
Abstract
Background
This study evaluated the role of the acute phase C-reactive protein (CRP) in the postoperative course of a large series of rectal resections on the basis of a prospective database. Main focus of this study was the early identification of complications.
Materials and methods
Three hundred eighty-three rectal resections with primary anastomosis for rectal cancer were screened for infectious postoperative complications. Forty-eight complicated cases were identified and matched with 48 patients with an uneventful postoperative course.
Results
In the postoperative setting, CRP peaked on postoperative day (POD) 2 with a median serum CRP of 140 mg/l and gradually declined thereafter in uncomplicated cases. In complicated cases, CRP elevation generally persisted after POD 2, whereas white blood cells and body temperature were within normal range in the early postoperative period. A cutoff CRP value of 140 mg/dl on PODs 3 and 4 resulted in predictive values of 85.7 and 90.5% (adjusted to the prevalence: 37.6 and 50.3%), sensitivities of 80.0 and 54.3%, and specificities of 81.0 and 92.3% for a complicated postoperative course (P < 0.001), respectively.
Conclusion
Persistent CRP elevation and elevation of serum CRP above 140 mg/dl on PODs 3–4 are predictive of infectious postoperative complications and should prompt intense clinical search for an inflammatory process, especially for an anastomotic leak if pneumonia and wound infection are unlikely or excluded.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
C-reactive protein (CRP) was originally identified as a serum component in patients with pneumonia that precipitated when brought into contact with a soluble extract (the C-polysaccharide) of Streptococcus pneumoniae [1]. The production of CRP occurs almost exclusively in the liver by hepatocytes as part of the acute-phase response upon stimulation by interleukin-6 (IL-6), tumor necrosis factor-α, and IL-1-β originating at the site of inflammation. It is a pentameric protein with various molecular functions including complement activation and opsonization [2]. CRP not only binds the Fc-gammaglobulin-receptor on leukocytes but also acts on endothelial cells via IL-8 activation [3, 4]. The function of CRP in vivo, however, is incompletely understood. Its short half-life (19 h) makes CRP a valuable marker to detect disease activity, inflammatory response, and postoperative recovery [5]. In healthy individuals, serum CRP is <1 mg/l but can rapidly increase up to 40 mg/l in mild inflammation or viral infections and up to 400 mg/l in severe inflammatory or septic conditions or burns [6].
CRP has been considered a strong biomarker for predicting cardiovascular risk including future myocardial infarction and stroke in the past [7–10]. Recent data, however, suggest that CRP elevation is only a moderately accurate predictor for coronary heart disease [11]. The predictive value of CRP has also been assessed for different cancers: Preoperative CRP is an independent predictor of a poor prognosis in patients with hepatocellular carcinoma, pancreatic and colon cancer, but not in rectal cancer [12–15].
CRP has already been established in clinical routine for detection of necrosis and to monitor disease severity in patients with acute pancreatitis [16, 17]. In conjunction with clinical signs and other inflammatory markers, CRP is considered as an indicator for an unfavorable postoperative course including surgical and nonsurgical complications. Previous studies examining CRP after major abdominal surgery described heterogeneous groups of patients after either surgery for colon carcinoma, colon diverticula, and reconstruction of bowel continuity (35 patients, 7 complicated cases) [18] or for diseases of the stomach, biliary tree, small and large bowel (108 patients, 40 complicated cases) [19]. However, acute-phase response and serum CRP levels depend on the infectious agent or stimulus (e.g., virus, bacteria, trauma, surgery, necrosis), the extent of inflammation or tissue injury, disease entity, and the host immune status [20]. Only recently, CRP analysis in patients after pediatric kidney and liver transplantation and in simultaneous adult pancreas–kidney transplantation demonstrated that CRP is a valuable marker for detection of postoperative complications in these homogeneous cohorts [21, 22].
To our knowledge, there are no data on serum CRP levels after a homogeneous series of open rectal surgery in uneventful and complicated postoperative courses. One of the most feared complications in rectal surgery is anastomotic leakage after reconstruction. Early detection and treatment of infectious postoperative complications can avert life-threatening conditions. The present study was designed to evaluate the role of CRP, white blood cells (WBC), and body temperature in the postoperative setting after rectal surgery and its potential in detecting infectious postoperative surgical and nonsurgical complications.
Materials and methods
Patients
Between October 2001 and November 2005, 383 rectal resections with sphincter preserving primary anastomosis were performed for rectal cancer at the Dept. of General Surgery, University of Heidelberg. Surgical resections for tumor recurrence and abdominoperineal resections were excluded. Patients’ data were recorded in a prospective database with weekly updates. Low anterior resection (LAR) was performed in 340 cases and high anterior resection (HAR) in 43 cases.
Screening and definition of infectious complications
All patients were screened retrospectively for the following infectious postoperative complications: anastomotic leak, intraabdominal abscess, wound infection, central line infection, pneumonia, and urinary tract infection (UTI).
Patients underwent further postoperative diagnostic tests or treatment only in case of symptoms or signs of an infectious complication: An anastomotic leak was verified either by a radiographic enema performed with computed tomography (CT) scan (standard for the inpatient setting), X-ray, or by endoscopy. Abscesses were verified by purulent drainage or during re-laparotomy. Wound infections were diagnosed in the presence of clear signs of inflammation at the wound margin or purulent drainage from the wound. Diagnosis of central line infection required positive blood cultures and cultures from the catheter tip. Pneumonia was diagnosed by pulmonary infiltration in chest CT scan or chest radiography accompanied by clinical symptoms of the lower respiratory tract (e.g., cough, sputum production, dyspnea) or on physical or laboratory exam (e.g., fever, altered breath sounds, leukocytosis). UTI was defined by positive urine sediment analysis combined with leukocytosis and/or fever.
Out of the 383 patients, 48 were found to have at least one of the above-mentioned infectious complications. This group was matched with patients with an uneventful postoperative course in regard to age, gender, neoadjuvant treatment, and surgical procedure (Table 1). In each group, one patient was on low dose steroids preoperatively because of asthma.
Neoadjuvant treatment and surgical technique
Briefly, the 96 patients underwent LAR in 82 and HAR in 14 cases, respectively. Eight patients underwent neoadjuvant chemoradiation, whereas 37 patients had neoadjuvant short-term radiation (5 Gy on five consecutive days). Short-term radiation was indicated in T3-stages, or lymph node positive stages except for T4-stages or a tumor location in close vicinity to the sphincter muscle both of which were indications for neoadjuvant chemoradiation. Five patients (three in the complication group and two in the control group) underwent intraoperative radiation therapy.
All patients underwent mechanical bowel preparation the day before surgery (Oralav®, Braun, Melsungen, Germany). A protective loop ileostomy was constructed in all LAR except in four cases (three in the complicated and one in the uncomplicated group). Regarding all 96 procedures, 83 patients had a loop ileostomy (40 in the complicated and 43 in the uncomplicated group, see Table 2). As a standard, LAR included total mesorectal excision, anastomosis with a CEEA stapling device (ILS, Ethicon, Norderstedt, Germany until 10/2003; Autosuture Premium Plus, USSC, Norwalk, CT, USA since 11/2003), and reconstruction with a transverse coloplasty or J-Pouch. HAR was performed with partial mesorectal excision. If not contraindicated for other reasons, mezlocillin and metronidazole were given as perioperative antimicrobial prophylaxis (in general, antibiotics were given 30 min before surgical incision with additional doses every 4 h during surgery and discontinued within 24 h after the operation). In 14 complicated and 16 uncomplicated cases, perioperative antibiotics were continued for 3 and 2 days (median), respectively.
Follow-up and treatment
Serum CRP levels, WBC counts, platelet counts, and body temperatures were recorded routinely before the operation and on PODs 1–12. If a complication did not occur within the first 12 PODs, CRP level and WBC were documented on the day the complication was diagnosed. Additionally, in patients with an anastomotic leak, CRP and WBC were assessed before and 5 days after interventional or surgical treatment. In uneventful cases (control group), the number of parameters recorded was lower toward the end of the observational period because some patients were discharged before POD 12 and laboratory data were not available on each single day.
Methods
CRP was measured by turbidometry. Levels higher than 5 mg/l were considered as elevated. A WBC count in the range from 4/nl to 10/nl and a platelet count from 150 to 440/nl were considered as normal.
Medical records of the postoperative hospital stay were reviewed on the basis of a prospective database, including patients’ morbidity, medication, operative data, laboratory data (including CRP and WBC), clinical signs (body temperature), and diagnostic and therapeutic procedures.
Thirteen (13/22) patients with anastomotic leak underwent re-laparotomy for anastomotic leak before POD 12. To exclude an increase in serum CRP due to re-laparotomy in these patients, laboratory data after the day of re-laparotomy were excluded in the graphical and statistical analysis.
Statistics
Statistical analysis of the data was performed with the SAS software (Release 9.1, SAS Institute, Cary, NC, USA). Sensitivity, specificity, the predictive value, and the area under the curve were estimated using logistic regression analyses. Data are presented as median values if not indicated otherwise. Box-and-whisker plots and line graphs (Sigma Plot, SPSS, IL, USA) were used to present CRP distribution on the day of diagnosis. Logistic regression models were used to determine whether CRP on POD 2, 3, or 4 was associated with complications. Two-sided P values were always computed, and an effect was considered statistically significant at a P value = 0.05.
The analysis of the distribution of sex, surgery, preoperative therapy, intraoperative radiation, and Union Internationale Contre le Cancer stage in the two groups was performed using Fisher’s exact test. Values for age, operation time, and postoperative hospital stay were statistically compared with the nonparametric Mann–Whitney U-test.
Results
In a 4-year period, 383 anterior resections with primary end-to-end anastomosis were performed. The complication and control group (n = 48) did not differ significantly in terms of age, gender, neoadjuvant therapy, and operative procedure (Table 1).
In 43 cases, isolated anastomotic leaks (leak rates 5.6% [19/340] in LAR, 7.0% [3/43] in HAR), wound infection, pneumonia, or UTI were diagnosed in the postoperative setting (Table 2). One patient with anastomotic leak died on POD 8 because of septic multiorgan failure, another patient with pneumonia died on POD 14 due to pulmonary decompensation. Five patients had two complications (three patients had a wound infection and pneumonia, two patients a wound combined with a central line infection) simultaneously.
Treatment in the case of pneumonia and UTI were antibiotics and drainage and antibiotics in case of wound infections. Wound infections affected exclusively the median laparotomy without dehiscence of the fascia. Patients with an anastomotic leak were treated with antibiotics alone (2/22), interventional or surgical drainage procedure without laparotomy (8/22) or re-laparotomy (13/22). One patient underwent laparotomy first, followed by a surgical drainage procedure on POD 14.
CRP and WBC at time of diagnosis
The median day of diagnosis of the complications was POD 8 (interquartile range: 5–9, for details see Table 2). On the day of complication diagnosis, serum CRP was over 20 mg/l in all cases (n = 48). Median serum CRP was 139, 110, 157, and 95 mg/l in patients with anastomotic leak, wound infection, pneumonia, and UTI, respectively (Fig. 1), whereas the median CRP was 38.7 mg/dl on POD 8 in uncomplicated cases. A CRP value over 100 mg/l had a sensitivity of 72.1% overall (anastomotic leak 86.4%, wound infection 58.3%, pneumonia 66.7%, UTI 33.3%). An abnormal WBC count had a sensitivity of 44.2% at the time point of diagnosis of a complication (anastomotic leak 36.4%, wound infection 41.7%, pneumonia 50%, UTI 100%).

Serum CRP in patients with different complications after rectal surgery on the day of diagnosis. Mean serum CRP was 139, 110, 157, and 95 mg/l in patients with anastomotic leak, wound infection, pneumonia, and UTI, respectively (white box plots). Patients presented with abnormal WBC in 8/22, 5/12, 3/6, and 3/3 cases, respectively (gray box plots). The normal range of WBC is highlighted. Whiskers indicate the 10th and 90th percentiles
Postoperative CRP and inflammatory markers
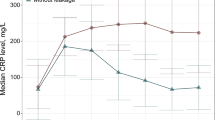
After uneventful rectal resection, serum CRP peaked on POD 2 (median CRP 140 mg/l overall; 177.8 mg/l in anastomotic leakage, 215.8 mg/l in wound infections, 165.3 mg/l in pneumonia; 144.9 mg/l in UTI and 149.0 mg/l in combined complications) and gradually decreased thereafter (Fig. 2, gray bars). CRP did not normalize during the observation period.

Serum CRP during PODs 1–12 following rectal surgery in patients with (black bars) and without (gray bars) infectious complications presented as box plot (medians connected by dashed lines). Whiskers are not plotted. Number of CRP values included in the study (of 48 cases in each group):
In patients with infectious postoperative complications, including anastomotic leak, wound infection, pneumonia, UTI, and combined complications, initial rise in CRP was higher compared to uncomplicated cases. CRP peaked on POD 2, with a median CRP of 183 mg/l, did not show a marked decline during the following days and, in most of the cases, remained elevated above 100 mg/l (Fig. 2, black bars).
The early rise and persisting elevation of CRP in complicated cases, visualized by calculation of medians (Fig. 2), was also reflected by CRP levels in single patients (not shown).
Because an early elevation of CRP was observed in complicated courses, we investigated whether WBC and temperature showed similar time courses and whether these parameters differed significantly in various complications. Early CRP elevation was evident in all complications, but did not differ significantly between anastomotic leakage, wound infection, pneumonia, and combined complications (Fig. 3a,c,e,g). In addition, the low number of detected UTI did not justify statistical analysis to compare the different complication groups.

Median serum CRP (left), WBC, and body temperature (right) preoperatively and during PODs 1–12 in patients with different complications (solid line) versus uncomplicated cases (n = 48, dashed line): anastomotic leak (a, b; n = 22), wound infection (c, d; n = 12), pneumonia (e, f; n = 6), and combined complications (g, h; n = 5). Interquartile range and medians (black) of the day of diagnosis are indicated by horizontal box plots
Whereas median WBC was within the normal range in the early postoperative period, WBC went up around POD 7, roughly reflecting the median day of diagnosis in each complication (Fig. 3b,d,f,h). There was no case of neutropenia (WBCs < 1/nl), but 23 (preoperative: three) and 17 (preoperative: three) cases with WBC count under 4/nl in the complication and control group, respectively. In both groups, the majority of cases with a WBC count under 4/nl was noted on POD 4. Body temperature was elevated predominantly in patients with pneumonia and combined complications after POD 7 (Fig. 3f,h).
Platelet counts were not significantly different in both groups, and there was a continuous increase of the median platelet count from 200/nl on POD 3 up to about 500/nl on POD 12.
We further analyzed the CRP response after treatment of anastomotic leakage. Twenty patients with anastomotic leak underwent therapeutic drainage or re-laparotomy. In 18 patients, CRP before and on day 5 after laparotomy or drainage could be assessed. In 15 cases, a decline in CRP level over 5 days after treatment was recorded, whereas CRP levels went up in three patients. Of the 13 patients who underwent re-laparotomy, six had generalized peritonitis, two had local peritonitis, and five had no macroscopic peritonitis.
Early CRP elevation in complicated cases prompted us to evaluate a serum CRP cutoff level for prediction of an unfavorable postoperative course. Assessment of a relevant cutoff level with a predictive value was considered reasonable on PODs 3 and 4 because the receiver operating characteristic curve revealed the highest area under the curve on these days. Moreover, most of the complications were clinically diagnosed later (median day of diagnosis: POD 8, see also Table 2). Logistic regression analysis revealed a sensitivity of 80.0%, a specificity of 81.0%, and a predictive value of 85.7% for complicated cases with a CRP cutoff level of 140 mg/l on POD 3, whereas the corresponding parameters on POD 4 were calculated as 54.3, 92.3, and 90.5% (Table 3), respectively. Adjustment for the prevalence of complications (48/383) results in a predictive value of 37.6 and 50.3% on PODs 3 and 4, respectively. Owing to the persistent elevation of CRP in complicated cases with a concomittant decline in uncomplicated cases, sensitivity drops to 54.3%, specificity rises to 92.3%, and the predictive value to 90.5% (cutoff: 140 mg/l) on POD 4. For statistical analysis, 51 and 61 CRP values (of 96 patients) were available on PODs 3 and 4, respectively. Combination of serum CRP on PODs 3 and 4 (n = 84 of 96) resulted in a predictive value of 83.8% for a complicated postoperative course within the group of examined patients.
Discussion
Anastomotic leak after rectal surgery is one of the most serious and life-threatening complications and continues to be a major clinical problem. Anastomotic leak rates after LAR with TME have been reported in a range from 2 to 17% [23–27]. Up to 50% of patients with anastomotic leak are asymptomatic [25] which can be explained by extraperitoneal localization of the leak. Postoperative mortality due to anastomotic complications is as high as 22% and estimated to account for one third of all deaths after colorectal surgery [28]. Surgery with rectal anastomosis is also associated with considerable morbidity rates around 20% [26, 27]. Patients who experienced anastomotic leak had a significantly inferior outcome with respect to neorectal capacity, evacuation problems, fecal urgency, and incontinence [29]. Therefore, early detection of developing complications is mandatory for reducing postoperative morbidity and patients’ long-term outcome.
In patients with anastomotic leak, clinical assessment, rectal angiography, and CT had have been reported to have a sensitivity of 50, 60, and 57%, respectively [25]. The aim of this study was to define the role of serum CRP, WBC, and body temperature for identification of patients at high risk for postoperative anastomotic leak and other infectious postoperative complications.
Recently, Wullstein et al. [22] showed that peak serum CRP within 72 h, after simultaneous pancreas–kidney transplantation, predicts pancreas graft-related complications and pancreas graft survival. After pediatric kidney and liver transplantation, elevated serum CRP was associated with rejection episodes, bacterial and viral infections, and proved to be a more sensitive marker than WBC and fever [21]. In accordance with our results, CRP tended to remain elevated in patients with an unfavorable outcome in this study. On the other hand, a peak serum CRP on POD 2 followed by a quick decline and a relatively low CRP thereafter is indicative for an uncomplicated outcome [21], which was confirmed by our present data. A peak CRP on POD 2 and a consecutive decline were also recorded in patients after laparoscopic LAR and colectomy when the invasiveness of the two procedures was examined [30]. This underlines our findings that rectal surgery alone causes significant CRP elevation with a median peak CRP of 140 mg/dl. The observation of persistent CRP elevation in complicated cases, however, implicates that inflammatory processes and activation of CRP production pre-exit before clinical manifestation and start almost immediately postoperatively. WBC count (including leukocytosis and neutropenia) and fever both did not indicate an unfavorable outcome as early as CRP elevation. CRP production is only impaired by liver failure, but plasma half-life of CRP is independent of diseases or pathological organ function, so that circulating plasma CRP is solely determined by the synthesis rate. There was no patient with liver failure in our present study. CRP synthesis rate in turn directly reflects the intensity of the inflammatory process [5]. In case of anastomotic leaks and wound infections, tissue ischemia and necrosis at the stapler line or ischemia and bacterial infection of the wound, respectively, may induce an early inflammatory response with activation of CRP production. A decreased anastomotic intramucosal pH within 24 h postoperatively was significantly associated with anastomotic leakage [31] and substantiates the theory of early local tissue malperfusion.
Contrary to anastomotic leak and wound infection, in some of the observed cases of pneumonia in our series, CRP initially declined and was followed by sudden CRP elevation shortly before clinical manifestation of pneumonia.
Although CRP production is directly stimulated by the pathological inflammatory process, CRP response after re-laparotomy for anastomotic leak was only moderate. This is probably due to the fact that most of the patients had peritonitis or were septic at the time of re-laparotomy and recovered gradually. In an intensive care unit setting, a decrease of CRP in patients with sepsis was shown to indicate higher survival or resolution of sepsis, but procalcitonin was even an earlier prognostic marker for patient outcome than CRP [32, 33]. Postoperative dynamics of procalcitonin are useful as a diagnostic parameter for complications but—compared to CRP—more obviously depend on the extent and type of surgery and thus must be interpreted critically [34]. Procalcitonin also reflected a systemic inflammatory response syndrome during the first 12 h after uncomplicated colorectal surgery, whereas CRP did not [35]. Hence, high postoperative procalcitonin levels immediately after surgery do not generally imply development of infectious complications.
Establishing a cutoff value for clinical decision making in general is often a trade-off. A predictive value of 90.5% (POD 4) in our cohort and an adjusted predictive value of 50.3% suggest that every second patient outranging the CRP cutoff has an ongoing and potentially life-threatening inflammatory process. The drawback is a lower sensitivity compared to POD 3 implicating that not all patients with infectious complications will be detected.
Low rates of complications often limit statistical analysis, which is even more aggravated if not all values are available for each day. Exclusion of parameters after reexploration in complicated cases and discharge of the patients before POD 12 in uncomplicated cases contributed to this fact in our analysis. The present study design, which was based on the analysis of a large series of rectal resections, yielded a reasonable data set of surgical and disease-specific infectious complications and allowed the authors to draw a conclusion for complicated cases, but not for each subgroup of complications. The disadvantage of this retrospective analysis is that the database was not primarily designed for the correlation of serum parameters with infectious complications. Thus, CRP data were not available for each day, and not all patients (including the control group) underwent routine screening examinations for infectious complications. A measurement bias on the basis of lacking data, therefore, cannot be excluded. Thus, asymptomatic leakages in patients with protective loop ileostomy might have not been detected. However, these patients normally do not require therapeutic intervention, and the main intention of the study was to identify complications that may later require treatment and increase morbidity, early.
In conclusion, persistent elevation of CRP and a CRP level higher than 140 mg/l on PODs 3–4 after rectal surgery with primary anastomosis should raise the degree of suspicion for infectious complications. In these cases, CRP seemed to be a sensitive, but nonspecific marker. As a consequence, these patients require special attention and probably further diagnostic tests to detect potential inflammatory processes and to avert life-threatening septic complications. If wound infection, UTI, and pneumonia can be ruled out, an intense search for anastomotic leakage is enforced by the present data. The role of procalcitonin as a complication marker in rectal surgery has still to be established.
This study supports the role of serum CRP as a helpful and relevant adjunct to clinical assessment in the postoperative setting. Further prospective trials are needed to test whether early diagnostic or therapeutic actions on the basis of CRP elevation lead to improved outcome and reduced morbidity after rectal surgery.
References
Tillet WS, Francis T (1930) Serological reactions in pneumonia with a non-protein somatic fraction of the pneumococcus. J Exp Med 52:561–571
Gabay C, Kushner I (1999) Acute-phase proteins and other systemic responses to inflammation. N Engl J Med 340:448–454
Bang R, Marnell L, Mold C, Stein MP, Clos KT, Chivington-Buck C, Clos TW (2005) Analysis of binding sites in human C-reactive protein for FcγRI, FcγRIIA, and C1q by site-directed mutagenesis. J Biol Chem 280:25095–25102
Venugopal SK, Devaraj S, Jialal I (2005) Effect of C-reactive protein on vascular cells: evidence for a proinflammatory, proatherogenic role. Curr Opin Nephrol Hypertens 14:33–37
Pepys MB, Hirschfield GM (2003) C-reactive protein: a critical update. J Clin Invest 111:1805–1812
Vermeire S, Van Assche G, Rutgeerts P (2006) Laboratory markers in IBD: useful, magic, or unnecessary toys? Gut 55:426–431
Koenig W (2005) Predicting risk and treatment benefit in atherosclerosis: the role of C-reactive protein. Int J Cardiol 98:199–206
Liuzzo G, Biasucci LM, Gallimore JR, Grillo RL, Rebuzzi AG, Pepys MB, Maseri A (1994) The prognostic value of C-reactive protein and serum amyloid a protein in severe unstable angina. N Engl J Med 331:417–424
Yeh ET (2004) CRP as a mediator of disease. Circulation 109:II11–4
Best LG, Zhang Y, Lee ET, Yeh JL, Cowan L, Palmieri V, Roman M, Devereux RB, Fabsitz RR, Tracy RP, Robbins D, Davidson M, Ahmed A, Howard BV (2005) C-reactive protein as a predictor of cardiovascular risk in a population with a high prevalence of diabetes: the Strong Heart Study. Circulation 112:1289–1295
Danesh J, Wheeler JG, Hirschfield GM, Eda S, Eiriksdottir G, Rumley A, Lowe GD, Pepys MB, Gudnason V (2004) C-reactive protein and other circulating markers of inflammation in the prediction of coronary heart disease. N Engl J Med 350:1387–1397
Jamieson NB, Glen P, McMillan DC, McKay CJ, Foulis AK, Carter R, Imrie CW (2005) Systemic inflammatory response predicts outcome in patients undergoing resection for ductal adenocarcinoma head of pancreas. Br J Cancer 92:21–23
Erlinger TP, Platz EA, Rifai N, Helzlsouer KJ (2004) C-reactive protein and the risk of incident colorectal cancer. JAMA 291:585–590
Helzlsouer KJ, Erlinger TP, Platz EA (2006) C-reactive protein levels and subsequent cancer outcomes: Results from a prospective cohort study. Eur J Cancer 42:704–707
Hashimoto K, Ikeda Y, Korenaga D, Tanoue K, Hamatake M, Kawasaki K, Yamaoka T, Iwatani Y, Akazawa K, Takenaka K (2005) The impact of preoperative serum C-reactive protein on the prognosis of patients with hepatocellular carcinoma. Cancer 103:1856–1864
Buchler M, Malfertheiner P, Schoetensack C, Uhl W, Beger HG (1986) Sensitivity of antiproteases, complement factors and C-reactive protein in detecting pancreatic necrosis. Results of a prospective clinical study. Int J Pancreatol 1:227–235
Werner J, Hartwig W, Uhl W, Muller C, Buchler MW (2003) Useful markers for predicting severity and monitoring progression of acute pancreatitis. Pancreatology 3:115–127
Reith HB, Mittelkotter U, Debus ES, Kussner C, Thiede A (1998) Procalcitonin in early detection of postoperative complications. Dig Surg 15:260–265
Mustard RA Jr, Bohnen JM, Haseeb S, Kasina R (1987) C-reactive protein levels predict postoperative septic complications. Arch Surg 122:69–73
Morley JJ, Kushner I (1982) Serum C-reactive protein levels in disease. Ann N Y Acad Sci 389:406–418
Their M, Ronnholm K, Sairanen H, Holmberg C, Jalanko H (2002) Serum C-reactive protein in pediatric kidney and liver transplant patients. Pediatr Transplant 6:153–160
Wullstein C, Drognitz O, Woeste G, Schareck WD, Bechstein WO, Hopt UT, Benz S (2004) High levels of C-reactive protein after simultaneous pancreas–kidney transplantation predict pancreas graft-related complications and graft survival. Transplantation 77:60–64
Karanjia ND, Corder AP, Bearn P, Heald RJ (1994) Leakage from stapled low anastomosis after total mesorectal excision for carcinoma of the rectum. Br J Surg 81:1224–1226
Law WL, Chu KW (2004) Anterior resection for rectal cancer with mesorectal excision: a prospective evaluation of 622 patients. Ann Surg 240:260–268
Nesbakken A, Nygaard K, Lunde OC, Blucher J, Gjertsen O, Dullerud R (2005) Anastomotic leak following mesorectal excision for rectal cancer: true incidence and diagnostic challenges. Colorectal Dis 7:576–581
Pakkastie TE, Luukkonen PE, Jarvinen HJ (1994) Anastomotic leakage after anterior resection of the rectum. Eur J Surg 160:293–297
Vignali A, Fazio VW, Lavery IC, Milsom JW, Church JM, Hull TL, Strong SA, Oakley JR (1997) Factors associated with the occurrence of leaks in stapled rectal anastomoses: a review of 1,014 patients. J Am Coll Surg 185:105–113
Alberts JC, Parvaiz A, Moran BJ (2003) Predicting risk and diminishing the consequences of anastomotic dehiscence following rectal resection. Colorectal Dis 5:478–482
Nesbakken A, Nygaard K, Lunde OC (2001) Outcome and late functional results after anastomotic leakage following mesorectal excision for rectal cancer. Br J Surg 88:400–404
Yamamoto S, Fujita S, Akasu T, Moriya Y (2004) A comparison of the complication rates between laparoscopic colectomy and laparoscopic low anterior resection. Surg Endosc 18:1447–1451
Millan M, Garcia-Granero E, Flor B, Garcia-Botello S, Lledo S (2006) Early prediction of anastomotic leak in colorectal cancer surgery by intramucosal pH. Dis Colon Rectum 49:595–601
Yentis SM, Soni N, Sheldon J (1995) C-reactive protein as an indicator of resolution of sepsis in the intensive care unit. Intensive Care Med 21:602–605
Claeys R, Vinken S, Spapen H, ver Elst K, Decochez K, Huyghens L, Gorus FK (2002) Plasma procalcitonin and C-reactive protein in acute septic shock: clinical and biological correlates. Crit Care Med 30:757–762
Meisner M, Tschaikowsky K, Hutzler A, Schick C, Schuttler J (1998) Postoperative plasma concentrations of procalcitonin after different types of surgery. Intensive Care Med 24:680–684
Sarbinowski R, Arvidsson S, Tylman M, Öresland T, Bengtsson A (2005) Plasma concentration of procalcitonin and systemic inflammatory response syndrome after colorectal surgery. Acta Anaesthesiol Scand 49:191–196
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Welsch, T., Müller, S.A., Ulrich, A. et al. C-reactive protein as early predictor for infectious postoperative complications in rectal surgery. Int J Colorectal Dis 22, 1499–1507 (2007). https://doi.org/10.1007/s00384-007-0354-3
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00384-007-0354-3