
Abstract
Purpose
We report an unusual case of endometriosis of the appendix with simultaneous invasion of the sigmoid colon.
Methods
Clinical, radiological, surgical, and histological data of the patient were reviewed, as well as the current literature on gastrointestinal endometriosis.
Results
A 41-year-old woman presented to the emergency department of our hospital with acute right lower quadrant pain, pronounced tenderness elevated white blood cell count, and increased C-reactive protein. Abdominal CT scan suggested a mucocele of the appendix. The patient was first treated with antibiotics, followed by en bloc resection of the appendix and of the sigmoid colon 2 months later. Histological examination revealed an endometriotic nodule of the appendix filling the appendiceal lumen and resulting in a mucocele which invaded the sigmoid colon wall.
Conclusions
The diagnosis of gastrointestinal endometriosis can be challenging due to the variety of symptoms it can produce. Although extremely rare, a concomitant double gastrointestinal location of endometriosis may be possible and should be considered in women of reproductive age.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Endometriosis is a common, benign, estrogen-dependent, chronic gynecological disorder characterized by the presence of uterine endometrial tissue outside its normal location. It affects 6 to 10% of women of reproductive age [1]. The presence of ectopic endometrial tissue and the resultant inflammatory reaction can cause devastating symptoms, including chronic pelvic pain, dysmenorrhea, dyspareunia, and infertility [2]. The pelvic cavity is the most common location for endometriotic implants, which usually affect the retrocervical space, ovaries, vagina, rectosigmoid colon, bladder dome, and round ligaments [3]. Extrapelvic endometriosis is a rare entity, with the most common location being the gastrointestinal tract. The sigmoid colon is most commonly involved, followed by the rectum, ileum, appendix, and caecum [4].
Endometriosis of the appendix is a rare manifestation and is most often reported as an incidental finding [5]. Appendiceal endometriosis can imitate symptoms of acute or chronic appendicitis, and is also known to cause cyclic and chronic right lower quadrant pain, melena, lower intestinal hemorrhage, cecal intussusception, and intestinal perforation [6]. Endometriosis can also be a rare cause of mucocele, which is a distended mucous-filled appendix secondary to obstruction [5]. Even more rarely, endometriosis can have a simultaneous double gastrointestinal location manifested by atypical intestinal symptoms and signs.
We report herein an unusual case of a 41-year-old woman suffering from appendiceal endometriosis with concomitant sigmoid colon involvement, which was successfully treated by en bloc surgical resection of the involved segments.
Case report
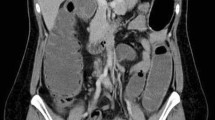
A 41-year-old woman, with no significant past medical history, presented to our hospital in March 2018 with sudden onset of abdominal pain in the right lower quadrant, accompanied by lower back pain and nausea. At physical examination, pronounced tenderness in the lower abdominal quadrants and a positive right psoas sign were found. Admission laboratory tests showed a white blood cell (WBC) count of 13,000/mm3 and a C-reactive protein (CRP) of 94 mg/l. Abdominal and pelvic CT scan revealed a short but enlarged appendix (27 mm × 19 mm) with an intraluminal mucocele-like mass and periappendiceal fat infiltration (Fig. 1). The patient was hospitalized and antibiotic therapy with amoxicillin/clavulanate was initiated for a total duration of 7 days. The patient was discharged at postoperative day 5, with a normal WBC count and a CRP at 33 mg/l. A colonoscopy performed 4 weeks later did not reveal any abnormal findings, except a millimeter-sized polyp that was resected. Histopathological examination of this small polyp revealed a hyperplastic polyp.

Preoperative contrast-enhanced abdominal CT scan showing an enlarged appendix with an intraluminal mass and periappendiceal fat infiltration (arrow)
Surgery was performed in May 2018, after surgical meeting validation, anesthesiology evaluation, and patient’s written informed consent. Initial planning consisted of simple laparoscopic appendectomy without rupture of the lesion in case of a normal appendiceal base, or, eventually, laparoscopic ileocecal resection in case of tumor invasion of the appendiceal base. Trocars were placed as for classic laparoscopic appendectomy (a 12-mm trocar at the umbilicus for the camera and two 5-mm trocars in suprapubic and left iliac fossa positions). The appendix found in the right iliac fossa showed no signs of inflammation but presented two round lesions at its distal end. Extreme care was taken throughout the procedure to avoid rupture of these lesions. Further exposition of the appendix revealed strong adhesion of the more distal appendiceal lesion to the terminal ileum (at 20 cm from the ileocecal valve) as well as to the sigmoid colon (Fig. 2). Careful dissection was initiated at the plane between the appendix and the terminal ileum, with successful dissociation of the two structures and without rupturing the appendiceal mass. Dissection was then carried out to the plane between the appendiceal mass and the sigmoid colon, with impossibility to dissociate the two structures due to tumor invasion of the sigmoid colon. In the context of mucocele suspicion, decision to convert to laparotomy was taken and a 10-cm lower midline incision was performed. En bloc appendectomy and segmental sigmoid colon resection were performed, with subsequent end-to-end anastomosis of the sigmoid colon. Nasogastric tube or abdominal drainage was not applied.

Intraoperative view showing adhesion of the appendiceal mass (long black arrow) to the terminal ileum (short black arrow) and to the sigmoid colon (white arrow)
Operative time was 98 min and blood loss minimal (50 ml). Postoperative course was uneventful. Gastrointestinal transit resumed at postoperative day 2 and then oral intake was progressively introduced. The patient was discharged on postoperative day 4. Microscopic examination of the specimen revealed a voluminous endometriotic nodule of the appendix filling completely the appendiceal lumen and resulting in a mucocele, invading partially the sigmoid wall with absence of dysplasia or malignancy (Fig. 3). Colonoscopy performed 3 months after surgery was normal. The patient remains in good health 6 months after surgery.

Macroscopic examination of the resected surgical specimen: a Appendix specimen, 4.5 cm long, with (A1) pseudotumoral enlargement of the head and evidence of wall perforation with mucous leak (arrow); (A2) on cut section, obstruction of the appendiceal lumen by white fascicular endometriotic nodule of 1.3 cm with bluish microcysts. b Transversal section of sigmoid resection specimen (9.5 × 7 cm) showing the invaded part of the sigmoid colon wall (arrow)
Discussion
Endometriosis is defined as the presence of endometrial mucosa outside the uterine cavity. The most widely accepted theory is retrograde menstruation of endometrial tissue through the fallopian tube into the pelvis [7]. Moreover, in patients with endometriosis, immunological dysregulation may prevent normal clearance of ectopic endometrial cells facilitating their implantation [8]. Other theories implicated in endometriosis are the coelomic metaplasia theory according to which normal peritoneal tissue mutates into ectopic endometrial tissue [9], bone marrow-derived stem/progenitor cells that differentiate in endometriotic tissue [10], or embryonic Mullerian rest according to which cell residual from Mullerian duct develop into endometriotic tissue under the estrogen stimulation at puberty [9].
Although endometriosis is a quite common pathology among women of reproductive age, gastrointestinal tract involvement occurs in only 12–15% of cases [11]. The most common presentation of gastrointestinal endometriosis is a cramp-like lower abdominal pain that follows the menstrual cycle. Other symptoms are constipation or diarrhea, melena, rectal bleeding, palpable mass, meteorism, and abdominal distention [12]. In some cases, as in the one reported here, gastrointestinal endometriosis can present with sudden onset abdominal pain, mimicking other conditions as, for example, acute appendicitis or intestinal obstruction. This mimicking of multiple conditions in addition to the lack of specific radiologic findings for gastrointestinal endometriosis makes accurate preoperative diagnosis difficult [4].
In the hereby presented case, preoperative examinations never suspected the presence of gastrointestinal endometriosis. Colonoscopy showed no abnormalities, since, in contrast to the appendix, the endometrioma invasion of the sigmoid colon was not transmural. Abdominal and pelvic CT scan was in favor of a mucocele. Even if magnetic resonance imaging (MRI) is the most accurate imaging modality for gastrointestinal endometriosis detection, the gold standard remains surgical resection of the involved intestinal segment and histopathological examination [4]. In our case, appendiceal endometriosis invading the sigmoid colon was an incidental finding after histopathological analysis of the resected specimen.
Surgical resection of the involved intestinal segments affected by endometriosis is the treatment of choice in presence of symptoms, such as intestinal obstruction, frequent bleeding episodes, severe pain, or malignancy suspicion [4]. After surgery, symptomatic lesion recurrences are frequent (40–50% at 5-year follow-up), especially when no postoperative adjuvant treatment is applied [13]. In the present case, the therapeutic attitude used was laparotomy with en bloc resection of the appendix and the involved part of the sigmoid colon which were impossible to dissociate during surgery. Even if laparoscopic resection of the appendix was initially intended, the suspicion of a malignant appendiceal mucocele, with fear of rupture in the peritoneal cavity and development of a pseudomyxoma peritonei, led us to convert to laparotomy. Appendiceal mucocele is a rare finding, occurring in 0.3% of appendectomy specimens [14]. It is even more rarely due to endometriosis, with only few cases reported in the literature [5]. One devastating complication of malignant mucocele is pseudomyxoma peritonei, defined as mucinous ascites of the abdomen due to dissemination of mucinous neoplastic cells throughout the peritoneal cavity. In 94% of cases of pseudomyxoma peritonei, the source of these cells is a perforated appendiceal tumor [15]. Therefore, the decision to convert to laparotomy in the present case was judicious and should not be considered a failure.
Conclusion
Endometriosis of the gastrointestinal tract is a rare finding, but remains a possible diagnosis in the context of gastrointestinal symptoms in women of reproductive age. Diagnosis of this condition is challenging, as it can mimic different conditions and has few specific clinical and radiologic findings. Surgery is currently the treatment of choice for symptomatic intestinal endometriosis. Although extremely unusual, simultaneous double gastrointestinal location is possible and must be considered. We reported here a very rare case of transmural appendiceal endometriosis invading the sigmoid wall, which was clinically expressed with acute abdominal symptoms and was successfully treated by en bloc resection of the involved intestinal segments.
References
Giudice LC (2010) Clinical practice. Endometriosis. N Engl J Med 362:2389–2398
Tai FW, Chang CY, Chiang JH, Lin WC, Wan L (2018) Association of pelvic inflammatory disease with risk of endometriosis: a nationwide cohort study involving 141,460 individuals. J Clin Med 7. https://doi.org/10.3390/jcm7110379
Chamie LP, Ribeiro D, Tiferes DA, Macedo Neto AC, Serafini PC (2018) Atypical sites of deeply infiltrative endometriosis: clinical characteristics and imaging findings. Radiographics 38:309–328
Charatsi D, Koukoura O, Ntavela IG, Chintziou F, Gkorila G, Tsagkoulis M, Mikos T, Pistofidis G, Hajiioannou J, Daponte A (2018) Gastrointestinal and urinary tract endometriosis: a review on the commonest locations of extrapelvic endometriosis. Adv Med 2018:3461209
Klingbeil KD, Azab B, Moller MG (2017) Low-grade appendiceal mucinous neoplasm and endometriosis of the appendix. World J Surg Oncol 15:226
Gustofson RL, Kim N, Liu S, Stratton P (2006) Endometriosis and the appendix: a case series and comprehensive review of the literature. Fertil Steril 86:298–303
Giudice LC, Kao LC (2004) Endometriosis. Lancet 364:1789–1799
Young S, Burns MK, DiFrancesco L, Nezhat A, Nezhat C (2017) Diagnostic and treatment guidelines for gastrointestinal and genitourinary endometriosis. J Turk Ger Gynecol Assoc 18:200–209
Burney RO, Giudice LC (2012) Pathogenesis and pathophysiology of endometriosis. Fertil Steril 98:511–519
Sasson IE, Taylor HS (2008) Stem cells and the pathogenesis of endometriosis. Ann N Y Acad Sci 1127:106–115
Tong YL, Chen Y, Zhu SY (2013) Ileocecal endometriosis and a diagnosis dilemma: a case report and literature review. World J Gastroenterol 19:3707–3710
Torralba-Moron A, Urbanowicz M, Ibarrola-De Andres C, Lopez-Alonso G, Colina-Ruizdelgado F, Guerra-Vales JM (2016) Acute small bowel obstruction and small bowel perforation as a clinical debut of intestinal endometriosis: a report of four cases and review of the literature. Intern Med 55:2595–2599
Vercellini P, Vigano P, Somigliana E, Fedele L (2014) Endometriosis: pathogenesis and treatment. Nat Rev Endocrinol 10:261–275
Aho AJ, Heinonen R, Lauren P (1973) Benign and malignant mucocele of the appendix. Histological types and prognosis. Acta Chir Scand 139:392–400
Rymer B, Forsythe RO, Husada G (2015) Mucocoele and mucinous tumours of the appendix: a review of the literature. Int J Surg 18:132–135
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Lainas, P., Dammaro, C., Rodda, G.A. et al. Appendiceal endometriosis invading the sigmoid colon: a rare entity. Int J Colorectal Dis 34, 1147–1150 (2019). https://doi.org/10.1007/s00384-019-03242-0
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00384-019-03242-0