
Abstract
Purpose
To provide updated information on trends and determinants of underweight, overweight, and obesity in Italian adults.
Methods
We considered data from 5 surveys conducted annually between 2006 and 2010, on a total of 14,135 subjects aged 18 years or more (6,834 men and 7,301 women), representative of the Italian adult population, including self-reported information on height and weight.
Results
Overall, 3.1 % of the Italian adult population was underweight (body mass index, BMI, <18.5 kg/m2; 0.8 % men, 5.3 % women), 31.8 % overweight (25≤ BMI <30 kg/m2; 39.8 % men, 24.4 % women), and 8.9 % obese (BMI ≥30 kg/m2; 8.5 % men, 9.4 % women). We observed no specific pattern of overweight/obesity across calendar years in men (multivariate prevalence ratios, PR, for 2010 vs 2006: 0.95; p for trend: 0.980) and a non-significant decreased trend in women (PR: 0.92; p for trend: 0.051). Prevalence of overweight/obesity significantly increased with age (PRs for ≥65 vs 18–24 years: 2.01 in men, 2.65 in women), decreased with education (PRs for high vs low education: 0.79 in men, 0.54 in women), and was less frequent in single than in married adults (PRs: 0.85 in men, 0.78 in women). Overweight/obesity was significantly more frequent in adults from southern versus northern Italy (PRs: 1.13 in men, 1.32 in women) and in former versus never smokers (PRs: 1.23 in men, 1.19 in women).
Conclusions
In Italy, we did not find unfavorable trends in overweight and obesity prevalence across calendar years. However, there are specific subgroups of the population with elevated prevalence of overweight and obesity, mainly adults from southern Italy and less educated ones.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Over the last few decades, overweight and obesity increased worldwide and became a major public health challenge not only in high-income countries but also in middle- and low-income ones [1–6].
In the USA, the 2007–2008 prevalence of overweight and obesity (body mass index, BMI, ≥25 kg/m2) was 68.0 % overall, 72.3 % among men, and 64.1 % among women [2], with a significant increasing trend over the last decade in men (odds ratio for 2007–2008 vs 1999–2000:1.32), and no particular pattern in women [2]. The rate of obesity has more than doubled over the past 30 years in most countries of northern Europe, including the UK and Scandinavian countries, as well as selected southern European countries [6, 7]. More recent data showed that, globally, 15.5 % of European adult population in 2008 was obese [7].
Among European countries, Italy had relatively favorable obesity prevalence and trends in adults [1, 8]. The prevalence of overweight and obesity modestly increased between the early 1980s (27 % of adult population was overweight and 7 % obese in 1983) and the late 1990s and levelled off thereafter (31–34 % overweight and 8–9 % obese between 1999 and 2004) [6, 8]. Subsequent studies based on national representative data showed that the age-standardized prevalence of overweight/obesity slightly increased from 52.0 to 55.3 % in men between 2001 and 2008 and from 33.6 to 34.5 % in women [9]. Italy is now among the European countries with the lowest adult obesity prevalence [1, 6, 7]. However, within Italy, differences in BMI have been reported according to geographic area, the prevalence of obesity being approximately two-fold higher in southern Italy than in northern Italy [8].
Moreover, scanty information is available in Italy, as in Europe, on underweight prevalence in adult populations, and no data are available on moderate to severe thinness [6].
In order to monitor underweight, overweight, and obesity in Italy and identify their determinants, we analyzed data from surveys conducted annually on representative samples of Italian adults between 2006 and 2010.
Subjects and methods
Since 2001, the Italian Institute of Health (Istituto Superiore di Sanità, ISS) has commissioned DOXA, the Italian branch of the Gallup International Association, to conduct annual surveys [8]. Each survey was based on about 3,000 individuals representative of the general Italian population aged 15 or over (about 52 million inhabitants) in terms of age, sex, geographic area, and socio-economic characteristics. The overall sample of the surveys conducted between 2006 and 2010 included 14,810 subjects (7,110 men and 7,700 women) aged 18 years or over. Of them, 675 subjects (4.6 %) did not report information on height or weight. Therefore, for the present analysis, we considered data collected in 5 consecutive surveys between 2006 and 2010 on a total sample of 14,135 adults (6,834 men and 7,301 women), aged 18 or over, with available information on height and weight. For the analysis of trends over time, we also considered data from a survey conducted in 2004 [8], also including information on anthropometric measures.
In each survey, the sample was defined through a representative multistage sampling of adults from 122 municipalities (the smallest Italian administrative divisions) in the 20 Italian regions (the largest Italian administrative divisions), identified in order to be representative of the geographic areas sampled. Individuals were randomly selected from electoral lists, within strata of sex and age group, in order to be representative of the demographic structure of the adult population. Statistical weights were used to assure the representativeness of each sample.
Data were collected by ad hoc trained interviewers, using a structured questionnaire in the context of a computer-assisted personal in-house interview (CAPI). Besides general information on socio-demographic characteristics, subjects were asked to report their height (cm) and weight (kg). From height and weight, we computed BMI as the ratio between weight (in kg) and height (in m2). BMI was then categorized in four levels, according to the standard classification by the World Health Organization [5], that is, underweight (BMI <18.5 kg/m2), normal weight (BMI between 18.5 and 24.9 kg/m2), overweight (BMI between 25.0 and 29.9 kg/m2), and obesity (BMI ≥30.0 kg/m2). Moderately to severely thin subjects were defined as individuals with a BMI <17.0 kg/m2. We further categorized obesity in 3 levels, according to its severity (I class obesity: BMI between 30.0 and 34.9 kg/m2; II class obesity: BMI between 35.0 and 39.9 kg/m2; III class obesity: BMI ≥40.0 kg/m2). Education was categorized in three levels: low (up to primary school diploma), intermediate (up to high school diploma), and high (university diploma). Area of residence (urban/rural) was classified according to the fact the municipality of residence was a provincial capital or not.
We computed, separately for men and women, the prevalence rate (%) of BMI categories overall and in strata of survey year, age group, level of education, income (based on self report or estimate by the interviewer), marital status, geographic area, area of residence, tobacco smoking, and alcohol drinking. For education, marital status, tobacco smoking, and alcohol drinking, age-standardized prevalence was provided, using the direct method separately for men and women. p-values for comparisons were derived using t-test for continuous variables and χ2 test for categorical ones. Prevalence ratios (PR) and corresponding 95 % confidence intervals (CI) were derived using multiplicative generalized linear models (log-binomial model) [10, 11], after adjustment for calendar year, age, education, marital status, geographic area, area of residence, tobacco smoking, and alcohol drinking.
Results
Table 1 shows the distribution of 14,135 Italian adults, according to selected self-reported anthropometric characteristics. Mean height was 168.8 cm, mean weight was 70.2 kg, and mean BMI was 24.6 kg/m2 (25.3 in men, 23.9 in women). Overall, 3.1 % of the Italian adult population were underweight (0.8 % of men, 5.3 % of women), 56.1 % were normal weight (50.9 % of men, 60.9 % of women), 31.8 % were overweight (39.8 % of men, 24.4 % of women), and 8.9 % were obese (8.5 % of men, 9.4 % of women). Prevalence of moderate to severe thinness was 0.2 % (16 subjects) among men and 0.8 % (60 subjects) among women. Overall, 7.4 % of the Italian adult population had a I class obesity, 1.2 % a II class, and 0.3 % a III class obesity.
Figure 1 shows the prevalence distribution of overweight and obesity by sex according to six DOXA surveys conducted between 2004 and 2010. For men, mean BMI was 25.5 in 2006, 25.1 in 2007, 25.2 in 2008, 25.5 in 2009, and 25.3 kg/m2 in 2010, corresponding to a linear trend of +0.004 kg/m2 per year (p = 0.898). Mean BMI for women was 24.1 in 2006, 24.0 in 2007, 23.8 in 2008, 23.8 in 2009, and 23.9 kg/m2 in 2010, corresponding to a linear trend of −0.068 kg/m2 per year (p = 0.067).

Sex-specific prevalence (%) of self-reported overweight and overweight/obesitya among males and females aged 18 years or over, according to 6 DOXA surveysb. Italy, 2004–2010. aOverweight: body mass index, BMI 25.0–29.9 kg/m2; overweight/obesity: BMI ≥25.0 kg/m2. bData from the 2004 survey were obtained by Gallus et al., 2006 [8]
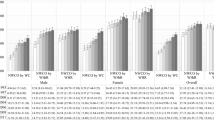
Figure 2 shows the prevalence distribution of men and women across levels of BMI in strata of age. Younger adults (aged 18–24 years) were more frequently underweight than older adults (aged ≥25 years) (2.8 vs 0.6 %, p-value <0.001, in men and 12.8 vs 4.5 %, p-value <0.001, in women). Adults reporting a BMI <17 kg/m2 were more prevalent among the young as compared to older populations (1.0 vs 0.1 %; p < 0.001, in men, 2.0 vs 0.7 %; p = 0.001, in women). Overweight/obesity (BMI ≥25.0 kg/m2) was reported by 17.0 % of adults aged 18–24 years (22.6 % of men and 11.1 % of women). The highest prevalence of overweight/obesity was observed in the elderly, both in men (61.3 % at ≥65 years vs 45.2 % at <65 years, p-value <0.001) and in women (54.6 % at ≥65 vs 26.8 % at <65 years, p-value <0.001).

Sex-specific prevalence (%) of self-reported overweight (in grey) and obesitya (in black) among males and females aged 18 years or over, according to age group. Italy, 2006–2010. aOverweight: body mass index, BMI, 25.0–29.9 kg/m2; Obesity: BMI ≥30.0 kg/m2; M males, F females
Table 2 shows the sex-specific distribution of BMI levels according to selected individual characteristics. Underweight was more frequent among adults with the highest level of education (1.4 % in men, 6.4 % in women), widowed men (4.2 %), and single women (7.6 %), adults from northern Italy (1.1 % in men, 6.3 % in women), male ex-smokers (1.5 %), and female current smokers (9.1 %). Obesity was more frequent among adults with lower level of education (11.6 % in men, 12.7 % in women), adults with lower income (11.3 % in men, 14.4 % in women), adults from southern Italy (9.7 % in men, 11.8 % in women) and from rural areas of residence (9.4 % in men, 10.2 % in women), divorced/separated men (10.4 %) and widowed women (17.2 %), ex-smokers (11.7 % in men, 11.9 % in women), and never alcohol drinkers (11.9 % in men, 10.9 % in women).
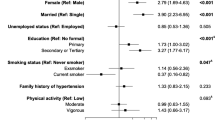
Table 3 shows the sex-specific PRs of overweight/obesity versus normal weight according to selected characteristics. No particular pattern was evident according to calendar year for men (compared to 2006, multivariate PRs were 0.93 in 2007, 0.92 in 2008, 1.02 in 2009, and 0.95 in 2010; p = 0.980), while a borderline significant inverse trend was shown for women (PRs were 0.93 in 2007, 0.92 in 2008, 0.91 in 2009, and 0.92 in 2010; p = 0.051). The inverse trend in women was observed in southern Italy (PR for 2010 vs 2006 was 0.82), whereas no difference was evident in northern (PR was 1.01), or in central Italy (PR was 1.00). When considering pattern according to calendar year among the young (1,383 subjects aged 18–24 years), no significant difference was shown both in men (compared to 2006, PRs were 0.97 in 2007, 0.76 in 2008, 0.98 in 2009, and 1.08 in 2010) and women (PRs were 0.97 in 2007, 0.55 in 2008, 1.29 in 2009, and 1.08 in 2010). Multivariate analysis confirmed that overweight prevalence increases with increasing of age (compared to <25 years, PR for 25–44 was 1.57 in men and 1.31 in women, for 45–64 was 2.08 in men and 2.34 in women, for ≥65 years was 2.01 in men and 2.65 in women). Higher educated subjects had significantly lower prevalence of overweight (compared with lower educated individuals, PRs were 0.94 and 0.67 for intermediate and high level of education in men, and 0.79 and 0.54 in women, respectively). This was consistent according to geographic area (PRs for high vs low education were 0.82 in northern, 0.70 in central, and 0.81 in southern Italy in men, and PRs were 0.45 in northern, 0.50 in central, and 0.64 in southern Italy in women). After further allowance for income, PR estimates for education did not substantially change (PRs were 0.96 and 0.82 for intermediate and high level of education in men, and 0.68 and 0.56 in women, respectively). As compared to subjects with low income, those with high income were less frequently overweight/obese (PRs were 0.91 in men and 0.89 in women). With reference to marital status, single adults and divorced/separated women had significantly lower overweight/obesity rates (PR was 0.85 in men and 0.78 in women for single vs married individuals, and PR was 0.79 for divorced/separated vs married women). As compared to northern Italy, higher overweight/obesity rates were observed in women (PR was 1.16) but not in men from central Italy, and both in men and women from southern Italy (PR was 1.13 in men and 1.32 in women). Men living in rural areas had higher overweight/obesity rates as compared to urban areas (PR was 1.07), but no significant difference was observed in women. As compared to never smokers, male current smokers (PR was 1.08) and ex-smokers (PRs were 1.23 and 1.19 in men and women, respectively) had higher overweight/obesity rates. In women, alcohol drinkers showed lower overweight/obesity rates (compared to never drinkers, PRs were 0.90 and 0.91 for <6 and ≥6 drinks per week, respectively). No significant difference across alcohol drinking was observed in men.
Discussion
Our data confirm that in the Italian population the prevalence of obesity is persistently low as compared to other populations from high-income countries [1, 2, 6, 7, 9].
In a recent report, Italy was considered among the countries with the most virtuous trends in terms of BMI for both sexes, with an estimated increase in BMI by 0.3–0.4 kg/m2 per decade for men and decrease by 0.1–0.2 kg/m2 per decade for women between 1980 and 2008 [1]. We found a further improvement in these favorable trends over more recent calendar years, the BMI being stable in men and slightly decreasing in women, despite the continuous aging of the Italian population. The slight decrease of overweight/obesity in women is limited to southern Italy. This likely reflects a reduced social acceptability of overweight/obesity in southern Italy, an area with a relatively high obesity prevalence. A favorable pattern in BMI has also been shown in selected eastern European countries, including Romania, Bulgaria, Lithuania, and Slovakia [6]. Conversely, several other European countries have recently showed a substantial BMI increase [1, 6]. In the UK—the European country with the highest levels of BMI—obesity rates rose from 10 % in 1987 to 19 % in 1998, up to 25 % in 2008 [7, 12]. Similarly, in Finland obesity increased from 11.3 to 20.7 % in men and from 17.9 to 24.1 % in women, between the late 1970s and the early 2000s [13].
Stratified analysis allowed to identify subgroups of Italian population at higher prevalence of both overweight and obesity, as well as underweight. The elderly appeared to be at higher risk of overweight and obesity in both sexes. On the contrary, only a small proportion of young adults were obese. Among women, but not among men, we found a considerably high prevalence of underweight, underlying previously reported discrepancies in underweight rate by sex in young adults in Italy [14] and Switzerland [15]. Our study provides the first Italian—and one of the first European [6]—estimate on prevalence of subjects with BMI <17 kg/m2. These data suggest that prevalence of moderate to severe thinness in young girls should be monitored.
Socio-economic characteristics are important determinants of overweight and obesity. Thus, less educated men and women have considerably higher levels of BMI, confirming findings from other investigations conducted in high-income European countries [16], the USA [17], and also in selected low- and middle-income countries [18]. A recent study combining data from 19 European countries showed that this is a generalized phenomenon of the European populations, particularly in women. However, in men from middle-income countries, including the Baltic and eastern European countries, weak positive associations between education and overweight were observed [16]. Accordingly, subjects with higher income were more frequently overweight/obese as compared to individuals with lower income.
In Italy, less privileged areas (southern Italy) showed higher levels of BMI compared to more affluent areas (northern Italy), confirming results from previous studies on Italian adults [8]. Differences in obesity prevalence according to geographic areas might be due to different socio-economical status, lifestyle, and dietary habits.
In agreement with our previous study [8], we did not find any major difference in obesity rates according to urbanization of the area of residence, these findings being similar to those from a 16,695-subject study carried out on 10 European countries [19].
With reference to marital status, we found higher rates of overweight/obesity in married as compared to either single or divorced/separated adults. Similar results were reported in national representative surveys conducted in other Mediterranean areas [20]. These findings are in broad agreement with those from longitudinal studies observing that entering marriage is associated with weight gain, while leaving marriage with weight loss [21, 22]. The relationship between marital status and overweight underlines how social characteristics can have a great influence on diet, physical activity, and consequently body weight [22, 23].
Although we found no relation between current smoking and overweight/obesity among women, our data show that male current smokers were more frequently overweight and obese as compared to never smokers. These findings are in partial disagreement with other data suggesting that current smokers have lower BMI than never smokers [24–28]. However, additional data support our findings. In Italy, it has been reported that while smokers tend to be leaner than non-smokers, there is no linear trend with number of cigarettes smoked [27, 29]. A study conducted in Israel over 29,745 young adults showed that the rate of smoking was lowest in normal weight subjects, higher in overweight, and highest in obese individuals [30]. Moreover, compared to non-smokers, current smokers have been reported to have a larger waist circumference, higher waist-to-hip ratio [26], and among current smokers, cigarette intensity is associated with increased rates of obesity and central fat accumulation [31, 32]. With reference to ex-smokers, we found that they were more frequently overweight/obese than never smokers, confirming the overall evidence of substantial weight gain after smoking cessation [25, 28, 33].
In our population, female alcohol drinkers were less frequently overweight and/or obese as compared to abstainers; among men, although abstainers were more frequently obese than drinkers, no significant difference was observed among drinkers and non-drinkers in terms of overweight/obesity. These data are in contrast with short-term laboratory-based studies on the unfavorable effects of alcohol on appetite and energy balance, but in broad agreement with the overall evidence from epidemiological studies, suggesting that moderate alcohol intake is inversely related with obesity, particularly in women [34, 35].
Potential limitations of our investigation include those inherent to the cross-sectional study design. An important weakness of our study is the use of self-reported information on height and weight, which complicates the interpretation of BMI results, and, more importantly, may lead to an under-estimate of BMI, and consequently of the prevalence of overweight and obesity. It is well known in fact that people tend to overestimate height and to underestimate weight [36–38]. However, in 3 large surveys validating self-reported with measured height and weight in adults [36–38], the over-estimation of height ranged between +0.38 and +1.23 cm in men, and between +0.40 and +0.68 cm in women, while the under-estimation of weight ranged between +0.30 and −1.85 kg in men, and between −0.85 and −1.40 kg in women. In addition, considering a worst-case analysis, thus subtracting from the height of our population the highest amount of over-reporting of height observed among the three studies and adding up to the weight of our population the highest amount of under-reporting, the prevalence of obesity would have increased to 12.3 % in men and 11.9 % in women and would have still been substantially lower than that observed in countries from central, eastern, and western Europe, North America, and Oceania [1]. Most estimates in those countries, in any case, are based on self-reported height and weight, too. The strengths of our study include its large sample size and the representativeness of the general Italian population. Moreover, the use of a CAPI survey administered by trained interviewers allowed us to avoid routing errors and to obtain more valid and reliable data on height and weight [39].
In conclusion, the present study indicates relatively favorable patterns and trends in Italy in terms of overweight and obesity prevalence compared to most other high-income countries. This might be in part due to the “Mediterranean diet”, still widespread in Italy [40], to culturally driven dietary habits as well as to the absence of a systematic increase in food portion size. However, there are specific subgroups of the population with elevated prevalence of overweight and obesity, mainly populations from southern Italy and with lower levels of education or income.
References
Finucane MM, Stevens GA, Cowan MJ, Danaei G, Lin JK, Paciorek CJ, Singh GM, Gutierrez HR, Lu Y, Bahalim AN, Farzadfar F, Riley LM, Ezzati M (2011) National, regional, and global trends in body-mass index since 1980: systematic analysis of health examination surveys and epidemiological studies with 960 country-years and 9.1 million participants. Lancet 377(9765):557–567
Flegal KM, Carroll MD, Ogden CL, Curtin LR (2010) Prevalence and trends in obesity among US adults, 1999–2008. JAMA 303(3):235–241
Kelly T, Yang W, Chen CS, Reynolds K, He J (2008) Global burden of obesity in 2005 and projections to 2030. Int J Obes (Lond) 32(9):1431–1437
Prentice AM (2006) The emerging epidemic of obesity in developing countries. Int J Epidemiol 35(1):93–99
WHO (2000) Obesity: preventing and managing the global epidemic. WHO Obesity Technical Report Series 894. World Health Organization (WHO), Geneva, Switzerland
WHO (2011) Global database on body mass index. World Health Organization (WHO), Geneva, Switzerland. Available online at: http://apps.who.int/bmi/index.jsp
OECD (2010) Health at a glance: Europe 2010, OECD Publishing. Available online at: http://dx.doi.org/10.1787/health_glance-2010-en
Gallus S, Colombo P, Scarpino V, Zuccaro P, Negri E, Apolone G, La Vecchia C (2006) Overweight and obesity in Italian adults 2004, and an overview of trends since 1983. Eur J Clin Nutr 60(10):1174–1179
Micciolo R, Di Francesco V, Fantin F, Canal L, Harris TB, Bosello O, Zamboni M (2010) Prevalence of overweight and obesity in Italy (2001–2008): is there a rising obesity epidemic? Ann Epidemiol 20(4):258–264
Skov T, Deddens J, Petersen MR, Endahl L (1998) Prevalence proportion ratios: estimation and hypothesis testing. Int J Epidemiol 27(1):91–95
Zocchetti C, Consonni D, Bertazzi PA (1997) Relationship between prevalence rate ratios and odds ratios in cross-sectional studies. Int J Epidemiol 26(1):220–223
Zaninotto P, Head J, Stamatakis E, Wardle H, Mindell J (2009) Trends in obesity among adults in England from 1993 to 2004 by age and social class and projections of prevalence to 2012. J Epidemiol Community Health 63(2):140–146
Lahti-Koski M, Seppanen-Nuijten E, Mannisto S, Harkanen T, Rissanen H, Knekt P, Rissanen A, Heliovaara M (2010) Twenty-year changes in the prevalence of obesity among Finnish adults. Obes Rev 11(3):171–176
ISTAT (2005) Stili di vita e condizioni di salute. Indagine multiscopo sulle famiglie “Aspetti della vita quotidiana”, Rome 2003: Available online at: http://www.istat.it/dati/catalogo/20051118_00
Eichholzer M, Bovey F, Jordan P, Schmid M, Stoffel-Kurt N (2010) [Body weight related data: results of the 2007 Swiss Health Survey]. Praxis (Bern 1994) 99(15):895–906
Roskam AJ, Kunst AE, Van Oyen H, Demarest S, Klumbiene J, Regidor E, Helmert U, Jusot F, Dzurova D, Mackenbach JP (2010) Comparative appraisal of educational inequalities in overweight and obesity among adults in 19 European countries. Int J Epidemiol 39(2):392–404
Freedman DS, Khan LK, Serdula MK, Galuska DA, Dietz WH (2002) Trends and correlates of class 3 obesity in the United States from 1990 through 2000. JAMA 288(14):1758–1761
Monteiro CA, Conde WL, Lu B, Popkin BM (2004) Obesity and inequities in health in the developing world. Int J Obes Relat Metab Disord 28(9):1181–1186
Peytremann-Bridevaux I, Faeh D, Santos-Eggimann B (2007) Prevalence of overweight and obesity in rural and urban settings of 10 European countries. Prev Med 44(5):442–446
Tur JA, Serra-Majem L, Romaguera D, Pons A (2005) Profile of overweight and obese people in a Mediterranean region. Obes Res 13(3):527–536
Jeffery RW, Rick AM (2002) Cross-sectional and longitudinal associations between body mass index and marriage-related factors. Obes Res 10(8):809–815
Sobal J, Rauschenbach B, Frongillo EA (2003) Marital status changes and body weight changes: a US longitudinal analysis. Soc Sci Med 56(7):1543–1555
Averett SL, Sikora A, Argys LM (2008) For better or worse: relationship status and body mass index. Econ Hum Biol 6(3):330–349
Healton CG, Vallone D, McCausland KL, Xiao H, Green MP (2006) Smoking, obesity, and their co-occurrence in the United States: cross sectional analysis. BMJ 333(7557):25–26
Munafo MR, Tilling K, Ben-Shlomo Y (2009) Smoking status and body mass index: a longitudinal study. Nicotine Tob Res 11(6):765–771
Shimokata H, Muller DC, Andres R (1989) Studies in the distribution of body fat. III. Effects of cigarette smoking. JAMA 261(8):1169–1173
Tavani A, Negri E, La Vecchia C (1994) Determinants of body mass index: a study from northern Italy. Int J Obes Relat Metab Disord 18(7):497–502
Xu F, Yin XM, Wang Y (2007) The association between amount of cigarettes smoked and overweight, central obesity among Chinese adults in Nanjing, China. Asia Pac J Clin Nutr 16(2):240–247
Pagano R, Negri E, Decarli A, La Vecchia C (1987) Smoking and weight in the 1983 Italian National Health Survey. Int J Obes 11(4):333–338
Zimlichman E, Kochba I, Mimouni FB, Shochat T, Grotto I, Kreiss Y, Mandel D (2005) Smoking habits and obesity in young adults. Addiction 100(7):1021–1025
Bamia C, Trichopoulou A, Lenas D, Trichopoulos D (2004) Tobacco smoking in relation to body fat mass and distribution in a general population sample. Int J Obes Relat Metab Disord 28(8):1091–1096
Clair C, Chiolero A, Faeh D, Cornuz J, Marques-Vidal P, Paccaud F, Mooser V, Waeber G, Vollenweider P (2011) Dose-dependent positive association between cigarette smoking, abdominal obesity and body fat: cross-sectional data from a population-based survey. BMC Public Health 11(1):23
Flegal KM, Troiano RP, Pamuk ER, Kuczmarski RJ, Campbell SM (1995) The influence of smoking cessation on the prevalence of overweight in the United States. N Engl J Med 333(18):1165–1170
Yeomans MR (2010) Alcohol, appetite and energy balance: is alcohol intake a risk factor for obesity? Physiol Behav 100(1):82–89
Wang L, Lee IM, Manson JE, Buring JE, Sesso HD (2010) Alcohol consumption, weight gain, and risk of becoming overweight in middle-aged and older women. Arch Intern Med 170(5):453–461
Merrill RM, Richardson JS (2009) Validity of self-reported height, weight, and body mass index: findings from the National Health and Nutrition Examination Survey, 2001–2006. Prev Chronic Dis 6(4):A121
Niedhammer I, Bugel I, Bonenfant S, Goldberg M, Leclerc A (2000) Validity of self-reported weight and height in the French GAZEL cohort. Int J Obes Relat Metab Disord 24(9):1111–1118
Spencer EA, Appleby PN, Davey GK, Key TJ (2002) Validity of self-reported height and weight in 4808 EPIC-Oxford participants. Public Health Nutr 5(4):561–565
Galesic M, Tourangeau R, Couper MP (2006) Complementing random-digit-dial telephone surveys with other approaches to collecting sensitive data. Am J Prev Med 31(5):437–443
Rossi M, Negri E, Bosetti C, Dal Maso L, Talamini R, Giacosa A, Montella M, Franceschi S, La Vecchia C (2008) Mediterranean diet in relation to body mass index and waist-to-hip ratio. Public Health Nutr 11(2):214–217
Acknowledgments
This work was conducted with contributions from the Italian Ministry of Health and the Italian Association for Cancer Research (AIRC grant number 10068).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Gallus, S., Odone, A., Lugo, A. et al. Overweight and obesity prevalence and determinants in Italy: an update to 2010. Eur J Nutr 52, 677–685 (2013). https://doi.org/10.1007/s00394-012-0372-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00394-012-0372-y