
Abstract
Introduction
The purpose of this systematic review and meta-analysis was to evaluate the efficacy of concurrent cartilage procedures during high tibial osteotomy (HTO) for medial compartment osteoarthritis (OA) by comparing the outcomes of studies that directly compared the use of HTO plus concurrent cartilage procedures versus HTO alone.
Materials and methods
Results that are possible to be compared in more than two articles were presented as forest plots. A 95% confidence interval was calculated for each effect size, and we calculated the I 2 statistic, which presents the percentage of total variation attributable to the heterogeneity among studies. The random effects model was used to calculate the effect size.
Results
Seven articles were included to the final analysis. Case groups were composed of HTO without concurrent procedures and control groups were composed of HTO with concurrent procedures such as marrow stimulation procedure, mesenchymal stem cell transplantation, and injection. The case group showed a higher hospital for special surgery score and mean difference was 4.10 [I 2 80.8%, 95% confidence interval (CI) − 9.02 to 4.82]. Mean difference of the mechanical femorotibial angle in five studies was 0.08° (I 2 0%, 95% CI − 0.26 to 0.43). However, improved arthroscopic, histologic, and MRI results were reported in the control group.
Conclusion
Our analysis support that concurrent procedures during HTO for medial compartment OA have little beneficial effect regarding clinical and radiological outcomes. However, they might have some beneficial effects in terms of arthroscopic, histologic, and MRI findings even though the quality of healed cartilage is not good as that of original cartilage. Therefore, until now, concurrent procedures for medial compartment OA have been considered optional. Nevertheless, no conclusions can be drawn for younger patients with focal cartilage defects and concomitant varus deformity. This question needs to be addressed separately.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
High tibial osteotomy (HTO) is a surgical technique that unloads the affected compartment and aims to relieve pain and improve function in medial compartment osteoarthritis (OA). During the surgery, the degenerative cartilage is frequently observed in the involved compartment and many methods (injection, marrow stimulation techniques, osteochondral autograft and allograft, and autologous chondrocyte implantation) have been tried to promote cartilage regeneration in the hope of delaying the progress of the osteoarthritis [5, 19].
For healing of the degenerative cartilage, both mechanical status and biologic potential are important. However, in the osteoarthritic knee, most cartilage lesions consist of degenerative articular cartilage and eburnated bone is eventually exposed [17]. Repaired tissue of the eburnated bone has been reported to be healed with fibrocartilage, which has poorer quality than hyaline cartilage [17]. In addition, several articles have reported that regeneration of the articular cartilage with clinical improvement was obtained by unloading the involved part using HTO alone [1, 6, 10, 12]. Therefore, controversy exists regarding the use of HTO in association with concurrent procedures for medial compartment OA [1, 14].
Cartilage regeneration after HTO is also a controversial factor for clinical outcomes [11]. Some studies reported no correlation between clinical outcomes and the extent of cartilage regeneration [1, 12, 17]. Therefore, it is questionable whether we should perform concurrent procedures during HTO for medial compartment OA. Therefore, we intended to search for evidence by performing a thorough analysis of the usefulness of concurrent cartilage procedures during HTO. The purpose of this systematic review and meta-analysis was to evaluate the efficacy of concurrent cartilage procedures during HTO for medial compartment OA by comparing the outcomes of studies that directly compared the use of HTO plus concurrent cartilage procedures versus HTO alone. The hypothesis was that concurrent cartilage procedures would produce little benefit compared with HTO alone, and therefore, concurrent cartilage procedures would not be necessary during HTO for medial compartment OA.
Materials and methods
Search strategy
To test the hypotheses, a rigorous and systematic approach according to the preferred reporting items for systematic review and meta-analysis (PRISMA) guidelines was used [13]. In phase 1 of the PRISMA search process, the MEDLINE, EMBASE, and Cochrane database were systematically searched (August 2016). Using a Boolean strategy, all field search terms included the following: search ((((((((((cartilage) OR chondral) OR chondro) OR injection) OR intraarticular injection) OR microfracture) OR drilling) OR chondroplasty) OR abrasion arthroplasty)) AND ((((tibia) OR high) OR proximal) AND osteotomy). The citations in the included studies were screened, and we also checked unpublished articles with hand searches. The bibliographies of the relevant articles were subsequently cross-checked for articles not identified in the search. In phase 2, abstracts and titles were screened for their relevance. In phase 3, the full text of the selected studies was reviewed to assess for the inclusion criteria and methodological appropriateness with a predetermined question. In phase 4, the studies underwent a systematic review process and meta-analysis, if appropriate.
Eligible criteria
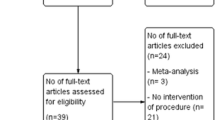
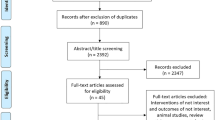
The inclusion criteria were as follows: (1) articles written in English, (2) studies reporting clinical and/or radiological results that are comparable to other studies, and (3) case–control studies regarding concurrent procedures (injection, transplantation, marrow stimulation procedure, osteochondral transfer, and chondrocyte implantation) during HTO for medial compartment OA (Fig. 1).

The PRISMA flow chart
Data extraction
Each of the selected studies was evaluated by two independent authors for methodological quality. Data were extracted according to the following: level of evidence, follow-up, composition of the case and control, method of control selection, enrollment, osteotomy type, site of concurrent procedure, clinical results, radiological results, arthroscopic finding, histologic finding, MRI finding and summary. The extracted data were subsequently cross-checked for accuracy; any disagreements were settled by the third review author.
Quality assessment
The methodological quality of the non-randomized case–control study was assessed using a Newcastle–Ottawa assessment scale. It consisted of three main domains (selection, comparability, and outcome), with four categories in the selection domain, one category in the comparability domain, and three categories in the outcome domain. A study was awarded a maximum of one star for each item within the selection and outcome domains. A maximum of two stars was given for comparability.
The methodological quality of the randomized controlled trials (RCT) was assessed using risk of bias (ROB), based on the Cochrane handbook, with the following nine standard criteria: allocation sequence generation, allocation concealment, baseline outcome measurement, baseline characteristics, incomplete outcome data, knowledge of the allocated interventions, protection against contamination, selective outcome reporting, and other ROB. Each criteria was scored as “Yes (low ROB)”, “No (high ROB)”, or “Unclear”.
Statistical analysis
Statistical analysis regarding clinical and radiological results between case and control group was performed using R version 3.1.1 (The R Foundation for Statistical Computing). Results that are possible to be compared in more than two articles were presented as forest plots. A 95% confidence interval (CI) was calculated for each effect size, and we calculated the I 2 statistic, which presents the percentage of total variation attributable to the heterogeneity among studies. The random effects model was used to calculate the effect size rather than the fixed-effect model because studies within each subgroup were not assumed to share a common effect size.
Results
Search
Seven articles were included to the final analysis. There were four RCT [2, 14, 18, 19] studies and three non-randomized case–control [1, 3, 7] studies. There were one level I, three level II, and three level III studies. All case groups were composed of HTO without concurrent procedures for medial compartment OA. All control groups were composed of HTO with concurrent procedures for medial compartment OA and they were concurrent marrow stimulation procedure, mesenchymal stem cell transplantation, and injection. Open-wedge HTO was performed in six studies and dome osteotomy was performed in one study (Table 1).
Quality assessment
Quality assessment details are presented in Table 2. Three non-randomized case–control studies were assessed using a Newcastle–Ottawa assessment scale. In the selection domain, all studies showed a low ROB except for one study that star was not awarded in category of selection of the non-exposed cohort. In the comparability domain, two studies were awarded two stars and one study was awarded one star. In the outcome domain, all studies were awarded one star except for one study that star was not awarded in the category of assessment of outcome and adequacy of follow up. Four RCTs were assessed using ROB, based on the Cochrane handbook. Eight criteria were scored as “Yes” in two studies. However, three categories were scored “No” in one study and one category was scored “No” in another one study.
Clinical results
Clinical results are presented in Table 3. Clinical results were reported in all seven studies. They were reported as hospital for special surgery (HSS) scores, Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), knee society knee score (K), knee society function score (F), Japanese orthopedic association (JOA), Tegner, and international knee documentation committee (IKDC) scores. In six studies, clinical results showed no statistically significant differences between groups. One study that performed mesenchymal stem cell injection as a concurrent procedure reported some additional effect of treatment in IKDC, Lysholm, and Tegner score [19]. Pooled analysis was possible only for HSS scores (Fig. 2). The case group showed a higher HSS score and mean difference was 4.10 [I 2 80.8%, 95% confidence interval (CI) − 9.02 to 4.82]. Therefore, it cannot be definitely stated that the score of the case group was better than that of the control group. Interestingly, HTO with microfracture showed a worse HSS score than that of the control group [3].

Forest plots showing postoperative HSS scores between groups
Radiological results
Radiological results are presented in Table 3. Radiologic results were reported in five studies and they were reported as the mechanical femorotibial (mFTA) or hip–knee–ankle (HKA) angle, and Kellgren–Lawrence (K–L) grade. All five studies reported no significant statistical differences in terms of the mFTA between groups. Mean difference of the mFTA was 0.08° (I 2 0%, 95% CI − 0.26 to 0.43) in the pooled analysis (Fig. 3). One study that evaluated K–L grade reported that a higher progression of arthritis was observed in the HTO with microfracture group [3].

Forest plots showing mFTA (HKA angle) between groups
Arthroscopic, histologic, and MRI findings
Arthroscopic, histologic, and MRI findings are presented in Table 4. In three studies, arthroscopic findings were reported. One study compared the arthroscopic findings of the cartilage healing between HTO only and HTO plus arthroscopic drilling. They reported that no significant differences were observed in the formation of fibrocartilage between groups (p = 0.425) [7]. In two studies (concurrent abrasion arthroplasty and human autologous culture expanded bone marrow mesenchymal cell transplantation), control groups showed more favorable healing than case groups [1, 18]. Control group showed a higher incidence of grade II healing and a lower incidence of grade IV healing in one study, and higher arthroscopic grading in another study. In two studies (concurrent abrasion arthroplasty and human autologous culture expanded bone marrow mesenchymal cell transplantation) that included histologic findings, contradictory results were reported, with no significant difference in the histologic finding and grade of repair reported in one study (concurrent abrasion arthroplasty) and histologic grading of the control group reported as higher in another study (concurrent human autologous culture expanded bone marrow mesenchymal cell transplantation) [1, 18]. In two other studies (concurrent hyaluronic acid and mesenchymal stem cell injection), MRI findings were reported, and both found a more favorable result in the control group in terms of cartilage volume and magnetic resonance observation of cartilage repair tissue score [2, 19].
Discussion
This systematic review and meta-analysis hypothesized that concurrent cartilage procedures would produce little benefit compared with HTO alone, and thus, a concurrent cartilage procedure would not be necessary during HTO. The principal finding of this systematic review and meta-analysis was that concurrent cartilage procedures, in the majority of the studies, produced little effect in terms of the clinical and radiological results following the HTO procedure. However, improved arthroscopic, histologic, and MRI results were reported. Therefore, our hypothesis was partially accepted and partially denied; indicating that further detailed study according to the different concurrent procedures and different outcomes should be performed. However, until now, concurrent procedures have not been considered necessary of the limited benefits in the clinical and radiological results. If we consider the characteristics of patients undergoing HTO, the clinical and radiological outcomes would be considered more important than the arthroscopic, histologic, and MRI findings because most of these patients have osteoarthritis.
Long-term series of HTO have shown a clinical and radiological deterioration over time, although good results at mid-term follow-up have been reported. Therefore, several authors have suggested using cartilage repair procedures such as marrow stimulation procedures, osteochondral graft, and autologous chondrocyte implantation with the aim of improving the long-term outcomes [3, 15, 16]. Kahlenberg et al. [8] reported that HTO with cartilage restoration procedures provides reliable improvement in functional status at least 2-year follow-up in their systematic review. However, they also addressed that analysis of second look outcome was limited by viability in methodology of each study. In the clinical trials, the data of combined procedures are contradictory and there have also been debates on the correlation between cartilage regeneration and clinical results [1, 4, 10, 12]. In our review, concurrent procedures for medial compartment OA showed little benefits in terms of clinical and radiological results. Most articles reported no significant difference regardless of concurrent procedures. In one article, interesting result was reported and concurrent microfracture contrarily showed worse clinical result than HTO alone [3]. In terms of arthroscopic, histological, and MRI findings, concurrent procedures produced a similar or superior result compared with HTO alone, even though there were some controversies.
Injection with hyaluronic acid, platelet rich plasm (PRP), or mesenchymal stem cell are also performed in the hope of relieving pain, improving function, modification cartilage structure, or exerting a chondroprotective effect [2, 9, 19]. Such injections are also used to augment the effect of arthroscopic microfracture, and arthroscopic and immunohistologic improvement have been found [19]. However, until now, their effects are still controversial. In our review, two studies reporting results of injection procedures were included. They showed improved clinical and radiological outcomes but, no differences compared with HTO alone, although there were benefits in terms of MRI findings. Their results were also similar to other arthroscopic or open cartilage procedures. One interesting paper analyzed factors affecting cartilage repair after open-wedge HTO [11]. They reported that cartilage regeneration is affected by body mass index, the difference between the medial femoral condyle and medial tibial condyle, preoperative cartilage degeneration grade, and postoperative limb alignment. This could imply that concurrent procedures for medial compartment OA cannot guarantee successful treatment and superior outcomes.
One remained issue is how to interpret the mismatch between clinical outcome and histologic or MRI outcome. The major feature of osteoarthritis is cartilage erosion, which may lead to eburnation of the underlying subchondral bone. Therefore, main goal of early osteoarthritis treatment is to promote cartilage regeneration [18]. In this respect, improved histologic or MRI findings would indicate success, and therefore, the value of the procedures. However, a problem is that healed cartilage is different from, and the quality is not good as, the original cartilage. Furthermore, success may not lead to a successful clinical or radiological outcome, although this is controversial. Therefore, it is still questionable whether to the improvement in some findings indicate a successful procedure and whether to recommend this kind of procedure. In the future, more technical development in this field may lead to healing with highly qualified cartilage, and then these issues should be reevaluated and the necessity of concurrent procedures revisited.
This study has both strengths and limitations. Our analysis was, to our best knowledge, the first meta-analysis to verify whether concurrent procedures during HTO for medial compartment OA are necessary compared to HTO alone. Regarding the included studies, only comparative studies on concurrent procedures for medial compartment OA were chosen. Therefore, it was possible to come to a qualified conclusion. Limitations of this review should also be noted. First, most studies compared their results using different methods such as clinical, radiological, arthroscopic, histologic, and MRI findings. In addition, different scoring systems were used in the assessment of clinical outcomes. Therefore, it was difficult to perform a pooled analysis. Second, the evaluation periods varied, which could result in bias. Third, it was impossible to analyze efficacy according to the individual procedure because the allocated numbers were too small. Fourth, results of concurrent procedures for medial compartment OA during HTO were only analyzed in this study. Therefore, no results could be obtained for the younger patients with focal cartilage lesions and concomitant varus deformity. Finally, our results do not allow us to draw a definite conclusion regarding which factor is most important for evaluating the effects of concurrent procedures among clinical, radiological, arthroscopic, histologic, and MRI findings.
Conclusion
Our analysis support that concurrent procedures during HTO for medial compartment OA have little beneficial effect regarding clinical and radiological outcomes. However, they might have some beneficial effects in terms of arthroscopic, histologic, and MRI findings even though the quality of healed cartilage is not good as that of original cartilage. Therefore, until now, concurrent procedures for medial compartment OA have been considered optional. Nevertheless, no conclusions can be drawn for younger patients with focal cartilage defects and concomitant varus deformity. This question needs to be addressed separately.
References
Akizuki S, Yasukawa Y, Takizawa T (1997) Does arthroscopic abrasion arthroplasty promote cartilage regeneration in osteoarthritic knees with eburnation? A prospective study of high tibial osteotomy with abrasion arthroplasty versus high tibial osteotomy alone. Arthroscopy 13:9–17
Chareancholvanich K, Pornrattanamaneewong C, Narkbunnam R (2014) Increased cartilage volume after injection of hyaluronic acid in osteoarthritis knee patients who underwent high tibial osteotomy. Knee Surg Sports Traumatol Arthrosc 22:1415–1423
Ferruzzi A, Buda R, Cavallo M, Timoncini A, Natali S, Giannini S (2014) Cartilage repair procedures associated with high tibial osteotomy in varus knees: clinical results at 11 years’ follow-up. Knee 21:445–450
Franceschi F, Longo UG, Ruzzini L, Marinozzi A, Maffulli N, Denaro V (2008) Simultaneous arthroscopic implantation of autologous chondrocytes and high tibial osteotomy for tibial chondral defects in the varus knee. Knee 15:309–313
Harris JD, McNeilan R, Siston RA, Flanigan DC (2013) Survival and clinical outcome of isolated high tibial osteotomy and combined biological knee reconstruction. Knee 20:154–161
Jung WH, Takeuchi R, Chun CW, Lee JS, Ha JH, Kim JH, Jeong JH (2014) Second-look arthroscopic assessment of cartilage regeneration after medial opening-wedge high tibial osteotomy. Arthroscopy 30:72–79
Jung WH, Takeuchi R, Chun CW, Lee JS, Jeong JH (2015) Comparison of results of medial opening-wedge high tibial osteotomy with and without subchondral drilling. Arthroscopy 31:673–679
Kahlenberg CA, Nwachukwu BU, Hamid KS, Steinhaus ME, Williams RJ (2017) Analysis of outcomes for high tibial osteotomies performed with cartilage restoration techniques. Arthroscopy 33:486–492
Koh YG, Kwon OR, Kim YS, Choi YJ (2014) Comparative outcomes of open-wedge high tibial osteotomy with platelet-rich plasma alone or in combination with mesenchymal stem cell treatment: a prospective study. Arthroscopy 30:1453–1460
Koshino T, Wada S, Ara Y, Saito T (2003) Regeneration of degenerated articular cartilage after high tibial valgus osteotomy for medial compartmental osteoarthritis of the knee. Knee 10:229–236
Kumagai K, Akamatsu Y, Kobayashi H, Kusayama Y, Koshino T, Saito T (2016) Factors affecting cartilage repair after medial opening-wedge high tibial osteotomy. Knee Surg Sports Traumatol Arthrosc 25:779–984
Matsunaga D, Akizuki S, Takizawa T, Yamazaki I, Kuraishi J (2007) Repair of articular cartilage and clinical outcome after osteotomy with microfracture or abrasion arthroplasty for medial gonarthrosis. Knee 14:465–471
Moher D, Liberati A, Tetzlaff J, Altman DG (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. J Clin Epidemiol 62:1006–1012
Pascale W, Luraghi S, Perico L, Pascale V (2011) Do microfractures improve high tibial osteotomy outcome? Orthopedics 34:e251–e255
Spahn G, Kirschbaum S, Kahl E (2006) Factors that influence high tibial osteotomy results in patients with medial gonarthritis: a score to predict the results. Osteoarthritis Cartil 14:190–195
Tang WC, Henderson IJP (2005) High tibial osteotomy: long term survival analysis and patients’ perspective. Knee 12:410–413
Wakabayashi S, Akizuki S, Takizawa T, Yasukawa Y (2002) A comparison of the healing potential of fibrillated cartilage versus eburnated bone in osteoarthritic knees after high tibial osteotomy: an arthroscopic study with 1-year follow-up. Arthroscopy 18:272–278
Wakitani S, Imoto K, Yamamoto T, Saito M, Murata N, Yoneda M (2002) Human autologous culture expanded bone marrow mesenchymal cell transplantation for repair of cartilage defects in osteoarthritic knees. Osteoarthritis Cartil 10:199–206
Wong KL, Lee KB, Tai BC, Law P, Lee EH, Hui JH (2013) Injectable cultured bone marrow-derived mesenchymal stem cells in varus knees with cartilage defects undergoing high tibial osteotomy: a prospective, randomized controlled clinical trial with 2 years’ follow-up. Arthroscopy 29:2020–2028
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that we have no conflict of interest.
Funding
This work was supported by Basic Science Research Program through the Ministry of Education of the Republic of Korea and Research Foundation of Korea (NRF) (NRF-2017R1D1A1A9000509).
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Rights and permissions
About this article

Cite this article
Lee, OS., Ahn, S., Ahn, J.H. et al. Effectiveness of concurrent procedures during high tibial osteotomy for medial compartment osteoarthritis: a systematic review and meta-analysis. Arch Orthop Trauma Surg 138, 227–236 (2018). https://doi.org/10.1007/s00402-017-2826-4
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-017-2826-4