
Abstract
Purpose
To examine the associations between infants’ dietary nutrient trajectories and subsequent neurodevelopment during childhood in the Growing Up in Singapore Towards healthy Outcomes study.
Methods
One-day food records were collected at ages 6, 9 and 12 months, whilst Bayley Scales of Infant and Toddler Development-III and Kaufman Brief Intelligence Test-2 were conducted at ages 24 and 54 months respectively. Nutrient trajectories were constructed using multi-level mixed modelling and associations with neurodevelopment (24 months: n = 484; 54 months: n = 444) were examined using adjusted multivariable linear regression.
Results
At age 24 months, higher protein intake (at 6 months) and increasing rate of intake (from 6 to 12 months) were associated with higher fine motor score [β = 0.17 SD (95% CI 0.03, 0.31) and 0.62 SD (0.10, 1.14) respectively]. Higher fat intake was associated with higher receptive language score [0.04 SD (0.003, 0.07)], but increasing rate of intake was associated with lower expressive language [− 0.20 SD (− 0.39, − 0.01)] and fine motor [− 0.29 SD (− 0.48, − 0.10)] scores. Higher carbohydrate intake was associated with lower gross motor score [− 0.07 SD (− 0.14, − 0.005)], but increasing rate of intake was associated with higher receptive language [0.44 SD (0.08, 0.81)] and fine motor [0.56 SD (0.18, 0.93)] scores. Increasing rate of dietary fibre intake was associated with higher fine motor scores [0.63 SD (0.16, 1.10)]. No significant associations were observed with neurodevelopment at 54 months.
Conclusion
Our findings provide greater understanding of how nutrition over time could have varying effects on child neurodevelopment.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The process of neurodevelopment is described as the interplay between the brain, environment and genes through which cognitive, motor, sensory, socioemotional, cultural and behavioural adaptive functions evolve over time [1]. One critical developmental period is the first 1000 days of life, from conception until age 2 years, when brain growth is rapid and plastic. This renders the brain vulnerable and highly sensitive to influences from environmental factors such as nutrition [2,3,4].
The importance of infant nutrition during the postnatal stage on neurodevelopment has been well documented in literature, with much focus placed on the quality of fats i.e. long-chain polyunsaturated fatty acids (LCPUFA), B vitamins, such as B12, folic acid and choline, and key minerals like zinc, iron and iodine [5, 6]. In fact, many benefits of breastfeeding on neurodevelopment have been attributed to these nutrients as well [7, 8]. Breastfeeding and its (longer) duration have been positively associated with improved cognitive, motor and language development and have potential protective effect against language impairment in infants [9,10,11]. However, as the infant grows and transits from breastmilk to solid foods, nutrients from complementary feeding do continue to build and maintain neurodevelopment [12, 13].
The nutrient composition of complementary diets during infancy in relation to neurodevelopment has not been extensively studied [14, 15]. Our knowledge on the importance of dietary nutrients during infancy comes mostly from supplementation trials, which have generally been conducted in developing countries, where rates of malnourishment are relatively high [16,17,18,19]. Historically, studies have observed positive associations between protein intake and cognitive performance in toddlers from developing countries [20, 21], whilst intervention studies demonstrated that energy and protein supplementation of undernourished infants (age 6–24 months) were associated with improved cognitive and motor development at childhood [22,23,24]. More recently, amino acid supplementation in very low birth weight neonates showed positive correlations with better language and motor scores at age 2 years [25]. There is, however, limited literature examining the relationship between energy, energy yielding macronutrients including carbohydrate, fat and protein, dietary fibre and neurodevelopment in healthy infants living in developed countries [14].
Similarly, whilst most studies have evaluated diets at discrete time points, to our knowledge, there are no studies examining dietary nutrients trajectories in relation to neurodevelopment in young children. Examining individual nutrients longitudinally, via nutrient trajectories, could reveal the cumulative effect of nutrient intakes and expand our understanding of the association between long-term nutrient intakes and neurodevelopment. Additionally, trajectories allow researchers to estimate changes in an individual and how each individual compares to the population mean over time [26].
This paper aims to bridge existing gaps by examining infants’ dietary nutrient trajectories from age 6 to 12 months and their associations with neurodevelopment at ages 24 and 54 months.
Methods
Study population
Data collected was part of the Growing Up in Singapore Towards healthy Outcomes (GUSTO) study, a prospective mother–offspring cohort that has been previously described in detail [27]. Briefly, 1247 pregnant women in their first trimester, aged 18–50 years old, were recruited from KK Women’s and Children’s Hospital (KKH) and National University Hospital (NUH) between June 2009 and September 2010. Participants were either Singapore citizens or permanent residents, of Chinese, Malay or Indian ethnicity with homogenous parental ethnic background, planned to reside in Singapore for the next 5 years and were willing to donate placenta, cord and cord blood at delivery. Excluded from the study were women on chemotherapy, psychotropic drugs or those with serious health conditions such as type 1 diabetes mellitus. The GUSTO study was approved by the Institutional Review Board of KKH and NUH, and written informed consent was obtained from all participants at each study visit.
Infant dietary assessment
Prior to the mother–infant postnatal visits at 6, 9 and 12 months, mothers were given a 3-day food diary to record their infant’s dietary intakes at each time point. The food diaries were collected during the visits and mothers who were unable to complete the food diaries were interviewed by trained clinical staff, with the use of the 5-stage multiple-pass interviewing technique, to recall their infant’s food intake in the past 24 h [28]. Mothers were also shown food pictures with standardised portion sizes and household measuring utensils to facilitate the 24-h food recall interview. For milk intakes, reported volumes of formula milk or expressed breastmilk consumed by infants were directly obtained from the food diaries or 24-h food recalls. For infants who were breastfed, volumes of breastmilk consumption were estimated using methods described by Ponza et al. [29]. Infants who were fed directly with breastmilk (latched-on) were estimated to have consumed 780 ml/day of breastmilk at age 6 months and 600 ml/day at ages 9 and 12 months. If infants took a mixture of breastmilk and infant formula (partial breastfeeding), the amount of infant formula consumption was deducted from these volumes and the remaining amounts estimated as breastmilk consumption. Nutrient compositions of breastmilk at the respective age groups were derived from existing literature that employed laboratory techniques to analyse the levels of macro- and micro-nutrients in breastmilk [30].
Data from either the 24-h food recalls or 1 randomly selected day from the food diaries were used for dietary nutrient analyses to maximise the sample size. Our previous study has established a moderate to strong correlation (r = 0.43–0.82) between the 1-day record and the two other days using a subset of infants with complete 3-day food diaries (n = 163) [31]. Nutrient analyses were performed using Dietplan 7 (Forestfield Software Ltd), a nutrient analysis software that includes a database of our local foods compositions. Energy and nutrient intakes values were tabulated and examined broadly without further classification of types and quality; protein, total fat and carbohydrate (available carbohydrates including sugars and starch [32]) were expressed as percentage contribution to total energy, whilst dietary fibre (non-digestible polysaccharides including lignin and resistant starch [32]) was expressed as grammes per 1000 kcal. Further details of dietary nutrient analysis were elaborated in Lim et al. [33]. Additionally from this study, it was observed that the energy and nutrient intakes of GUSTO infants at age 6, 9 and 12 months met Institute of Medicine (IOM) guidelines [33] (Online Resource 1).
Infant nutrient trajectories
Infant energy and nutrient trajectories were constructed using multi-level mixed models with level-1 (age at 6, 9 and 12 months) and level-2 (individual infant) random effects. This accounts for repeated measures of infant dietary intakes, allowing variations in individual trajectories such that each infant has his/her own intercept and slope. Multi-level mixed modelling also allows for missing time points in data, with the assumption that the data is missing at random. The current estimates for intercept reflect the nutrient intake difference of each infant compared to the population mean at age 6 months, whilst estimates for slope represent the difference in the rate of change of each nutrient intake as compared to the population mean from age 6 to 12 months. These estimates were used as predictor variables in the subsequent analyses.
Child neurodevelopment assessments
At ages 24 (± 1 month) and 54 months (+ 2 months), a subset of the children underwent neurodevelopment assessments conducted by trained staff. The Bayley Scales of Infant and Toddler Development, 3rd Edition (BSID-III) and Kaufman Brief Intelligence Test, 2nd Edition (KBIT-2) were part of the questionnaires administered at ages 24 and 54 months respectively. BSID-III is a standardised test that evaluates children aged 1–42 months across 5 domains: cognition, expressive language, receptive language, fine motor and gross motor [34]. KBIT-2 can be used from 4 to 90 years old and consists of 2 domains: verbal and non-verbal IQ subtests. The verbal subtests measure verbal skills, concept formation and reasoning, whilst non-verbal subtests measure problem-solving abilities. Items are free of cultural and gender bias [35]. Further methodological details of the neurodevelopment assessments conducted in GUSTO have been described in Lai et al. [36].
Covariates
Potential confounding variables were selected based on previous literature [10, 37,38,39]. Maternal age, ethnicity, and education were collected during recruitment whilst breastfeeding duration was determined from infant feeding questionnaires administered at 3 weeks, and at 3, 6, 9 and 12 months postpartum. Breastfeeding duration was subsequently categorised into 3 groups—any breastfeeding for less than 6 months, any breastfeeding for 6 to less than 12 months and any breastfeeding for 12 months or more. Infant gestational age, reported in completed weeks, was determined by ultrasonography during the first trimester by trained ultra-sonographers and information on sex and birth weight was obtained from delivery records. Gestational age and sex adjusted birth weight z-scores and subsequent percentile classification were derived based on methods from Mikolajczyk et al. [40].
Statistical analysis
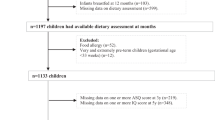
Using the available dietary records at age 6 months (n = 748), 9 months (n = 881) and 12 months (n = 899), 1035 nutrient trajectories were generated. Of 1035 infants, 484 completed BSID-III and 444 completed KBIT-2 at ages 24 and 54 months, respectively. Due to the unavailability of age-specific norms for our population and to facilitate comparison between the neurodevelopment assessments, raw scores of BSID-III and KBIT-2 domains were converted to standard deviation (SD) scores. Independent sample t-test and One-way Analysis of Variance (ANOVA) with Bonferroni post hoc analyses were used to assess differences in BSID-III and KBIT-2 domains SD scores across various maternal socio-demographic characteristics and infant characteristics. Multivariable linear regression analyses were performed to study the associations between infant nutrient trajectories and neurodevelopment assessments. Models were adjusted for potential confounders—maternal age, ethnicity, maternal education, infant’s exact age at neurodevelopment testing, gestational age, sex, birth weight z-scores and duration of breastfeeding. Models examining slopes were further adjusted for intercepts. Beta coefficients in intercept models are reflective of change in neurodevelopment outcome SD score per 1-unit higher nutrient intake than the population mean at age 6 months, whilst beta coefficients in slope models are reflective of change in neurodevelopment outcome SD score per 1-unit increase in rate of nutrient intake greater than the population mean from age 6 to 12 months. Missing covariate data [Education (n = 2); Breastfeeding Duration (n = 9)] were estimated by multiple imputation techniques with chained equations (20 times) and pooled analyses were presented. Further sensitivity analysis was done to examine associations amongst children who completed both BSID-III and KBIT-2 (n = 373). All statistical analyses were performed using Stata version 17 (StataCorp LLC, TX, USA). A 2-tailed p-value of < 0.05 was considered to be statistically significant.
Results
Study population characteristics
Maternal and infant characteristics in association with BSID-III and KBIT-2 domains SD scores are presented in Tables 1 and 2.
Mothers who had university or higher education had infants with significantly higher BSID-III scores across cognition, language and fine motor domains at age 24 months. Mothers who breastfed for 12 months or more also had infants with significantly higher cognition and language scores. Older mothers tended to have infants with higher receptive language score. Infants born to Chinese mothers had significantly higher receptive language score, whilst infants born to Malay mothers had higher gross motor score at age 24 months. With the exception of gross motor domain, female infants had higher scores across all other BSID-III domains than males at age 24 months.
Similar trends were observed for KBIT-2 domains, where mothers who had university or higher education and breastfed for 12 months or more had infants with significantly higher verbal and non-verbal scores at age 54 months. Infants born to Chinese mothers also had significantly higher verbal and non-verbal scores. No other significant characteristics differences were observed for KBIT-2 domains.
Associations of infant nutrient trajectories with BSID-III domains SD scores at age 24 months
The adjusted associations of infant energy and nutrient trajectories at age 6 to 12 months with BSID-III domains SD scores at age 24 months are shown in Table 3.
At age 6 months (intercept), higher total fat intake was associated with higher receptive language score [β = 0.04 SD (95% CI 0.003, 0.07)], whilst higher protein intake was associated with higher fine motor score [0.17 SD (0.03, 0.31)] and higher carbohydrate intake was associated with lower gross motor score [− 0.07 SD (− 0.14, − 0.005)]. No associations were observed for energy and fibre intakes at age 6 months with BSID-III domains at age 24 months.
From age 6 to 12 months (slope), increasing rate of carbohydrate intake was associated with higher receptive language [0.44 SD (0.08, 0.81)] and fine motor [0.56 SD (0.18, 0.93)] scores. Increasing protein and fibre intakes were also associated with higher fine motor score [0.62 SD (0.10, 1.14) and 0.63 SD (0.16, 1.10) respectively]. Conversely, increasing total fat intake was associated with lower expressive language [− 0.20 SD (− 0.39, − 0.01)] and fine motor scores [− 0.29 SD (− 0.48, − 0.10)]. No associations were observed for nutrient intakes from age 6 to 12 months with cognition and gross motor scores at age 24 months.
Similar trends were observed from the sensitivity analysis. However, the association between increasing rate of carbohydrate intake from age 6 to 12 months with higher receptive language score at age 24 months was lost. (Online Resource 2).
Associations of infant nutrient trajectories with KBIT-2 domains SD scores at age 54 months
The adjusted associations of infant energy and nutrient trajectories at age 6 to 12 months with KBIT-2 domains SD scores at age 54 months are shown in Table 4. For both intercepts (age 6 months) and slopes (age 6 to 12 months), no significant associations between nutrient trajectories and KBIT-2 scores at age 54 months were observed.
However, from the sensitivity analysis, there were associations observed between total energy intake and verbal score. At age 6 months, higher energy intake was associated with higher verbal score [β = − 0.003 SD (95% CI − 0.01, − 0.0005)] at age 54 months. In contrast, increasing rate of energy intake from age 6 to 12 months was associated with lower verbal score [− 0.01 SD (− 0.02, − 0.002)] at age 54 months. (Online Resource 3).
Discussion
In the present study, we found that protein, total fat and carbohydrate intake trajectories from 6 to 12 months of infancy had significant but opposing associations with childhood language and motor development, whilst dietary fibre intake trajectory was positively associated with fine motor development at age 24 months. However, total energy trajectory showed no significant associations with neurodevelopment outcomes. Additionally, no associations were found between nutrient trajectories and neurodevelopment outcomes at 54 months of age.
Positive associations were observed between higher protein intake at age 6 months and across 6 to 12 months with higher fine motor score at age 24 months. Protein is essential for brain development and regions associated with fine motor development—cortex and cerebellum [41], are vulnerable to protein inadequacy [42]. Much of the literature focussed on protein supplementation in preterm, low birthweight or malnourished infants and results on fine motor scores were mixed [43,44,45]. Even though findings from literature may not be directly comparable to our study sample of healthy infants, protein remains to be an important nutrient for brain development and findings from our study suggest possible influence on motor development.
Higher fat intake at age 6 months was positively associated with receptive language development at age 24 months. This is in line with literature, where dietary fats, in particular fatty acids, have been reported to play a crucial role in neurodevelopment [5]. It is also possible that our findings were in part contributed by breastmilk consumption, as a substantial proportion of our study population (43%) were breastfed for 6 months or more. However, when considering the rate of change in fat intake from age 6 to 12 months, increased rate of fat intake greater than the population mean was negatively associated with expressive language and fine motor development at age 24 months. This suggests that whilst fat intake may be important for language and motor development during infancy, a greater increase in fat intakes over time (from age 6 to 12 months) could attenuate its beneficial effects at age 24 months. It is recommended that dietary fats contribute 40–60% of total energy in the first 6 months of life and gradually reduce to 30–35% up to 3 years of age [46]. Consistent higher intakes of fat during the first year of life could be a reflection of poor diet, which in turn is associated with poor childhood cognitive development [47].
To the best of our knowledge, no previous study has examined the influence of carbohydrate intake during infancy on neurodevelopment in childhood. We observed that higher carbohydrate intake at age 6 months was associated with lower gross motor scores at age 24 months. This inverse association may be due to the higher percentage of carbohydrate contribution to energy at the expense of lower fat contribution. Interestingly, our study also observed that an increased rate of carbohydrate intake from 6 to 12 months was positively associated with better receptive language and fine motor development at age 24 months. Whilst the current evidence in this area remain equivocal [48], findings from our study suggests that sustained carbohydrate intake could benefit neurodevelopment. As carbohydrate, in the form of glucose, is the main energy source that the brain uses for neurodevelopment [49], it is essential for developing infants to consume sufficient carbohydrates, to maintain the brain’s development and processes [50]. We were not able to examine the type and quality of carbohydrates consumed in our current study and future research should consider exploring this to ascertain the influence of carbohydrates on neurodevelopment. Additionally, long-term intake of carbohydrate has been linked to gut microbiota composition [51], and several studies have observed associations between gut microbiota composition and neurodevelopment in infants [5, 52, 53]. Further research is needed to elucidate the mechanism underpinning carbohydrate intake–gut microbiota interactions and neurodevelopment.
Dietary fibre intake from age 6 to 12 months also exhibited positive associations with fine motor skills at age 24 months. A cross-sectional study in pre-pubertal children aged 7 to 9 years old showed that children with greater dietary fibre intake performed better at tasks needing different levels of cognitive control [54]. Although this study was conducted in older children, it is possible that the association of dietary fibre with child neurodevelopment could have occurred earlier in life. A study examining maternal diet high in dietary fibre and protein was shown to be associated with lower risk of non-competency in cognitive and gross motor development in 1-year old infants [55]. Khan et al. suggested that dietary fibre could affect neurocognitive development via immunomodulation or gut microbiota–brain interactions, where bacterial fermentation of dietary fibre produces short-chain fatty acids that could reduce pro-inflammatory cytokines and support neuronal survival and growth [54].
It is well recognised that brain growth occurs rapidly during the first two years of life and is especially sensitive around age one year, due to developments associated with frontal lobe maturation [56, 57]. From our study, the observed associations of dietary nutrient trajectories in the first year of life with neurodevelopment suggest that it may be possible to improve neurodevelopment outcomes of young children through changing infant diet, with a focus on balancing protein, total fats and carbohydrate intakes. The construction of dietary nutrient trajectories enabled us to maximise the potential of repeated measures in a longitudinal cohort study, taking into account changes in intake over time as the infant grows progressively from consuming baby foods to table foods. In addition, presence of intercepts and slopes allowed us to observe how dietary intakes could potentially affect neurodevelopment cross-sectionally (intercept) and over time (slope). Though it is not possible to determine specific causality of the associations due to influence from factors, such as genetics and the environment, we have adjusted for several common and important confounders. However, as with all observational studies, there could be residual confounding that was not be accounted for. The large sampling frame of 484 infants also provided greater power to the regression models, reducing the probability of chance findings. The study sample of healthy infants also allows for greater generalisability of findings to populations in developed countries. Although dietary intakes obtained from single day food records may not accurately represent the infant’s usual diet, in our previous study, we have established strong correlation between single day intake and 2 day intakes from a 3 day food diary, indicating reproducibility of the single day food records [31]. Lastly, whilst breastmilk intakes of infants who were directly breastfed were estimated using established methods, there could still be deviations from the actual amounts and nutrients consumed. However, this should have minimal impact on our findings as majority of the GUSTO infants were predominantly formula fed (63–80%) [33].
Conclusion
In this study on Asian infants, intakes of dietary protein, total fat, carbohydrate and fibre between ages 6 and 12 months showed differing associations with language and motor outcomes at age 24 months. Cross-sectionally at age 6 months, higher protein and total fat intake, but not carbohydrate intake, was beneficial for language and motor development. However, the opposite was observed when dietary fat and carbohydrate were examined across time from 6 to 12 months, where an increase rate of carbohydrate intake was favourable for language and motor outcomes, whilst fat was not. Separately, increasing rate of dietary fibre intake from 6 to 12 months was beneficial for fine motor development. Trajectory of total energy intake during infancy had no significant associations with childhood neurodevelopment outcomes. The ability to examine longitudinal dietary intakes of infants and identifying differences in association with neurodevelopment potentially provides a more in-depth understanding of how nutrition over time could have varying effects on child neurodevelopment. Further studies could also consider looking into the quality of macronutrients and how these change over time, which could shed some light on the mechanism underlying the associations between macronutrients and neurodevelopment.
Data availability
The datasets generated and/or analysed during the current study are not publicly available due to an ethical restriction (patient confidentiality) which was imposed by the Centralised Institutional Review Board of SingHealth. Interested researchers may request for the data by contacting the corresponding author.
References
Suchdev PS, Boivin MJ, Forsyth BW, Georgieff MK, Guerrant RL, Nelson CA 3rd (2017) Assessment of neurodevelopment, nutrition, and inflammation from fetal life to adolescence in low-resource settings. Pediatrics 139(Suppl 1):S23–S37. https://doi.org/10.1542/peds.2016-2828E
Krebs NF, Lozoff B, Georgieff MK (2017) Neurodevelopment: the impact of nutrition and inflammation during infancy in low-resource settings. Pediatrics 139(Suppl 1):S50–S58. https://doi.org/10.1542/peds.2016-2828G
Britto PR, Perez-Escamilla R (2013) No second chances? Early critical periods in human development. Soc Sci Med 97:238–240. https://doi.org/10.1016/j.socscimed.2013.09.001
Bryan J, Osendarp S, Hughes D, Calvaresi E, Baghurst K, van Klinken JW (2004) Nutrients for cognitive development in school-aged children. Nutr Rev 62(8):295–306. https://doi.org/10.1111/j.1753-4887.2004.tb00055.x
Cohen Kadosh K, Muhardi L, Parikh P, Basso M, Jan Mohamed HJ, Prawitasari T, Samuel F, Ma G, Geurts JM (2021) Nutritional support of neurodevelopment and cognitive function in infants and young children—an update and novel insights. Nutrients. https://doi.org/10.3390/nu13010199
Nyaradi A, Li J, Hickling S, Foster J, Oddy WH (2013) The role of nutrition in children’s neurocognitive development, from pregnancy through childhood. Front Hum Neurosci 7:97. https://doi.org/10.3389/fnhum.2013.00097
Chiurazzi M, Cozzolino M, Reinelt T, Nguyen TD, Elke Chie S, Natalucci G, Miletta MC (2021) Human milk and brain development in infants. Reprod Med 2(2):107–117. https://doi.org/10.3390/reprodmed2020011
Kamini D, Amrita K, Preeti C-G, Sadhana J (2020) Breast milk components and neurodevelopment of children. Indian J Public Health Res Dev. https://doi.org/10.37506/ijphrd.v11i6.9771
Leventakou V, Roumeliotaki T, Koutra K, Vassilaki M, Mantzouranis E, Bitsios P, Kogevinas M, Chatzi L (2015) Breastfeeding duration and cognitive, language and motor development at 18 months of age: Rhea mother-child cohort in Crete. Greece J Epidemiol Community Health 69(3):232–239. https://doi.org/10.1136/jech-2013-202500
Cai S, Pang WW, Low YL, Sim LW, Sam SC, Bruntraeger MB, Wong EQ, Fok D, Broekman BF, Singh L, Richmond J, Agarwal P, Qiu A, Saw SM, Yap F, Godfrey KM, Gluckman PD, Chong YS, Meaney MJ, Kramer MS, Rifkin-Graboi A, Group GS (2015) Infant feeding effects on early neurocognitive development in Asian children. Am J Clin Nutr 101(2):326–336. https://doi.org/10.3945/ajcn.114.095414
Smith JM (2015) Breastfeeding and language outcomes: a review of the literature. J Commun Disord 57:29–40. https://doi.org/10.1016/j.jcomdis.2015.04.002
Murray R (2020) Starting strong: dietary, behavioral, and environmental factors that promote “strength” from conception to age 2 years. Appl Physiol Nutr Metab 45(10):1066–1070. https://doi.org/10.1139/apnm-2020-0073
Campoy C, Campos D, Cerdo T, Dieguez E, Garcia-Santos JA (2018) Complementary feeding in developed countries: the 3 Ws (when, what, and why?). Ann Nutr Metab 73(Suppl 1):27–36. https://doi.org/10.1159/000490086
Agostoni C, Guz-Mark A, Marderfeld L, Milani GP, Silano M, Shamir R (2019) The long-term effects of dietary nutrient intakes during the first 2 years of life in healthy infants from developed countries: an umbrella review. Adv Nutr 10(3):489–501. https://doi.org/10.1093/advances/nmy106
Fewtrell M, Bronsky J, Campoy C, Domellof M, Embleton N, Fidler Mis N, Hojsak I, Hulst JM, Indrio F, Lapillonne A, Molgaard C (2017) Complementary feeding: a position paper by the European Society for Paediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN) Committee on Nutrition. J Pediatr Gastroenterol Nutr 64(1):119–132. https://doi.org/10.1097/MPG.0000000000001454
Prado EL, Dewey KG (2014) Nutrition and brain development in early life. Nutr Rev 72(4):267–284. https://doi.org/10.1111/nure.12102
Larson LM, Yousafzai AK (2017) A meta-analysis of nutrition interventions on mental development of children under-two in low- and middle-income countries. Matern Child Nutr. https://doi.org/10.1111/mcn.12229
Ip P, Ho FKW, Rao N, Sun J, Young ME, Chow CB, Tso W, Hon KL (2017) Impact of nutritional supplements on cognitive development of children in developing countries: a meta-analysis. Sci Rep 7(1):10611. https://doi.org/10.1038/s41598-017-11023-4
Grantham-McGregor S, Baker-Henningham H (2005) Review of the evidence linking protein and energy to mental development. Public Health Nutr 8(7A):1191–1201. https://doi.org/10.1079/phn2005805
Wachs TD, Moussa W, Bishry Z, Yunis F, Sobhy A, McCabe G, Jerome N, Galal O, Harrison G, Kirksey A (1993) Relations between nutrition and cognitive performance in Egyptian toddlers. Intelligence 17(2):151–172. https://doi.org/10.1016/0160-2896(93)90025-z
Sigman M, McDonald MA, Neumann C, Bwibo N (1991) Prediction of cognitive competence in Kenyan children from toddler nutrition, family characteristics and abilities. J Child Psychol Psychiatry 32(2):307–320. https://doi.org/10.1111/j.1469-7610.1991.tb00309.x
Pollitt E, Gorman KS, Engle PL, Rivera JA, Martorell R (1995) Nutrition in early life and the fulfillment of intellectual potential. J Nutr 125(4 Suppl):1111S-1118S. https://doi.org/10.1093/jn/125.suppl_4.1111S
Pollitt E, Gorman KS, Engle PL, Martorell R, Rivera J (1993) Early supplementary feeding and cognition: effects over two decades. Monogr Soc Res Child Dev 58(7):1–99. https://doi.org/10.1111/j.1540-5834.1993.tb00418.x
Grantham-McGregor SM, Powell CA, Walker SP, Himes JH (1991) Nutritional supplementation, psychosocial stimulation, and mental development of stunted children: the Jamaican Study. Lancet 338(8758):1–5. https://doi.org/10.1016/0140-6736(91)90001-6
Yang J, Chang SS, Poon WB (2016) Relationship between amino acid and energy intake and long-term growth and neurodevelopmental outcomes in very low birth weight infants. JPEN J Parenter Enteral Nutr 40(6):820–826. https://doi.org/10.1177/0148607115572833
McNeish D, Matta T (2018) Differentiating between mixed-effects and latent-curve approaches to growth modeling. Behav Res Methods 50(4):1398–1414. https://doi.org/10.3758/s13428-017-0976-5
Soh SE, Tint MT, Gluckman PD, Godfrey KM, Rifkin-Graboi A, Chan YH, Stunkel W, Holbrook JD, Kwek K, Chong YS, Saw SM, Group GS (2014) Cohort profile: Growing Up in Singapore Towards healthy Outcomes (GUSTO) birth cohort study. Int J Epidemiol 43(5):1401–1409. https://doi.org/10.1093/ije/dyt125
Conway JM, Ingwersen LA, Vinyard BT, Moshfegh AJ (2003) Effectiveness of the US Department of Agriculture 5-step multiple-pass method in assessing food intake in obese and nonobese women. Am J Clin Nutr 77(5):1171–1178. https://doi.org/10.1093/ajcn/77.5.1171
Ponza M, Devaney B, Ziegler P, Reidy K, Squatrito C (2004) Nutrient intakes and food choices of infants and toddlers participating in WIC. J Am Diet Assoc 104(1 Suppl 1):s71-79. https://doi.org/10.1016/j.jada.2003.10.018
Dewey KG, Finley DA, Lönnerdal B (1984) Breast milk volume and composition during late lactation (7–20 months). J Pediatr Gastroenterol Nutr 3(5):713–720. https://doi.org/10.1097/00005176-198411000-00014
Lim GH, Toh JY, Aris IM, Chia AR, Han WM, Saw SM, Godfrey KM, Gluckman PD, Chong YS, Yap F, Lee YS, Kramer MS, Chong MF (2016) Dietary pattern trajectories from 6 to 12 months of age in a multi-ethnic Asian cohort. Nutrients. https://doi.org/10.3390/nu8060365
Charrondiere UR, Chevassus-Agnes S, Marroni S, Burlingame B (2004) Impact of different macronutrient definitions and energy conversion factors on energy supply estimations. J Food Compos Anal 17(3):339–360. https://doi.org/10.1016/j.jfca.2004.03.011
Lim SX, Toh JY, van Lee L, Han WM, Shek LP, Tan KH, Yap F, Godfrey KM, Chong YS, Chong MF (2018) Food sources of energy and macronutrient intakes among infants from 6 to 12 months of age: the Growing Up in Singapore Towards Healthy Outcomes (GUSTO) study. Int J Environ Res Public Health. https://doi.org/10.3390/ijerph15030488
Bayley N (2006) Bayley scales of infant and toddler development, 3rd edn. Harcourt Assessment, San Antonio
Kaufman AS, Kaufman NL (2013) Kaufman brief intelligence test. Encyclopedia of special education, 2nd edn. Wiley, New York. https://doi.org/10.1002/9781118660584.ese1325
Lai JS, Cai S, Lee BL, Godfrey KM, Gluckman PD, Shek LP, Yap F, Tan KH, Chong YS, Ong CN, Meaney MJ, Rifkin-Graboi A, Broekman BFP, Chong MFF (2021) Higher maternal plasma beta-cryptoxanthin concentration is associated with better cognitive and motor development in offspring at 2 years of age. Eur J Nutr 60(2):703–714. https://doi.org/10.1007/s00394-020-02277-2
Smithers LG, Golley RK, Mittinty MN, Brazionis L, Northstone K, Emmett P, Lynch JW (2012) Dietary patterns at 6, 15 and 24 months of age are associated with IQ at 8 years of age. Eur J Epidemiol 27(7):525–535. https://doi.org/10.1007/s10654-012-9715-5
Smithers LG, Golley RK, Mittinty MN, Brazionis L, Northstone K, Emmett P, Lynch JW (2013) Do dietary trajectories between infancy and toddlerhood influence IQ in childhood and adolescence? Results from a prospective birth cohort study. PLoS ONE 8(3):e58904. https://doi.org/10.1371/journal.pone.0058904
Pang WW, Tan PT, Cai S, Fok D, Chua MC, Lim SB, Shek LP, Chan SY, Tan KH, Yap F, Gluckman PD, Godfrey KM, Meaney MJ, Broekman BFP, Kramer MS, Chong YS, Rifkin-Graboi A (2020) Nutrients or nursing? Understanding how breast milk feeding affects child cognition. Eur J Nutr 59(2):609–619. https://doi.org/10.1007/s00394-019-01929-2
Mikolajczyk RT, Zhang J, Betran AP, Souza JP, Mori R, Gulmezoglu AM, Merialdi M (2011) A global reference for fetal-weight and birthweight percentiles. Lancet 377(9780):1855–1861. https://doi.org/10.1016/S0140-6736(11)60364-4
Burr P, Choudhury P (2022) Fine motor disability. StatPearls Publishing, Treasure Island
Cormack BE, Harding JE, Miller SP, Bloomfield FH (2019) The influence of early nutrition on brain growth and neurodevelopment in extremely preterm babies: a narrative review. Nutrients 11(9):2029. https://doi.org/10.3390/nu11092029
Hortensius LM, Janson E, van Beek PE, Groenendaal F, Claessens NHP, Swanenburg de Veye HFN, Eijsermans MJC, Koopman-Esseboom C, Dudink J, van Elburg RM, Benders MJNL, Tataranno ML, van der Aa NE (2021) Nutritional intake, white matter integrity, and neurodevelopment in extremely preterm born infants. Nutrients 13(10):3409. https://doi.org/10.3390/nu13103409
Kashaki M, Samghabadi FM, Bordbar A (2019) Effect of fortification of breast milk in conjugation with protein supplement on neurodevelopment of preterm low birth weight infants at 3 years. Med Arch 73(5):344–350. https://doi.org/10.5455/medarh.2019.73.344-350
Olsen MF, Iuel-Brockdorff A-S, Yaméogo CW, Cichon B, Fabiansen C, Filteau S, Phelan K, Ouédraogo A, Michaelsen KF, Gladstone M, Ashorn P, Briend A, Ritz C, Friis H, Christensen VB (2020) Impact of food supplements on early child development in children with moderate acute malnutrition: a randomised 2 x 2 x 3 factorial trial in Burkina Faso. PLoS Med 17(12):e1003442. https://doi.org/10.1371/journal.pmed.1003442
Uauy R, Dangour AD (2009) Fat and fatty acid requirements and recommendations for infants of 0–2 years and children of 2–18 years. Ann Nutr Metab 55(1–3):76–96. https://doi.org/10.1159/000228997
Tandon PS, Tovar A, Jayasuriya AT, Welker E, Schober DJ, Copeland K, Dev DA, Murriel AL, Amso D, Ward DS (2016) The relationship between physical activity and diet and young children’s cognitive development: a systematic review. Prev Med Rep 3:379–390. https://doi.org/10.1016/j.pmedr.2016.04.003
Stephen A, Alles M, de Graaf C, Fleith M, Hadjilucas E, Isaacs E, Maffeis C, Zeinstra G, Matthys C, Gil A (2012) The role and requirements of digestible dietary carbohydrates in infants and toddlers. Eur J Clin Nutr 66(7):765–779. https://doi.org/10.1038/ejcn.2012.27
Hay WW Jr, Brown LD, Denne SC (2014) Energy requirements, protein-energy metabolism and balance, and carbohydrates in preterm infants. World Rev Nutr Diet 110:64–81. https://doi.org/10.1159/000358459
Hardy K, Brand-Miller J, Brown KD, Thomas MG, Copeland L (2015) The importance of dietary carbohydrate in human evolution. Q Rev Biol 90(3):251–268. https://doi.org/10.1086/682587
Oluwagbemigun K, O’Donovan AN, Berding K, Lyons K, Alexy U, Schmid M, Clarke G, Stanton C, Cryan J, Nothlings U (2021) Long-term dietary intake from infancy to late adolescence is associated with gut microbiota composition in young adulthood. Am J Clin Nutr 113(3):647–656. https://doi.org/10.1093/ajcn/nqaa340
Tamana SK, Tun HM, Konya T, Chari RS, Field CJ, Guttman DS, Becker AB, Moraes TJ, Turvey SE, Subbarao P, Sears MR, Pei J, Scott JA, Mandhane PJ, Kozyrskyj AL (2021) Bacteroides-dominant gut microbiome of late infancy is associated with enhanced neurodevelopment. Gut Microbes 13(1):1–17. https://doi.org/10.1080/19490976.2021.1930875
Carlson AL, Xia K, Azcarate-Peril MA, Goldman BD, Ahn M, Styner MA, Thompson AL, Geng X, Gilmore JH, Knickmeyer RC (2018) Infant gut microbiome associated with cognitive development. Biol Psychiatry 83(2):148–159. https://doi.org/10.1016/j.biopsych.2017.06.021
Khan NA, Raine LB, Drollette ES, Scudder MR, Kramer AF, Hillman CH (2015) Dietary fiber is positively associated with cognitive control among prepubertal children. J Nutr 145(1):143–149. https://doi.org/10.3945/jn.114.198457
Lv S, Qin R, Jiang Y, Lv H, Lu Q, Tao S, Huang L, Liu C, Xu X, Wang Q, Li M, Li Z, Ding Y, Song C, Jiang T, Ma H, Jin G, Xia Y, Wang Z, Geng S, Du J, Lin Y, Hu Z (2022) Association of maternal dietary patterns during gestation and offspring neurodevelopment. Nutrients 14(4):730. https://doi.org/10.3390/nu14040730
Nyaradi A, Li J, Foster JK, Hickling S, Jacques A, O’Sullivan TA, Oddy WH (2016) Good-quality diet in the early years may have a positive effect on academic achievement. Acta Paediatr 105(5):e209–e218. https://doi.org/10.1111/apa.13324
Chugani HT (1998) A critical period of brain development: studies of cerebral glucose utilization with PET. Prev Med 27(2):184–188. https://doi.org/10.1006/pmed.1998.0274
Acknowledgements
We would like to thank the participants for their contributions to this study. We would also like to thank and acknowledge the GUSTO study group. The GUSTO study group includes Allan Sheppard, Amutha Chinnadurai, Anne Eng Neo Goh, Anne Rifkin-Graboi, Anqi Qiu, Arijit Biswas, Bee Wah Lee, Birit Froukje Philipp Broekman, Boon Long Quah, Chai Kiat Chng, Cheryl Shufen Ngo, Choon Looi Bong, Christiani Jeyakumar Henry, Daniel Yam Thiam Goh, Doris Ngiuk Lan Loh, Fabian Kok Peng Yap, George Seow Heong Yeo, Helen Yu Chen, Hugo P. S. van Bever, Iliana Magiati, Inez Bik Yun Wong, Ivy Yee-Man Lau, Jeevesh Kapur, Jenny L. Richmond, Jerry Kok Yen Chan, Joanna Dawn Holbrook, Joshua J. Gooley, Keith M. Godfrey, Kenneth Yung Chiang Kwek, Kok Hian Tan, Krishnamoorthy Naiduvaje, Leher Singh, Lin Su, Lourdes Mary Daniel, Lynette Pei-Chi Shek, Marielle V. Fortier, Mark Hanson, Mary Foong-Fong Chong, Mary Rauff, Mei Chien Chua, Michael J. Meaney, Mya Thway Tint, Neerja Karnani, Ngee Lek, Oon Hoe Teoh, P. C. Wong, Peter David Gluckman, Pratibha Keshav Agarwal, Rob Martinus van Dam, Salome A. Rebello, Seang Mei Saw, Shang Chee Chong, Shirong Cai, Shu-E Soh, Sok Bee Lim, Stephen Chin-Ying Hsu, Victor Samuel Rajadurai, Walter Stunkel, Wee Meng Han, Wei Pang, Yap Seng Chong, Yin Bun Cheung, Yiong Huak Chan and Yung Seng Lee.
Funding
The GUSTO cohort study was funded by the Singapore National Research Foundation’s Translational and Clinical Research (TCR) Flagship Programme and was administered by the Singapore Ministry of Health’s National Medical Research Council (NMRC), Singapore—NMRC/TCR/004-NUS/2008; NMRC/TCR/012-NUHS/2014. Additional funding was given by the Singapore Institute for Clinical Sciences, Agency for Science Technology and Research (A*STAR), Singapore. KMG is supported by the UK Medical Research Council (MC_UU_12011/4), the National Institute for Health Research (NIHR Senior Investigator NF-SI-0515-10042), NIHR Southampton 1000DaysPlus Global Nutrition Research Group (17/63/154) and NIHR Southampton Biomedical Research Centre (IS-BRC-1215-20004), the British Heart Foundation (RG/15/17/3174) and by the European Union (Erasmus + Programme Early Nutrition eAcademy Southeast Asia-573651-EPP-1-2016-1-DE-EPPKA2-CBHE-JP and ImpENSA).
Author information
Authors and Affiliations
Contributions
The authors’ responsibilities were as follows: YSL, LP-CS, KHT, FY, KMG, Y-SC, JGE, BFPB and AR-G were responsible for conceiving designing and leading the GUSTO cohort study. JYT and MF-FC designed the present work. JYT, SC, SXL and WWP contributed to the data collection. JYT, SC, SXL and WWP contributed to data processing and cleaning. MF-FC supervised and guided the data collection and cleaning process. JYT and MF-FC analysed and interpreted the data. JYT and MF-FC were responsible for drafting and finalising the manuscript. All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
K.M.G. and Y.-S.C. report being part of an academic consortium that has received research funding from Abbott Nutrition, Nestle and Danone. K.M.G. and Y.-S.C. report receiving reimbursement for speaking at conferences sponsored by companies selling nutritional products. The other authors declared no conflict of interests. The funders had no role in the choice of research project, design of this study, data collection and statistical analyses, preparation of manuscript and decision to publish.
Ethical standards
The GUSTO study was approved by the National Healthcare Group Domain Specific Review Board (D/2009/00021 and D/2014/00414) and Singhealth Centralized Institutional Review Board (2018/2767/D). All procedures were performed in line with the principles of the 1964 Declaration of Helsinki and its later amendments. All participants gave their informed written consent at each study visit. The GUSTO study was registered at http://www.clinicaltrials.gov as NCT01174875.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Toh, J.Y., Cai, S., Lim, S.X. et al. Nutrient trajectories during infancy and their associations with childhood neurodevelopment. Eur J Nutr 62, 2429–2439 (2023). https://doi.org/10.1007/s00394-023-03164-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00394-023-03164-2