
Abstract
Introduction
Traumatic shoulder instability most frequently occurs in young people often during sports events. Currently, the arthroscopic Bankart repair is the therapy of choice in the absence of extensive glenoid bone loss and has proved to be a safe and effective procedure. Nevertheless, we see recurrence of instability—especially if new trauma happens—and further data are needed to guide the right decision-making for these often young patients. The purpose of this study was to determine the long-term outcome 10 years after arthroscopic Bankart operation in terms of satisfaction of the patient, functional result, complications, recurrent instability, and development of osteoarthritis, and to look after possible risk factors for recurrence of instability and statistical proof of these.
Materials and methods
Thirty-nine out of 49 patients underwent physical examination of both shoulders. We could perform a postoperative shoulder a-p X-ray in 28 patients. According to Samilson, [24] the extent of osteoarthritis was measured. The Constant score and the postoperative ROWE score were determined for both shoulders as well as the WOSI Score. In 25 cases, we calculated the ISIS Score.
Results
We could reach out to 89.6% of patients and 79.6% could be physically examined. The vast majority of 95.5% are either very satisfied or satisfied with the result at the time we ended the follow-up. The mean Constant score of 95.5 reflects this result. In contrast to this, we found at the same time in 15.3% ongoing clinical signs of instability of the concerning shoulder, even though 9.1% had to be re-operated for recurrent instability in between the follow-up timeline and we found in the X-rays (57.1% of all patients) in 35.7% at least moderate and in 10.7% severe signs of osteoarthritis. The Constant score but not the ROWE score differed significantly in patients with no or mild compared to those with moderate-to-severe osteoarthritis.
Conclusions
The arthroscopic Bankart stabilization procedure showed after 10 years to be a very safe operation and to be able to produce a satisfying and functional very good long-term result—reflected by the Constant score. We assume that the extent of osteoarthritis seems to be the determining factor of the very good functional result, even though ongoing instability was present in 15.3% of the patients.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Dislocation of the shoulder joint following trauma is the most common joint dislocation [1]. In most of these cases, the humeral head is pressed anteriorly and will injure the joint capsule [2]. After reposition, the capsular defect remains and leads to a weakening of the stability of the shoulder joint [3]. This may lead to recurrence of dislocation at much less traumatic force [4]. The inability to control and stabilize the shoulder is affecting not only the ability to perform in sports but also the daily life activities and the professional life performance as well [5, 6]. These broad implications in combination with the often very young age of affected patients lead to urgency in determining the right therapeutic measurements to stabilize the shoulder [7]. Historically, Perthes and then Bankart [8] were the first to find the capsulo-labral complex to be the most crucial stabilizing structure of the shoulder joint. Bankart performed the first series of open transosseous capsulo-labral repair and the outstanding results published in 1954 made his operation the gold standard of surgical intervention in case of traumatically caused shoulder instability. With the introduction of arthroscopic devices, the operation could be performed arthroscopically with suture anchors and optimal visualization without the potentially damaging effects to the deltoid muscle, the subscapular tendon, and even the axillary nerve [3]. Harris et al. compared the published results of the open and the arthroscopic procedure, and could not find significant differences in the outcome in respect of recurrent instability and return to the level of sports [9].
However, recurrent instability after surgical repair does happen [10], and in recent history, some authors reported studies with a follow-up timeline of 10 years with recurrence rates of instability of up to 30% [11].
Since we all try to provide the optimal result for the patient when considering surgical repair in terms of stability and risk of complications [12], especially in recurrent traumatic dislocation after a Bankart operation [13], the decision-making has to be done very carefully with the patient in good knowledge of the results [14].
Retrospectively, using the hospital data system, we contacted all of the 49 patients, which were operated upon in our institution between June 2006 and December 2008 with an arthroscopic Bankart repair after primary traumatic dislocation of the shoulder, to reveal information about the stability of the shoulder, possible complications and their ability to perform in sports, daily life, and professionally 10 years after the operation.
Materials and methods
Between June 2006 and December 2008, we performed 54 consecutive arthroscopic Bankart procedures at 54 patients in the hand of two surgeons. The inclusion criteria were primary traumatic shoulder instability and operative intervention in the above described time interval with the aim of a 10-year follow-up period and the exclusion criterion was recurrent instability with prior stabilizing operation (n = 5) of the concerning shoulder. 49 patients met the inclusion criteria and those were part of this study.
We started after the approval of the ethics committee of the medical faculty of the University of Heidelberg in May 30th 2017.
It turned out that five patients were not accessible because of change of address and phone number. Therefore, in 10.2%, we cannot provide with follow-up data.
The study was closed in February 15th 2019.
Records
The preoperative records of all 49 patients were reviewed and the date and cause of the initial trauma was determined. We classified the initial trauma in three classes: massive accident, direct hit, and distorsion trauma. The age at initial trauma and the age at the time of operation and all findings of the initial examination were collected including the number of dislocations prior operation, physical data like height and weight, the sports, and professional activities.
Operation
The arthroscopic operation was performed mostly in an ambulant setting in beach-chair position and general anesthesia in our institution. To re-fixate the capsulo-labral complex, we used Lupine loop anchors (DePuy, Mitek, Raynham, MA, United States). We would see all patients the next day. The shoulder was strictly immobilized in a Gilchrist shoulder-immobilizer for 3 weeks, and after that, the patient started physiotherapy according to our treatment regimen: week 4–6: passive shoulder mobilization with limitation in abduction 90° and external rotation 20°. Week 7–12: active and passive mobilization without limitation and begin with isometric strengthening of the scapula-stabilizing muscles as well as the rotator cuff. Since week 13: begin of dynamic strengthening of the scapulothoacic system and the rotator cuff with sport-specific training.
The operative records were checked for the width of the Hill–Sachs lesion [15] modified after the Callandra [16] classification and the width of glenoidal defects modified after the Itoi classification [16]. We looked after lesions of the long head of the biceps tendon and the rotator cuff. The intraoperative findings of gleno-humeral translation as a sign for hyperlaxity were classified after the Hawkins classification as well as the finding of a sulcus sign.
Physical examination
Forty-four patients were contacted and invited to the hospital. As stated above, we did not reach out to 5 of the patients because of change of address and phone number (10.2%). Thirty-three patients complied with our invitation (67.85%), and we asked about recurrence of instability, the sports activity, and the influence of the operated shoulder at the professional activity. Then, a thorough physical examination was performed by two observers with emphasis on instability. Both shoulders were examined. In case the patients had no time to come to the hospital, we fixed a date and made the physical exam and the interview at their place. In these six cases (12.24%), we could not perform the shoulder X-ray. Put together, 39 patients were physically examined and questioned (79.59%). Five of the contacted patients were not comfortable to be examined at all but would do the telephone interview and would fill out the questionnaire and send it back to us (10.2%)—so in 44 of 49 patients (89.6%), we know how they do and what happened to them in the follow-up time period.
X-rays of the shoulder
The preoperative shoulder X-rays could be collected of 25 patients (51.02%) and they were re-examined by two examinors after signs of osteoarthritis after Samilson [17] measuring Osteophytes in mm after standardizing with reference body and the bony lesions at the time of the operation including the presence of bony lesions of the glenoid rim and the extent of the Hill–Sachs lesion. At the hospital visit of the 33 patients, we performed a shoulder a-p X-ray in 28 patients (57.14%) to look after signs of osteoarthritis in similar fashion and measured cystic formations in the glenoid rim.
Measuring the scores
We measured the ROWE score for signs of recurrent instability, the Constant score for shoulder function for both shoulders and assessed the satisfaction of the patient. The force in N was measured as the average of three trials putting maximal force in holding the arm in 90° abduction in place while pulling upward with a Newton-meter. This was done for both shoulders. Retrospectively we calculated the ISIS score [18] for the 25 patients (51.02%) when preoperative X-rays were still available. The patient had to fill out a questionnaire to assess the subjective shoulder-related daily life and professional impairment with the Western Ontario Score-Index form.
Statistical analysis
For descriptive statistics, we summarized results for discrete variables in absolute and relative frequencies, while for continuous variables, we provided means, standard deviations, medians, and minimum and maximum values. For the comparison of continuous or ordinal variables (e.g., Constant score in patients with no-to-mild vs. moderate-to-severe osteoarthritis), descriptive p values of Mann–Whitney U tests were provided. Spearman correlation tests were applied to investigate potential correlations between continuous and/or ordinal variables. The conducted analyses and derived p values are purely exploratory and have no confirmatory value. Statistical analysis was performed using SAS Version 9.4.
Results
Of all 49 patients, the preoperative and the operative records were collected. We had 44 male (89.8%) and 5 female patients (10.2%). The mean age at the time of the initial dislocation was 26.1 years (median: 23 years, range: 15–65 years). The initial accident occurred at sports activities in 26 cases (53.06%) (Table 1).
The kind of trauma was classified as follows: massive accident: 2 cases (4.08%), direct hit to the shoulder: 25 cases (51.02%) and distorsion trauma: 22 cases (44.9%). 21 (42.86%) dislocations occurred at the right shoulder and 28 at the left (57.14%). In the median, two dislocations occurred till the operation took place (mean 16.2, range 1– > 200). After the initial dislocation, the median time-frame to operation was 5 months (mean 28.2, range 1–252 months).
We could recollect preoperative shoulder X-rays of 25 patients. Only in 1 case (4%), we found mild signs of glenoidal osteoarthritis. In one other case, there was a non-dislocated fracture of the greater tuberosity, which was treated conservatively. Four of the X-rays showed a small bony Bankart lesion (16%).
The mean age at time of the operation was 28.4 years (median: 27 years, range 16–65 years). All operations were performed under general anesthesia in beach-chair position arthroscopically. In any case, we used Lupine Loop anchors (DePuy Mitek). 45 patients received 2 anchors (91.83%), 1 only 1 anchor (2.04%), and 3 patients 3 anchors (6.12%). The reconstruction could be performed anatomical in 44 cases (89.8%); in 5 cases (10.2%), a neo-labrum out of the ruptured capsule had to be constructed. In addition to the labral repair, an interval closure was performed in 5 patients (10.2%). Refixation of the biceps anchor was done in 1 case (2.04%).
The intraoperative findings concerning capsular stability were as follows: the Shift Test according to Hawkins: 37 cases grade 1 (75.51%), 8 cases grade 2 (16.33%), and 4 cases grade 3 (8.2%). A positive sulcus sign was found in 15 patients (30.6%). Therefore, all-together signs of hyperlaxity were intraoperatively found in 18 patients (36.7%). Concerning the gleno-humeral pathway [19, 20], we looked after the Hill–Sachs lesion modified after Callandra [16] and found no obvious lesion in two patients (4.08%), Type 1 with a small lesion loco typico in 44 cases (89.8%), and a large but nonengaging lesion was found in 3 cases (Type 2) (6.12%). There was no case with an engaging lesion (25). A small bony Bankart fragment could be found in 4 cases (8.2%) (Itoi modified Type II) (11). The remaining findings are shown in Table 2.
As stated above, 39 patients (79.59%) were contacted and were open for physical examination. Five patients (10.2%) were only willing to give answers via telephone but were willing to fill out the questionnaire. Five (10.2%) patients could not be reached at all because of change of address and telephone number.
The mean follow-up time was 122.9 months (median: 124.5 months, range 105–141 months).
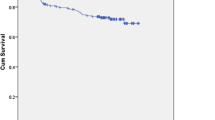
A re-dislocation after the operation took place in 7 patients of 44 we contacted (15.9%) (Fig. 1).

Recurrence of shoulder instability in the follow-up period
Only in one patient, the re-dislocation occurred in between the first 2 years after operation; all others appeared at or after 24 months postoperatively. Three of them (42.9%) were atraumatic and treated conservatively. Four had been traumatic (57.1%) and had to be re-operated. In three of these, a second arthroscopic Bankart operation, and in one case, an open Latarjet procedure was performed in our institution.
The physical examination in 39 patients revealed a reduction in passive external rotation of 74.7° (median: 80°) in comparison to the non-operated shoulder with 81.3° (median: 80°). All other findings of the physical examination are presented in Table 3.
A positive anterior apprehension sign was to be found in 6 patients (15.3%). Two of them did have a second arthroscopic Bankart operation during the follow-up interval and still experienced atraumatic instability (2 and 3 atraumatic re-dislocations, respectively). Three of the remaining four patients had either one or two atraumatic re-dislocations and one patient had no re-dislocation at all and did very well besides experiencing apprehension when tested. Therefore, all-together in 8 out of 39 patients (20.51%)—including the remaining 2 patients who were re-operated but showing no signs of recurrent instability at the time of the examination and doing very well so far—we found objective signs of recurrent instability after the initial Bankart operation.
Statistically, we could not find any of the clinical signs, including age, force of initial trauma, or number of dislocations prior to the operation as well as signs of hyperlaxity, to be significantly different in patients who experienced recurrent shoulder instability compared to patients without recurrent shoulder instability in the follow-up interval (Table 4).
The mean postoperative ROWE score [2] was 84.6 Points (median: 100 range 15–100) for the operated shoulder and 95.8 Points (median: 100 range 30–100) for the opposite side. The mean functional Constant score showed for the operated shoulder 95.5 Points (median: 100, range 88–100 Points) and for the opposite side 99.0 Points (median 100, range 88–100).
The good functional results being shown by the Constant score may reflect the high overall satisfaction rate of 30 patients very satisfied (68.2%), and 12 satisfied (27.3%) and only two were not satisfied with the result (4.5%).
The WOSI Scores of 44 Patients are shown in Table 5.
We used and summarized the raw points given by the patient to each questioned symptom ranging from 1 (no felt symptoms) to 10 (massive felt symptoms) for all 21 items. Therefore, the minimum summarized complaints are 21 points and the maximal are 210 for the 21 items. The subjective perception of the described signs and symptoms did inversely very well correlate to the postoperative ROWE Score as is to be expected (p = 0.0002, correlation coefficient = − 0.57). Interestingly it did also significantly correlate to the Constant score (p = 0.0007, correlation coefficient = − 0.52), as well. This was also the case for either the physical symptoms (Section A) (ROWE p = 0.0016, correlation coefficient = − 0.49, Constant score p = 0.0001, and correlation coefficient = − 0.57), the recreational and occupational activities (Section B) (ROWE p = 0.0005, correlation coefficient = − 0.53, Constant score p = 0.045, and correlation coefficient = − 0.32), the daily life activities (Section C) (ROWE p = 0.0005, correlation coefficient = − 0.53, Constant score p = 0.0008, correlation coefficient = − 0.51) and the allover perception of the concerning Shoulder (Section D) (ROWE p = 0.0006, correlation coefficient = − 0.53, Constant score p = 0.0095, and correlation coefficient = − 0.41). Figure 2 gives insight to the summarized WOSI Score points and the respecting constant scores of the patients.

Correlation between the WOSI scores and the Constant score
The postoperative X-ray of the operated shoulder could be obtained from 28 patients (57.14%). After Samilson [17], we measured the osteophytes in mm and found no signs of osteoarthritis in 3 patients (10.7%), mild arthritis in 12 patients (42.9%), moderate arthritis in 10 patients (35.7%), and severe arthritis in 3 cases (10.7%). Cystic formations in the glenoid rim were found in 3 patients (10.7%) ranging from 2 to 6 mm (Table 6).
The extent of the osteoarthritis 10 years after arthroscopic stabilization did not show differences in the ROWE score, or the WOSI scores.
When relating the functional status measured by the constant score of the shoulder to the extent of osteoarthritis, we found that the patients with high constant scores had less osteoarthritis (Fig. 3).

Extent of osteoarthritis in relation to the Constant score of the patients
To receive larger group sizes to apply U tests for group comparisons, we divided osteoarthritis into two groups. The first were patients with no or mild signs of osteoarthritis (n = 15) and the second group with moderate and severe osteoarthritis (n = 13). We could find that the patients with no or mild signs of osteoarthritis did show a significantly better Constant score compared to those with moderate or severe osteoarthritis (p = 0.038) (Fig. 4).

Correlation between the Constant score and osteoarthritis after dividing in two subgroups
We measured the ISIS score (2) in case the preoperative X-ray could be collected (n = 25) and we found only 1 patient (4%) to be > = 7. This patient luckily did very well and had no signs of recurrent instability and was very satisfied.
Concerning peri-operative complications, we found no infection or nerve lesions. Two patients complained about partial postoperative shoulder stiffness and were treated conservatively (4.5%).
Discussion
Instability of the shoulder joint is the most common cause of dysfunctional complaints in young people [1]. Either they experience a traumatic event, frequently during sports activities with a forceful dislocation or, especially in the developmental phase, there may be a dysbalance between the capsular strength and the forces put upon the shoulder, even without apparent trauma, causing pain and unwillingly dislocation of the joint [21]. Both cases lead to physical impairment and inability to perform in sports or in professional life [7]. After traumatic events, the arthroscopic Bankart repair is in most cases shown to restore stability of the shoulder with a low risk of operative complications [22]. This could be confirmed in our study. As in other publications [22, 23], we found 10 years after the operation at least one recurrent dislocation in 7 patients (16.3%) and recurrent instability in 8 patients we are aware of (20.3%). Patients who experienced a postoperative re-dislocation were in the median 21 years of age at the time of the operation compared to 26.5 years (median) to those who did not—although this was not statistically significant. In 4 of the 7 patients, the re-dislocations resulted from another traumatic event. Since these 4 patients did undergo a second operative stabilization, we could find at the time of the clinical assessment 10 years after the first operation 6 patients to still showing clinical signs of shoulder instability (15.4%). Three of these 6 nevertheless were very satisfied with the overall result—they have no shoulder pain and mostly adapted their sports activities, two were fairly satisfied, and only one was not satisfied because of ongoing signs of instability after having received 2 arthroscopic Bankart stabilization procedures.
Comparable long-term studies using the arthroscopic Bankart repair found a re-dislocation rate of 18.8% [24, 25] in a 13-year follow-up, in 8–10-year follow-up 35% [26], and others report a rate of 25% [27], 12% [28], and 5% [29], respectively. Lowering the follow-up time, of cause, reduces the reported re-dislocation rate to 8.2% [30] in a 3.5-year follow-up and 6.4% [31] in a 4.3-year follow-up. These results were also confirmed by our study, since the first re-dislocation was found taking place not earlier than 24 months after the initial operation (Fig. 1).
The physical examination revealed a mean postoperative ROWE score of 84.6 of the concerning shoulder and 95.8 of the opposite side. The mean Constant score was 95.5 and 99, respectively; in 39 patients, we were able to perform a physical examination on. In other studies, the postoperative ROWE-score ranged from 84.3 to 92 [11, 30,31,32]—mostly depending of the follow-up time. These scores are mostly a reflection of the recurrence of shoulder instability over time after the operation and are in line with our findings.
Since we could not reach out to physically examine all of the patients, we were happy to be delivered the completed WOSI Questionnaire and being able to add the subjectively felt symptoms to the medical history of the interview via telephone. We had an overall average WOSI score of 50.9 points ranging from 21 to 136 Points. This score had a significant inverse correlation with the ROWE score and the Constant score, as well [Fig. 2]. Patients with high ROWE and Constant scores showed significantly low WOSI scores points throughout almost every single item of the Questionnaire. These results may give proof of the quality of the data in our physical examination, but it suggests at the other side even only having the data of the Questionnaire without having the possibility to perform a physical examination to be able to have a very good insight to the concerning shoulder problem.
In 28 patients (57.14%), we were able to perform a shoulder X-ray at the time of the visit in our clinic. We found, measuring the osteophytes after Samilson [17] in mm by two observers, no or only mild signs of osteoarthritis in 15 patients (53.6%). Moderate osteoarthritis was present in 10 (35.7%) and severe osteoarthritis in 3 cases (10.7%). Adding the moderate and the severe cases, 46.6% showed explicit signs of osteoarthritis. In other long-term studies, moderate-to-severe osteoarthritis was present in 10–40% [11, 27, 33]. The high percentage of explicit osteoarthritis in our study may be due to the fact that of the 39 patients we saw and could perform a physical examination on; only 28 were able and willing to do the X-ray. Six patients were visited at their place and we could not perform the X-ray—all of those were very satisfied with the result of the operation. The remaining 5 patients in the clinical setting mostly denied it, because they had no problems with the shoulder and claimed to still be very young and therefore did not want to get exposed to radiation. It is reasonable to assume that in these 11 patients, we would have found no or only mild signs of osteoarthritis.
Finally, we looked after the clinical effect of the measured osteoarthritis. We divided into two groups—one with no or mild and one with moderate and severe osteoarthritis and applied a U test for group comparison of the ROWE and the Constant score data. No difference was observed for the ROWE score, but for the Constant score (Fig. 3)—divided into 2 subgroups—patients with no-to-mild osteoarthritis showed significantly higher Constant scores compared to patients with moderate-to-severe osteoarthritis (Fig. 4). These results may show that the functional status of the shoulder—represented by the Constant score—10 years after stabilization operation—is more dependent of the osteoarthritis than still on instability.
Conclusion
This is a retrospective long-term study of the outcome of a series of 49 consecutive arthroscopic Bankart operations on 49 patients. In the interval of a median 124.5 months later, we found 7 cases with at least one recurrent dislocation of the shoulder—4 of these caused by new severe trauma. Only 3 have been atraumatic. Overall, there is a high satisfaction rate confirmed by the median Constant score of 98. We found no case of infection or nerve lesion or any major complication. This result confirms that this operation is very safe and very effective. Nevertheless, digging deeper, we found at the reexamination after 10 years in 6 patients clinical signs of ongoing instability and in 13 patients moderate or severe signs of osteoarthritis.
Limitations
The biggest limitation of this study is the incomplete data set. Most of the patients with traumatic shoulder instability are young people. Reaching out to them 10 years after the operation is a really difficult task and not in all cases possible. But even after having contact by mail or telephone—they may live far away now—they may feel well with the shoulder and so do not see the need to come to the hospital for scientific reasons. The more symptomatic they are, the easier it is to move them back to the hospital for examination and make an X-ray of the shoulder. Furthermore, we did not have a control group. There are only 5 women, and in about half of all patients, it was a sports accident causing the instability. This is a very heterogeneous group. There is a big variation of the age when the accident took place. In addition to this, there is a big variation in the timeline between first traumatic shoulder dislocation and the operation, and there is a large variety of number of dislocations until the operation took place.
References
Zacchilli MA, Owens BD (2010) Epidemiology of shoulder dislocations presenting to emergency departments in the United States. J Bone Jt Surg Am 92(3):542–549
Rowe CR (1980) Acute and recurrent anterior dislocation of the shoulder. Orthop Clin North Am 11(2):253–270
Burkhart SS, De Beer JF (2000) Traumatic glenohumeral bone defects and their relationship to failure of arthroscopic Bankart repairs: significance of the inverted-pear glenoid and the humeral engaging Hill-Sachs lesion. Arthroscopy 16(7):677–694
Robinson CM, Howes J, Murdoch H, Will E, Graham CJ (2006) Functional outcome and risk of recurrent instability after primary traumatic anterior shoulder dislocation in young patients. J Bone Jt Surg Am 88(11):2326–2336
Robinson CM, Jenkins PJ, White TO, Ker A, Will E (2008) Primary arthroscopic stabilization for a first-time anterior dislocation of the shoulder: a randomized, double-blind trial. J Bone Jt Surg Am 90(4):708–721
Hovelius L, Saeboe M (2009) Neer Award 2008: arthropathy after primary anterior shoulder dislocation—223 shoulders prospectively followed up for twenty-five years. J Shoulder Elbow Surg 18(3):339–347
Roberts SB, Beattie N, McNiven CM, Robinson CM (2015) The natural history of primary anterior dislocation of the glenohumeral joint in adolescence. Bone Jt J. 97-B(4):520–526
Bankart ASB (1923) Recurrent or habitual dislocation of the shoulder-joint. Br Med J 2(3285):1132–1133
Harris JD, Gupta AK, Mall NA, Abrams GD, McCormick FM, Cole BJ, Bach BRJR, Romeo AA, Verma NN (2013) Long-term outcomes after bankart shoulder stabilization. Arthroscopy 29(5):920–933
Castagna A, Markropoulos N, Conti M, Delle Rose G, Papadakou E, Garofalo R (2010) Arthroscopic bankart suture-anchor repair: Radiological and clinical outcome at minimum 10 years of follow-up. Am J Sports Med 38(10):2012–2016
Murphy AI, Hurley ET, Hurley DJ, Pauzenberger L, Mullett H (2019) Long-term outcomes of the arthroscopic bankart repair: a systematic review of studies at 10-year follow-up. J Shoulder Elbow Surg 28(11):2084–2089
Bhatia S, Frank RM, Ghodadra NS, Hsu AR, Romeo AA, Bach BR Jr, Boileau P, Provencher MT (2014) The outcomes and surgical techniques of the latarjet procedure. Arthroscopy 30(2):227–235
Shin SJ, Ko YW, Lee J (2016) Intra-articular lesions and their relation to arthroscopic stabilization failure in young patients with first-time and recurrent shoulder dislocations. J Shoulder Elbow Surg 25(11):1756–1763
Zimmermann SM, Scheyerer MJ, Farshad M, Catanzaro S, Rahm S, Gerber C (2016) Long-term restoration of anterior shoulder stability: a retrospective analysis of arthroscopic Bankart repair versus open latarjet procedure. J Bone Jt Surg Am 98(23):1954–1961
Widjaja AB, Tran A, Bailey M, Proper S (2006) Correlation between Bankart and Hill-Sachs lesions in anterior shoulder dislocation. ANZ J Surg 76(6):436–438
Horst K, Von Harten R, Weber C, Andruszkov H, Pfeifer R, Dienstknecht T, Pape HC (2014) Assessment of coincidence and defect sizes in bankart and hill-sachs lesions after anterior shoulder dislocations: a radiological study. Br J Radiol 87(1034):20130673
Samilson RL, Prieto V (1983) Dislocation arthropathy of the shoulder. J Bone Jt Surg Am 65(4):456–460
Balg F, Boileau P (2007) The instability severity index score. A simple pre-operative score to select patients for arthroscopic or open shoulder stabilization. J Bone Jt Surg (Br). 89(11):1470–1477
Trivedi S, Pomerantz ML, Gross D, Golijanan P, Provencher MT (2014) Shoulder instability in the setting of bipolar (glenoid and humeral head) bone loss: the glenoid track concept. Clin Orthop Relat Res 472(8):2352–2362
Yamamoto N, Itoi E, Abe H, Minagawa H, Seki N, Shimada Y, Okada K (2007) Contact between the glenoid and the humeral head in abduction, external rotation and horizontal extension: a new concept of glenoid track. J Shoulder Elbow Surg 16(5):649–656
Pötzl W, Thorwesten L, Götze C, German S, Steinbeck J (2004) Proprioception of the shoulder joint after surgical repair for instability: a long-term follow-up study. Am J Sports Med 32(4):425–430
Williams HLM, Evans JP, Furness ND, Smith CD (2019) It’s not all about redislocation: a systematic review of complications after anterior shoulder stabilization surgery. Am J Sports Med 47(13):3277–3283
Rowe CR, Patel D, Southmayd WW (1978) The Bankart procedure: a long-term end-result study. J Bone Jt Surg Am 60(1):1–16
Aboalata M, Plath JE, Seppel G, Juretzko J, Vogt S, Imhoff AB (2017) Results of arthroscopic Bankart repair for anterior-inferior shoulder instability at 13-year follow-up. Am J Sports Med 45(4):782–787
Plath JE, Aboalata M, Seppel G, Juretzko J, Waldt S, Vogt S, Imhoff AB (2015) Prevalence of and risk factors for dislocation arthropathy: radiological long-term outcome of arthroscopic Bankart repair in 100 shoulders at an average 13-year follow-up. Am J Sports Med 43(5):1084–1090
Van der Linde JA, Van Kampen DA, Terwee CB, Dijksman LM, Kleinjan G, Willems WJ (2011) Long-term results after arthroscopic shoulder stabilization using suture anchors: an 8- to 10-year follow-up. Am J Sports Med 39(11):2396–2403
Privitera DM, Bisson LJ, Marzo JM (2012) Minimum 10-Year follow-up of arthroscopic intra-articular Bankart repair using bioabsorbable tacks. Am J Sports Med 40(1):100–107
Yapp LZ, Nicholson JA, Robinson CM (2020) Primary arthroscopic stabilization for a first-time anterior dislocation of the shoulder: long-term follow-up of a randomized, double-blinded trial. J Bone Jt Surg Am 102(6):460–467
Gill TJ, Micheli LJ, Gebhard F, Binder C (1997) Bankart repair for anterior instability of the shoulder. Long term outcome. J Bone Jt Surg (Am). 79(6):850–857
Pötzl W, Witt KA, Hackenberg L, Marquard B, Steinbeck J (2003) Results of suture anchor repair of anteroinferior shoulder instability: a prospective clinical study of 85 shoulders. J Shoulder Elbow Surg 12(4):322–326
Milchteim C, Tucker SA, Nye DD, Lamour RJ, Liu W, Andrews JR, Ostrander RV (2016) Outcomes of Bankart repairs using modern arthroscopic technique in an athletic population. Arthroscopy 32(7):1263–1270
Moroder P, Odorizzi M, Pizzinini S, Demetz E, Resch H, Moroder P (2015) Open Bankart Repair for the treatment of Anterior Shoulder Instability without substantial Osseous Glenoid Defects: Results After a Minimum Follow-up of Twenty Years. J Bone Jt Surg Am 97(17):1398–1405
Hovelius L, Vikerfors O, Olofsson A, Svensson O, Rahme H (2011) Bristow-latarjet and bankart: a comparative study of shoulder stabilization in 185 shoulders during a seventeen-year follow-up. J Shoulder Elbow Surg 20(7):1095–1101
Funding
No funding was received to assist with the preparation of this manuscript. No funding was received for conducting this study. No funds, grants, or other support was received. This study was approved by the ethics committee of University of Heidelberg Mannheim 4th of July 2017. All authors are informed and approve the publishing of this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
This study was performed comlying with the following ethical standards. The authors have no relevant financial or non-financial interests to disclose. The authors did not receive support from any organization for the submitted work.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Zink, S., Pfeiffenberger, T., Müller, A. et al. The arthroscopic Bankart operation: a 10-year follow-up study. Arch Orthop Trauma Surg 142, 3367–3377 (2022). https://doi.org/10.1007/s00402-021-04282-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-021-04282-4