke SE, Tewari S et al (2005) Safety and cost benefits of bilateral total knee replacement in an acute hospital. ANZ J Surg 75:739–746
Sliva CD, Callaghan JJ, Goetz DD, Taylor SG (2005) Staggered bilateral total knee arthroplasty performed four to seven days apart during a single hospitalization. J Bone Jt Surg Am 87:508e13. https://doi.org/10.2106/jbjs.D.02193
Hutchinson JR, Parish EN, Cross MJ (2006) A comparison of bilateral uncemented total knee arthroplasty: simultaneous or staged. J Bone Joint Surg Br 88:40–43
Barrett J, Baron JA, Losina E, Wright J, Mahomed NN, Katz JN (2006) Bilateral total knee replacement: staging and pulmonary embolism. J Bone Jt Surg Am 88:2146e51. https://doi.org/10.2106/jbjs.E.01323
Walmsley P, Murray A, Brenkel IJ (2006) The practice of bilateral, simultaneous total knee replacement in Scotland over the last decade. Data Scott Arthroplasty Project Knee 13:102–105
Forster MC, Bauze AJ, Bailie AG et al (2006) A retrospective comparative study of bilateral total knee replacement staged at a one-week interval. J Bone Joint Surg Br Vol 88:1006–1010
Stef ansdottir A, Lidgren L, Robertsson O (2008) Higher early mortality with simul- taneous rather than staged bilateral TKAs: results from the Swedish knee Arthroplasty Register. Clin Orthop Relat Res 466:3066e70. https://doi.org/10.1007/s11999-008-0404-3
Yoon H-S, Han C-D, Yang I-H (2010) Comparison of simultaneous bilateral and staged bilateral total knee arthroplasty in terms of perioperative complications. J Arthroplasty 25:179–185
Meehan JP, Danielsen B, Tancredi DJ et al (2011) A population-based comparison of the incidence of adverse outcomes after simultaneous bilateral and staged-bilateral total knee arthroplasty. J Bone Joint Surg Am 93:2203–2213
Bolognesi MP, Tyler Steven W, Attarian DE et al (2013) Simultaneous vs staged bilateral total knee arthroplasty among Medicare beneficiaries, 2000–2009. J Arthroplasty 28:87–91
Bini SA, Khatod M, Inacio MC et al (2014) Same-day versus staged bilateral total knee arthroplasty poses no increase in complications in 6672 primary procedures. J Arthroplasty 29:694–697
Courtney PM, Melnic CM, Alosh H et al (2014) Is bilateral total knee arthroplasty staged at a one-week interval safe? A matched case control study. J Arthroplasty 29:1946–1949
Niki Y, Katsuyama E, Takeda Y et al (2014) Comparison of postoperative morbidity between simultaneous bilateral and staged bilateral total knee arthroplasties: serological perspective and clinical consequences. J Arthroplasty 29:504–509
Lindberg-Larsen M, Jørgensen CC, Husted H et al (2015) Early morbidity after simultaneous and staged bilateral total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc off J Esska 23:831–837
Sheth DS, Cafri G, Paxton EW et al (2016) Bilateral simultaneous vs staged total knee arthroplasty: a comparison of complications and mortality. J Arthrop 31:212–216
Sobh AH, Siljander MP, Mells AJ et al (2018) Cost analysis, complications, and discharge disposition associated with simultaneous vs staged bilateral total knee arthroplasty. J Arthrop 33:320–323
Chua HS, Whitehouse SL, Lorimer M et al (2018) Mortality and implant survival with simultaneous and staged bilateral total knee arthroplasty experience from the Australian orthopaedic association national joint replacement registry. J Arthroplasty 33:3167–3173
Koh WU, Kim HJ, Park HS, Jang MJ, Ro YJ, Song JG (2018) Staggered rather than staged or simultaneous surgical strategy may reduce the risk of acute kidney injury in patients undergoing bilateral TKA. J Bone Jt Surg Am 100:1597e604. https://doi.org/10.2106/jbjs.18.00032
Wyatt MC, Hozack J, Frampton C, Hooper GJ (2019) Safety of single-anaesthetic versus staged bilateral primary total knee replacement: experience from the New Zealand National Joint Registry. ANZ J Surg 89:567e72. https://doi.org/10.1111/ans.15160
Tsay EL, Grace TR, Vail T, Ward D (2019) Bilateral simultaneous vs staged total knee arthroplasty: minimal difference in perioperative risks. J Arthroplasty 34:2944. https://doi.org/10.1016/j.arth.2019.07.002. e2949.e1
Richardson SS, Kahlenberg CA, Blevins JL, Goodman SM, Sculco TP et al (2019) Complications associated with staged versus simultaneous bilateral total knee arthroplasty: an analysis of 7747 patients. Knee 26:1096e101. https://doi.org/10.1016/j.knee.2019.06.008
Gill SD, Hill-Buxton L-M, Gwini SM, Morrison S, Moreira B, Beattie S et al (2020) Simultaneous (two-surgeon) versus staged bilateral knee arthroplasty: an observational study of intraoperative and post-operative outcomes. ANZ J Surg 90:826e32. https://doi.org/10.1111/ans.15766
Funding
No funding was received for the study.
Author information
Authors and Affiliations
Contributions
All authors have contributed equally to the preparation of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no financial conflicts of interest to disclose.
PRISMA 2020 checklist statement
The authors have read the PRISMA 20,020 Checklist, and the manuscript was prepared and revised according to the PRISMA 20,020 Checklist.
Consent for publication
Not Applicable.
Informed consent
Not Applicable.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Desouza, C., Shetty, V. Beyond one step: unveiling optimal approach for bilateral knee arthroplasty - a comprehensive meta-analysis. Arch Orthop Trauma Surg 144, 3631–3639 (2024). https://doi.org/10.1007/s00402-024-05454-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-024-05454-8