
Abstract
We report a case of pheochromocytoma in the urinary bladder of a 14-year-old girl who presented with headache and palpitation after voiding. This is an extremely rare condition in pediatric age group and thus can be missed easily. This case is the seventh case reported in the reviewed literature.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Extra-adrenal pheochromocytomas are uncommon neoplasm that is found in about 10% in adults and up to 30% in children suffering from pheochromocytomas [1]. Its occurrence in the urinary bladder is even rarer, accounting for less than 0.06% of all bladder tumors and less than 1% of all pheochromocytomas [2, 3]. We report a case of pheochromocytoma of the urinary bladder in a 14-year-old girl, in whom a partial cystectomy was performed.
Case report
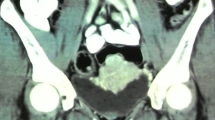
A 14-year-old Chinese girl first presented with a short history of headache and palpitation after voiding, which lasted for 30–60 min. Physical examination and random blood pressure was normal. She was treated as migraine but her symptoms did not improve for 2 years. It was subsequently found that she had intermittent hypertension up to 188/136 mmHg after micturition and an elevated 24-h noradrenaline up to 1,678 nmol. Ultrasonography and magnetic resonance imaging (MRI) showed a 4 × 3 × 3.5 cm well-defined solid lesion in the left posterior aspect of the urinary bladder (Fig. 1). Iodine-131—methyliodobenzylguanidine scintigraphy (I-MIBG) confirmed a solitary lesion of increased uptake in the urinary bladder. The diagnosis of solitary pheochromocytoma of the urinary bladder was made.

MRI pelvis showing the lesion at the posterior wall of the urinary bladder
Her blood pressure was controlled at 120/80 mmHg (for both pre-voiding and post-voiding) with phenoxybenzamine and propanolol 4 weeks before surgery. She underwent cystoscopy followed by open excision of the tumor. At cystoscopy, a 4 cm vascular tumor was found protruding from the left wall of the bladder, just proximal to the trigone and close to the left ureteric orifice. Tumor excision with partial cystectomy without reimplantation was successfully performed though repair of the bladder wall near the distal end of the left ureter was required. Throughout the intraoperative period, blood pressure remained stable with minimal fluctuation. All anti-hypertensive medications were discontinued immediately after the operation. The post-operative recovery was uneventful and the Foley catheter was removed at 2 weeks after the operation. Histopathological examination confirmed the diagnosis of a pheochromocytoma of the urinary bladder. All the resected margins were clear of tumor cells with a focal vascular invasion noted.
At 3-month follow-up there were no any urinary symptoms identified and patient could pass urine up to a volume of 150 ml about 5–6 times per day.
Discussion
Pheochromocytoma of the urinary bladder in children is very rare. On literature review, there are only 7 cases, including our patient, since 1960 [4–6, 11, 12]. Their age ranges from 7 to 14 years. The majority of the tumors were hormonally active (83%) and lead to the characteristic symptoms of headache, palpitation, fainting, diaphoresis and hypertension after micturition. In 4 out of 7 patients, there was a significant delay in making the diagnosis up to 2 years from the onset of the symptoms. This was probably attributed to the rarity of the tumor [2, 5, 10]. On the contrary, as observed in our review, the diagnosis was more readily made, usually within 6 weeks, when patients presented with hematuria.
Preoperative recognition of the tumor is important as patient safety during surgery improves by proper preoperative blood pressure optimization. A high index of suspicion helps an early diagnosis and treatment, which leads to a good outcome. To investigate for suspected cases of pheochromocytoma, it is important to perform either the computed tomography or MRI for anatomical localization of the tumor and the functional scan, I-MIBG, for diagnostic confirmation and for the search for possible metastasis. A sensitivity of almost 100% can be achieved by combining these investigations [7]. This is particularly important in pediatric patients, as pheochromocytomas are more often multifocal and extra-adrenal when compared with adults [8].
The definitive treatment of bladder pheochromocytoma is excision with partial cystectomy. It is worthwhile to have prior cystoscopic examination as this can assess the exact location of the tumor and its relationship to ureters. Depending on the site and size of the tumor, open partial cystectomy with or without reimplantation of the ureter is usually possible though total cystectomy may rarely be needed [11]. In small lesions, there are anecdotal reports of laparoscopic and transurethral resection done in adults [2, 3, 9], suggesting the feasibilities of the minimally invasive approach in selected cases.
All these patients have to be followed up regularly for the bladder function after partial cystectomy as well as the surveillance for recurrence. The blood pressure should be monitored regularly and periodic endocrine and radiological evaluation like I-MIBG and MRI is essential. Life-long follow up is recommended for these patients as recurrence or metastasis cannot be predicted on the histology alone.
Bladder pheochromocytoma is a very rare tumor in children. We need to have a high index of suspicion to allow early diagnosis and treatment. A good outcome is usually observed in properly treated patients.
References
Whalen RK, Althausen AF, Daniels GH (1992) Extra-adrenal pheochromocytoma. J Urol 147:1–10
Doran F, Yarinli S, Bayazit Y (2002) Pheochromocytoma of the urinary bladder. APMIS 110:733–736
Onishi T, Sakata Y, Yonemura S (2003) Pheochromocytoma of the urinary bladder without typical symptoms. Int J Urol 10:398–400
Pinto KJ, Jerkins GR (1997) Bladder pheochromocytoma in a 10-year-old girl. J Urol 158:583–584
Kazzi GB (2000) Asymptomatic bladder phaeochromocytoma in a 7-year-old boy. J Paediatr Child Health 37:600–602
Naqiyah I, Rohaizak M, Meah FA (2005) Phaeochromocytoma of the urinary bladder. Singapore Med J 46(7):344–346
Guller U, Turek J, Eubanks S (2006) Detecting pheochromocytoma: defining the most sensitive test. Ann Surg 243(1):102–107
Ross JH (2000) Pheochromocytoma. Special considerations in children. Urol Clin North Am 27:393–402
Kozlowski PM, Mihm F (2001) Laparoscopic management of bladder pheochromocytoma. Urology 57:365
Meyer JJ, Sane SM, Drake RM (1979) Pheochromocytoma of the urinary bladder: report of a case and review of the literature. Pediatrics 63(6):879–885
Scott WW, Eversole SL (1960) Pheochromocytoma of the urinary bladder. J Urol 83:656
Higgins PM, Tresidder GC (1966) Pheochromocytoma of the urinary bladder. Br Med J 2:274
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Mou, J.W.C., Lee, K.H., Tam, Y.H. et al. Urinary bladder pheochromocytoma, an extremely rare tumor in children: case report and review of the literature. Pediatr Surg Int 24, 479–480 (2008). https://doi.org/10.1007/s00383-007-2013-8
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00383-007-2013-8