
Abstract
Purpose
To investigate the frequency of meniscal tear and the location of tear associated with anterior cruciate ligament (ACL) injury.
Subjects and methods
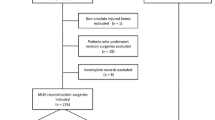
We studied 549 patients (552 knees) who were diagnosed with ACL injury by arthroscopy at our center between January 2006 and March 2014 (8 years and 3 months). The subjects comprised 289 males and 263 females ranging in age from 13 to 66 (mean 26.1) years. The cause of injury was sports-related in 89.1 %, and the mean interval from injury to initial arthroscopy was 23 months. The patients were divided into two groups: arthroscopy performed within 8 weeks after injury (acute group; 256 knees) and more than 8 weeks after injury (chronic group; 296 knees). Frequency of meniscal tear and location of tear were compared between two groups.
Results
The incidence of meniscal tear diagnosed by arthroscopic examination was 79.2 % (437 of 552 knees) in all subjects; 72.7 % (186 of 256 knees) in acute group and 84.8 % (251 of 296 knees) in chronic group, and was significantly higher in chronic group. Regarding the locations of meniscal tears, in acute group (186 knees), medial meniscal tear only was found in 20 knees (10.8 %), lateral meniscal tear only in 129 knees (69.4 %), and bilateral (including medial and lateral) meniscal tears in 37 knees (19.9 %). In chronic group (251 knees), medial meniscal tear only was found in 62 knees (24.7 %), lateral meniscal tear only in 85 knees (33.9 %), and bilateral meniscal tears in 104 knees (41.4 %). Lateral meniscal tear was commonly associated with acute ACL injury, while medial meniscal tear with chronic ACL injury. Bucket handle tear was observed in 25 knees (medial: 17 knees, lateral: 8 knees) in acute group, and 81 knees (medial: 69 knees, lateral: 12 knees) in chronic group, and was more common in the chronic group.
Conclusion
The incidence of meniscal tear associated with ACL injury is higher in chronic cases; the number of medial meniscal tears is particularly high, many of which require meniscectomy. Early ACL reconstruction is recommended also for the prevention of secondary meniscal tear.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Functional instability after anterior cruciate ligament (ACL) injury can be successfully treated with ligament reconstruction. However, the associated meniscus lesions often cannot be repaired and may have long-term detrimental effects on knee function [3]. The reported incidence of meniscal injury varies considerably, ranging from 16 to 82 % in acute ACL injuries and up to 96 % in chronic ACL deficiency [2, 13, 14]. The lateral meniscus is injured more often in acute ACL injuries, and the medial meniscus is more likely involved in chronic ACL deficiency [2, 9].
In the present study, we investigated the frequency of occurrence of meniscal tear associated with ACL injury. We aimed to evaluate the relationship between the time elapsed from ACL injury to arthroscopy and the incidence of meniscal injury detected at the time of arthroscopic surgery for ACL injuries, and to assess the treatment methods for meniscal tears in our patients.
Subjects and methods
We studied 549 patients (552 knees) who were diagnosed definitively with ACL injury based on arthroscopic findings at our center between January 2006 and March 2014 (8 years and 3 months). The subjects comprised 289 males and 263 females with mean age of 26.1 (range 13–66) years. The mean interval from injury to arthroscopic surgery was 726 days (2 days to 32 years). The cause of ACL injury in the subjects was mainly sports-related, accounting for 89.1 % (492 knees). The sporting events in which ACL injury was sustained were basketball in 106 knees (22 %), soccer in 90 knees (18 %), volley ball in 78 knees (16 %), skiing in 41 knees (8 %), rugby in 30 knees (6 %), handball in 23 knees (5 %), judo in 22 knees (4 %), and others in 102 knees (21 %).
The patients were divided into two groups: arthroscopy performed within 8 weeks after injury (acute group; 256 knees, mean age 23.7 years) and more than 8 weeks after injury (chronic group; 296 knees, mean age 28.2 years). We compared the two groups with respect to frequency of meniscal tear, the location of tear, and the treatment method selected. In documenting the location of the tear, we used the classification system described by Cooper et al. [4]. This system divides each meniscus into thirds radially and circumferentially. The radial zones are denoted as A, B, and C (A being the posterior third) for the medial meniscus and D, E, and F (F being the posterior third) for the lateral meniscus. The circumferential zones are divided as follows: 0, the meniscocapsular junction; 1, the outer third; 2, the middle third; and 3, the inner third (Fig. 1).

Meniscal zones of the knee according to Cooper’s classification system [6]. The radial (A–F) and circumferential (0–3) zones of the medial and lateral meniscus
The treatment policy for meniscal tears is to perform meniscal repair for all the lesions that are judged to be suturable, and to perform meniscectomy for the remaining lesions. In principle, medical meniscus was repaired by the inside-out technique and lateral meniscus by the all-inside technique using the Meniscal Viper System [8].
Statistical analysis was performed using StatView 5.0. Chi square test was used for comparisons between groups. A p value less than 0.05 was considered to indicate a significant difference.
Results
A high incidence of meniscal tears was diagnosed at the initial arthroscopy, which was 79 % (437 of 552 knees). The incidence was 72.7 % (186 of 256 knees) in the acute group and 84.8 % (251 of 296 knees) in the chronic group, showing that meniscal tears occurred at a significantly higher rate in the chronic group (Fig. 2).

Rate of meniscal tears in ACL-deficient knees
Regarding the locations of meniscal tears in the acute group, medial meniscal tear only was found in 20 knees (11 %), lateral meniscal tear only in 129 knees (69 %), and bilateral (including medial and lateral) meniscal tears in 37 knees (20 %). In the chronic group, medial meniscal tear only was found in 62 knees (25 %), lateral meniscal tear only in 85 knees (34 %), and bilateral meniscal tears in 104 knees (41 %). These results show that lateral meniscal tears were common in acute ACL injuries, while the rate of medial meniscal tears increased in chronic ACL injuries (Fig. 3).

Distribution of meniscal tears in ACL-deficient knees
When meniscal tear locations were classified according to Cooper (6), the tears in the acute group were frequently located in zones E and F; that is, middle to posterior region of the lateral meniscus. In the chronic group, however, there was an increase of tears in zones A and B; that is, middle to posterior region of the medial meniscus (Fig. 4). When the tear locations were classified by circumferential zones in the acute group, there were few tears in zones 1 and 2 of the medial meniscus, whereas there were relatively large numbers of tears in zones 1 and 2 in the lateral meniscus (Fig. 5).

The radial zone distribution of meniscal tears

The circumferential zone distribution of meniscal tears
Bucket handle tear was observed in a total of 25 knees (lateral: 8 knees, medial: 17 knees) in the acute group, and 81 knees (lateral: 12 knees, medial 69: knees) in the chronic group, with significantly more bucket handle tears in the chronic group (Fig. 6).

Rate of bucket handle tear in ACL-deficient knees
Regarding the choice of treatment methods for the torn menisci, 39 % of the medial meniscal tears were treated by meniscectomy and 40 % by suture in the acute group, while 55 % of the medial meniscal tears were treated by meniscectomy and 35 % by suture in the chronic group (p = 0.0288). For the lateral meniscal tears, 44 % of the tears were treated by meniscectomy and 36 % by suture in the acute group, while 46 % were treated by meniscectomy and 34 % by suture in the chronic group. There were no differences in treatment method between the acute and chronic groups (Fig. 7).

Treatment of meniscal tears
Discussion
Previous American studies of adolescent patients with ACL tears showed an association between a delay in surgical reconstruction (>5 months from initial injury) and an increase in medial meniscus tears [5, 10, 11]. Guenther et al. [7] confirmed an increased likelihood of medial meniscal tears when surgery was performed more than 1 year after injury, but no change in lateral meniscal tears with time. Similar findings have been reported by Millett et al. [11] using a cutoff time to treatment of 6 weeks after ACL tear, by Lawrence et al. [10] using 12 weeks, and by Dumont et al. [5] using 5 months. The increase in medial meniscal tears with time is primarily attributed to the development of new displaced bucket handle meniscal tears. In the present study using a cutoff time from injury to arthroscopy of 8 weeks, the incidence of meniscal tear was significantly higher in the chronic group (84.8 %) than in the acute group (72.7 %). Acute ACL injury was associated with more lateral meniscal tears, while chronic ACL deficiency was associated with more medial meniscal tears. In addition, the number of bucket handle tears was greater in the chronic group (lateral meniscal tear in 12 knees and medial in 69 knees, total 81 knees) than in the acute group (lateral meniscal tear in 8 knees and medial in 17 knees, total 25 knees). Guenther et al. [7] investigated 112 adolescents with ACL ruptures, and reported that medial meniscal tears, especially bucket handle tears, increased steadily in frequency more than 1 year after ACL injury.
In a systematic review, Noyes and Barber-Westin [12] analyzed 19,531 patients and reported that 63 % of medial compartment tears were treated by meniscectomy, 27 % were treated by repair, and 9 % were left in situ. For lateral compartment tears, 71 % were treated by meniscectomy, 14 % were treated by repair, and 14 % were left in situ. Thus, meniscectomy was performed 2–3 times more frequently than meniscus repair during ACL reconstruction. They concluded that this finding is concerning because studies have shown that regardless of knee stability obtained after ACL reconstruction, meniscectomy accelerates degenerative joint changes. In our study, 39 % of medial meniscal tears were treated by meniscectomy and 40 % by suture in the acute group, while 55 % were treated by meniscectomy and 35 % by suture in the chronic group. For lateral meniscal tears, 44 % were treated by meniscectomy and 36 % by suture in the acute group, while 46 % were treated by meniscectomy and 34 % by suture in the chronic group. Compared to the report of Noyes and Barber-Westin [12], our suture rate was high, especially for lateral meniscal tears. The reason is that we use the Meniscal Viper System [8] for suturing tears located in the middle to posterior zone of the lateral meniscus, which are associated with ACL injury at a high rate.
Chhadia et al. [3] studied 1252 patients with ACL injury and found a strong association of prolonged time to surgery with increased risk of medial meniscus injury and decreased repair rate. Thus, it is important to perform surgery within 12 months after injury; otherwise the opportunity of meniscus repair will decrease after this time. Ghodadra et al. [6] studied the articular and meniscal pathology associated with primary ACL reconstruction in 709 patients and concluded that delayed reconstruction may be associated with more serious pathology. Furthermore, in the study of Anderson and Anderson [1] on 130 (135 knees) who received ACL reconstruction younger than 17 years of age, delayed ACL reconstruction increased the risks of secondary meniscal and chondral injuries. Dumont et al. [5] reported that pediatric patients treated more than 150 days after injury for ACL tears had a higher rate of medial meniscal tears than those treated 150 days or less after injury, and demonstrated that increased age and weight are independently associated with a higher rate of medial meniscal tear. Guenther et al. [7] proposed that timely ACL reconstruction may be warranted to reduce the risk of further medial meniscal damage even in the patients who sustained the original injury more than 1 year before.
In the present study also, the incidence of meniscal tear associated with ACL injury was higher in patients with chronic than in those with acute ACL deficiency. In particular, there was an increase in medial meniscal tears, most of which were treated by meniscectomy. From previous reports and the present findings, early ACL reconstruction is necessary also for the prevention of secondary meniscal tear.
References
Anderson AF, Anderson CN (2015) Correlation of meniscal and articular cartilage injuries in children and adolescents with timing of anterior cruciate ligament reconstruction. Am J Sports Med 43(2):275–281
Bellabarba C, Bush-Joseph CA, Bach BR Jr (1997) Patterns of meniscal injury in the anterior cruciate-deficient knee: a review of the literature. Am J Orthop (Belle Mead NJ) 26(1):18–23
Chhadia AM, Inacio MC, Maletis GB, Csintalan RP, Davis BR, Funahashi TT (2011) Are meniscus and cartilage injuries related to time to anterior cruciate ligament reconstruction? Am J Sports Med 39(9):1894–1899
Cooper DE, Arnoczky SP, Warren RF (1990) Arthroscopic meniscal repair. Clin Sports Med 9(3):589–607
Dumont GD, Hogue GD, Padalecki JR, Okoro N, Wilson PL (2012) Meniscal and chondral injuries associated with pediatric anterior cruciate ligament tears: relationship of treatment time and patient-specific factors. Am J Sports Med 40(9):2128–2133
Ghodadra N, Mall NA, Karas V et al (2013) Articular and meniscal pathology associated with primary anterior cruciate ligament reconstruction. J Knee Surg 26(3):185–193
Guenther ZD, Swami V, Dhillon SS, Jaremko JL (2014) Meniscal injury after adolescent anterior cruciate ligament injury: how long are patients at risk? Clin Orthop Relat Res 472(3):990–997
Hagino T, Ochiai S, Watanabe Y et al (2014) Clinical results of arthroscopic all-inside lateral meniscal repair using the Meniscal Viper Repair System. Eur J Orthop Surg Traumatol 24(1):99–104
Kilcoyne KG, Dickens JF, Haniuk E, Cameron KL, Owens BD (2012) Epidemiology of meniscal injury associated with ACL tears in young athletes. Orthopedics 35(3):208–212
Lawrence JT, Argawal N, Ganley TJ (2011) Degeneration of the knee joint in skeletally immature patients with a diagnosis of an anterior cruciate ligament tear: is there harm in delay of treatment? Am J Sports Med 39(12):2582–2587
Millett PJ, Willis AA, Warren RF (2002) Associated injuries in pediatric and adolescent anterior cruciate ligament tears: does a delay in treatment increase the risk of meniscal tear? Arthroscopy 18(9):955–959
Noyes FR, Barber-Westin SD (2012) Treatment of meniscus tears during anterior cruciate ligament reconstruction. Arthroscopy 28(1):123–130
Shoemaker SC, Markolf KL (1986) The role of the meniscus in the anterior-posterior stability of the loaded anterior cruciate-deficient knee. Effects of partial versus total excision. J Bone Joint Surg Am 68(1):71–79
Warren RF, Levy IM (1983) Meniscal lesions associated with anterior cruciate ligament injury. Clin Orthop Relat Res 172:32–37
Acknowledgments
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None.
Rights and permissions
About this article

Cite this article
Hagino, T., Ochiai, S., Senga, S. et al. Meniscal tears associated with anterior cruciate ligament injury. Arch Orthop Trauma Surg 135, 1701–1706 (2015). https://doi.org/10.1007/s00402-015-2309-4
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-015-2309-4