
Abstract
Background
Deficiency of vitamin K predisposes to early, classic, or late vitamin K deficiency bleeding (VKDB), of which late VKDB may be associated with serious and life-threatening intracranial bleeding. Late VKDB is characterized with intracranial bleeding in infants aged 2–24 weeks due to severe vitamin K deficiency, occurring primarily in exclusively breast-fed infants. Late VKDB is still an important cause of mortality and morbidity in developing countries.
Materials and methods
We presented 120 cases of late VKDB, which were evaluated at Erciyes University Medical Faculty Hospital between June 1990 and June 2006.
Results
Signs and symptoms of the patients were bulging fontanels (70%); irritabilities (50%); convulsions (49%); bleeding and ecchymosis (47%); feeding intolerance, poor sucking, and vomiting (46%); diarrhea (34%); jaundice (11%); and pallor (9%), and among these infants, 21% received medication before the diagnosis (10%, antibiotics; 3%, simethicone; 4%, paracetamol; and 4%, phenobarbital). Intracranial hemorrhage in 88 (73%) patients has been observed. The hemorrhage was subdural in 34 (28%) cases, intracerebral in 28 (23%), subarachnoid in 17 (14%), intraventricular in 9 (8%), intracerebral and subdural in 12 (10%), subdural and subarachnoid in 6 (5%), and combination of intracerebral, subdural, and intraventricular in 14 (12%), and the mortality rate was 31%.
Conclusion
Although late VKDB leads to significant morbidity and mortality, it can be avoided by providing vitamin K prophylaxis to all newborns. Administration of vitamin K (1 mg) at birth can prevent intracranial bleeding and other hemorrhagic manifestations.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Vitamin K is a fat-soluble vitamin that is necessary for the synthesis of functional molecules of factors II, VII, IX, and X by the liver. Vitamin K level in the newborn is usually low due to insufficient vitamin K stores, and vitamin K poorly transfers in the placenta from mother to infant and is present only in very low concentrations in human milk. Thus, it is not surprising that the newborn infant suffer from undetectable vitamin K serum levels with abnormal amounts of the coagulation proteins and undercarboxylated prothrombin. Breast-fed infants cannot receive the recommended vitamin K intake via human milk. In addition, the intestinal flora of the breast-fed infant may produce less vitamin K than the flora of the formula-fed infant [1–3].
Vitamin K deficiency bleeding (VKDB) has three distinct patterns of presentation. Early VKDB is seen within 24 h of birth in infants whose mothers have been on anticonvulsant or antituberculous drugs during pregnancy. Classic VKDB occurs between the second and seventh days of life with most of the cases being idiopathic. Late VKDB is characterized by bleeding in infants between day 8 to 6 months of life due to severe vitamin K deficiency, occurring primarily in exclusively breast-fed infants. It has a peak incidence between 3 and 8 weeks [1–3]. A major feature of late VKDB from the classical syndrome is a much higher incidence of intracranial hemorrhage (ICH), often as the first presenting sign [1–3]. ICH originating from VKDB can be more seen rather than other factor deficiency [4].
Considering the alarming nature of the clinical manifestation, the morbidity and mortality can be indirectly estimated from referral centers, while the exact incidence of VKDB is observed only in an elaborate population-based study. There are few case reports available on this aspect from the region [3, 5–26]. Herein, we present 120 cases of late VKDB, observed at Erciyes University Medical Faculty Hospital between June 1990 and June 2006.
Patients and methods
In this retrospective study, charts of children with late VKDB were evaluated. Details regarding pregnancy and delivery, type of feeding, timing of presentation, signs and symptoms, bleeding sites, underlying illness in the baby, laboratory assays, management, and outcome were recorded. All infants who were older than 1 week and admitted in the pediatric ward of Erciyes University, with a diagnosis of late vitamin K deficiency bleeding from June 1990 to June 2006, were evaluated.
The diagnostic criteria of late VKDB were established as the bleeding in an infant after 7 days of life with (a) normal levels of fibrinogen and platelet count, (b) prothrombin time (PT) and activated partial thromboplastin time (aPTT) prolonged initially but returned to normal level after vitamin K administration, and (c) if fresh frozen plasma was also administered, seventh day PT and aPTT control must be normal to exclude the effect of transfused factors.
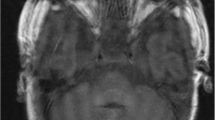
Laboratory studies included a complete blood count; liver function test [aspartate aminotransferase (AST), alanine aminotransferase (ALT), alkaline phosphatase] and urine analysis were also performed. Cranial tomography and/or magnetic resonance imaging was performed in all cases suspected with ICH. All cases were evaluated for expected complication for ICH, while during follow-up period, psychomotor assessments and neurological examinations were done in all patients. Postmortem liver biopsy was done at 17 infants who died.
Results
Of 120 infants who fulfilled the diagnostic criteria of late VKDB, 83 (69%) were males and 37 (31%) were females. Eighty-one cases who were delivered in the hospital received 1 mg of vitamin K intramuscularly (IM) shortly after delivery, as is routine practice in Turkey. The rest were delivered at home and did not receive any vitamin K prophylaxis. The age at presentation ranged between 1 and 12 weeks.
There were 7 (6%) babies, ages between 8 and 14 days, 25 (21%) cases between 15 and 30 days, 43 (36%) between 31 and 45 days, 21(17%) between 46 and 60 days, 13 (11%) between 61 and 90 days, and 11 (9%) between 91 and 240 days. All children except 3% were breast-fed infants (Table 1).
Signs and symptoms of the patients were bulging fontanels (70%); irritability (50%); convulsions (49%); bleeding and ecchymosis (47%); feeding intolerance, poor sucking, and vomiting (46%); diarrhea (34%); jaundice (11%), and pallor (9%) (Table 2). Among these infants, 21% had received medications (10%, antibiotics; 3%, simethicone; 4%, paracetamol; and 4%, phenobarbital).
There was ICH in 88 (73%) patients. The percentage of subdural hemorrhage (SDH), intracerebral hemorrhage (ICEH), subarachnoid hemorrhage (SAH), and intraventricular hemorrhage (IVH) were 28%, 23%, 14%, and 8%, respectively. The combinations of ICEH and SDH, SDH and SAH, and ICEH and SDH and IVH were seen at 10%, 5%, and 12%, respectively (Table 3). The mortality rate of ICH was 31%.
Liver biopsy revealed six idiopathic neonatal hepatitis (two of them were due to cytomegalovirus infection), and biliary atresia was found in three cases. Other liver biopsies were normal. At the time of admission, AST and ALT levels were high in only 10% of the cases. Before treatment, PT and aPTT levels in all cases were higher than normal. After administration of vitamin K, PT and aPTT levels became normal in all cases. Of the patients, 52% had neurological sequelae, 18% well, and 30% out of control after discharge.
Discussion
VKDB caused by vitamin K deficiency has been recognized as an important cause of morbidity and mortality. It was formerly called as “hemorrhagic disease of newborn,” but this term has been discarded as the etiological basis is solely due to vitamin K deficiency and to include those infants who develop VKDB beyond the usually defined 4-week neonatal period. VKDB is one of the most common causes of acquired hemostatic disorder in early infancy.
The history of VKDB is littered with clouds of uncertainties and controversies on the extent of the problem in public health that still persist to the present [3]. In 1992, Golding et al. [27] reported an unexpected association between IM vitamin K prophylaxis in the neonatal period and later childhood cancer. Although unconfirmed, the report caused considerable concern worldwide and prompted changes in national prophylaxis policies in several countries [5]. Cornelissen et al. [5] compared and evaluated three basic strategies for vitamin K prophylaxis for healthy newborns in four countries. These strategies were (1) daily supplementation of low-dose vitamin K for breast-fed infants (the Netherlands), (2) 1 mg orally [Australia (January 1993 ± March 1994) and Germany (December 1992 ± December 1994)], (3) 1 mg vitamin K IM (Australia since March 1994), and finally (4) 2 × 2 mg vitamin K (new mixed micellar preparation) (Switzerland). From their report, it had been underlined that the failure rates for complete prophylaxis only were: strategies (1) 0 (0 ± 0.7) in the Netherlands, (2) 1.8 (1.1 ± 2.8) in Germany and 1.5 (0.5 ± 3.6) in Australia, (3) 0 (0 ± 0.9) in Australia (IM), and (4) 1.2 (0 ± 6.5) in Switzerland [5]. The compliance of prophylactic regimen in Turkey does not seem to be satisfactory, so we advise a repetitive IM dose of vitamin K especially for breast-fed infants. Although it is not evidence-based, we believe that it may reduce the high mortality rates in our country.
The low concentration of vitamin K in human breast milk and the predisposition to vitamin K deficiency bleeding following exclusive breast feeding are emerging as a matter of concern especially in developing countries where exclusive breast feeding is vigorously advocated to promote optimal health in the infant. Late VKDB, an important cause of morbidity and mortality, manifests after the second week of life and is particularly associated with intracranial hemorrhage. The rate of late VKDB ranges from 4.4 to 7.2 cases per 100,000 births, based on reports from Europe and Asia [1–3, 5, 16–25]. In developed countries, VKDB is now a rare life-threatening disease due to the widespread use of effective prophylaxis with vitamin K at birth [1–3, 5, 20, 21]. The postnatal administration of vitamin K has dramatically reduced the incidence of vitamin K deficiency bleeding during the first weeks of life, although sporadic cases with late-onset hemorrhage are described among exclusively breast-fed infants who did not receive additional prophylaxis. Routine vitamin K prophylaxis at birth declined the incidence of late VKDB from 7/100,000 to 1.1/100,000 live births in the Netherlands [5].
Intracranial hemorrhage can be a presenting manifestation of late VKDB in children leading to death in some cases and neurological sequelae in the survivors. Almost two thirds of the babies with late VKDB present with serious intracranial bleeding lead to high morbidity and subsequent mortality [1–3]. In a study performed in Turkey, neurologic findings were found in 73% of the patients and mortality was 33% [12]. Similarly, 10 out of 30 patients (mortality rate was 33%) died in another study [14]. Still another study including 14 cases in India showed that 88% of the cases had intracranial bleeding and mortality rate was 57% [24]. Also in another review of 108 cases of late VKDB from Germany, 58% had intracranial hemorrhage with a mortality rate of 19% and neurological sequel in 21% [10]. A prospective study being conducted for over 2 years in the British Isles revealed that 10 out of the 27 infants had intracranial hemorrhage, which two of them with intracranial bleed later died [20]. The same group recently reported that the incidence of VKDB had decreased about one third that was detected in the two earlier studies; however, late-onset VKDB remains virtually confined [21]. On the other hand, in our 120 cases, intracranial hemorrhage was determined in 88%, and the mortality rate in these patients was 31%.
Pooni et al. [25] demonstrated that SDH was the most common type of intracranial hemorrhage reported, followed by SAH. Martín-López et al. [18] found that the majority of the patients showed hemorrhage at more than one site (75%). The reported percentages of hemorrhage were ICEH in 67% of the cases, followed by SDH and SAH in 57% and 46% of the cases, respectively. Shearer [3] reported ICEH, 44%; ICEH + IVH, 22%; SAH, 11%; and other sites. In our study, the hemorrhage was SDH in 28% of the cases followed by ICH, SAH, and IVH in 23%, 14%, and 8% of the cases, respectively. In addition, the hemorrhage was ICH + SDH, 10% and SDH + SAH, 5% in two sites.
The breast feeding and no vitamin K prophylaxis at birth were reported as the most common causes of late VKDB in previous studies. In a Malaysian study, 76% of 42 patients with late VKDB had breast feeding and 81% of the patients were delivered at home [24]. Our results were similar to previous reports. We have presented 120 patients with late VKDB. All children with late VKDB were breast-fed infants except for three patients.
Eighty-one cases who were delivered at the hospital received 1 mg of vitamin K intramuscularly shortly after delivery. The rest were delivered at home and did not receive any vitamin K prophylaxis. In recent years, the ratio of administration of prophylactic vitamin K in Turkey was increased; the ratio of not receiving vitamin K seems to be relatively high in our group. We speculated that this high ratio can be originated from the previously enrolled patients. Intramuscular administration of 1 mg vitamin K is a standard care in Turkey, but as supposed it can be neglected, especially with home deliveries. The number of home deliveries is decreasing; in inverse proportions, the incidence of cesarean delivery is increasing in Turkey as worldwide. Despite the World Health Organization recommendation that cesarean section rates should not be higher than 10% to 15% [28], the cesarean rate is continuously increasing in Turkey, from 6.9% in 1993, to 14.0% in 1998, to 21.2% in 2003, and progressively to 36.7% in 2008 [29].
Late VKDB may be primary or secondary to cystic fibrosis, biliary atresia, alfa 1 antitrypsin deficiency, hepatitis, abetalipoproteinemia, celiac disease, or chronic warfarin exposure [1–3]. Liver biopsy revealed six idiopathic neonatal hepatitis and biliary atresia in three cases.
Newborns have only 20–50% of adult coagulation activity. Lack of vitamin K administration at birth, exclusive breast feeding, chronic diarrhea, and prolonged use of antibiotics make them more prone to vitamin K deficiency bleeding. In our study, 34% of the infants had diarrhea, and 21% had received medications.
The recommendation of the American Academy of Pediatrics is to give vitamin K to all newborns as a single intramuscular dose of 0.5 to 1.0 mg [13]. The standard manner of vitamin K administration in Turkey is 1 mg intramuscular vitamin K administration at birth. We think that the prophylaxis of vitamin K may be neglected in home-birth infants, especially at rural area.
In summary, this study evaluated the prognosis and clinical features of infants with late-type VKDB based on the data collected during a 16-year period. Our results underline that late-type VKDB is still one of the remarkable problems of today and may initially accompany with catastrophic ICH. Therefore, physicians should be aware of the importance of early use of vitamin K when necessary, and an attempt should be made to provide this to infants not only in hospitals but also to those born at home in rural areas. The compliance of prophylactic regimen in Turkey does not seem to be satisfactory, so we vigorously emphasize that an additional IM dose of vitamin K especially for breast-fed infants may reduce the high mortality and morbidity rates associated with VKDB in our country.
References
Palis J, Segel GB (2010) Hematology of the fetus and newborn. In: Kaushansky K, Lichtman MA, Beutler E, Kipps TJ, Seligohn U, Prchal JT (eds) Williams hematology. McGraw-Hill, New York, pp 87–104
Cantor AB (2009) Developmental hemostasis: relevance to newborns and infants. In: Orkin SH, Nathan DG, Ginsburg D (eds) Hematology of infancy and childhood, 7th edn. Saunders, Philadelphia, pp 147–191
Shearer MJ (2009) Vitamin K deficiency bleeding (VKDB) in early infancy. Blood Rev 23:49–59
Patiroglu T, Ozdemir MA, Unal E et al (2011) Intracranial hemorrhage in children with congenital factor deficiencies. Childs Nerv Syst. doi:10.1007/s00381-011-1519-5, PubMed PMID: 21748400
Cornelissen M, von Kries R, Loughnan P, Schubiger G (1997) Prevention of vitamin K deficiency bleeding: efficacy of different multiple oral dose schedules of vitamin K. Eur J Pediatr 156:126–130
Cekinmez M, Cemil T, Cekinmez EK, Altinörs N (2008) Intracranial hemorrhages due to late-type vitamin K deficiency bleeding. Childs Nerv Syst 24:821–825
Zengin E, Sarper N, Türker G, Corapçioğlu F, Etuş V (2006) Late haemorrhagic disease of the newborn. Ann Trop Paediatr 26:225–231
Per H, Kumandaş S, Ozdemir MA, Gümüş H, Karakukcu M (2006) Intracranial hemorrhage due to late hemorrhagic disease in two siblings. J Emerg Med 31:49–52
Yilmaz C, Yuca SA, Yilmaz N, Bektaş MS, Caksen H (2009) Intracranial hemorrhage due to vitamin K deficiency in infants: a clinical study. Int J Neurosci 119:2250–2256
Sutor AH, Dagres N, Niederhoff H (1995) Late form of vitamin K deficiency bleeding in Germany. Klin Padiatr 207:89–97
Uluşahin N, Arsan S, Ertogan F (1996) Effects of oral and intramuscular vitamin K prophylaxis on PIVKA-II assay parameters in breastfed infants in Turkey. Turk J Pediatr 38:295–300
Bor O, Akgun N, Yakut A, Sarhus F, Kose S (2000) Late hemorrhagic disease of the newborn. Pediatr Int 42:64–66
Pirinccioglu AG, Gurkan F, Bosnak M, Acemoglu H, Davutoglu M (2011) Intracranial hemorrhage: clinical and demographic features of patients with late hemorrhagic disease. Pediatr Int 53:68–71
Demirören K, Yavuz H, Cam L (2004) Intracranial hemorrhage due to vitamin K deficiency after the newborn period. Pediatr Hematol Oncol 21:585–592
Doneray H, Tan H, Buyukavci M, Karakelleoglu C (2007) Late vitamin K deficiency bleeding: 16 cases reviewed. Blood Coagul Fibrinolysis 18:529–530
Takahashi D, Shirahata A, Itoh S, Takahashi Y, Nishiguchi T, Matsuda Y (2011) Vitamin K prophylaxis and late vitamin K deficiency bleeding in infants: the 5th nation-wide survey in Japan. Pediatr Int. doi:10.1111/j.1442-200X.2011.03392.x.
Visser DY, Jansen NJ, Ijland MM, de Koning TJ, van Hasselt PM (2011) Intracranial bleeding due to vitamin K deficiency: advantages of using a pediatric intensive care registry. Intensive Care Med 37:1014–1020
Martín-López JE, Carlos-Gil AM, Rodríguez-López R, Villegas-Portero R, Luque-Romero L, Flores-Moreno S (2011) Prophylactic vitamin K for vitamin K deficiency bleeding of the newborn. Farm Hosp 35:148–155
Kasatkar P, Shetty S, Ghosh K (2010) Delayed vitamin K deficiency as a cause of bleeding: still a concern in the 21st century! Blood Coagul Fibrinolysis 21:608–610
McNinch AW, Tripp JH (1991) Haemorrhagic disease of the newborn in the British Isles: two year prospective study. BMJ 303:1105–1109
McNinch A, Busfield A, Tripp J (2007) Vitamin K deficiency bleeding in Great Britain and Ireland: British Paediatric Surveillance Unit Surveys, 1993–94 and 2001–02. Arch Dis Child 92:759–766
American Academy of Pediatrics Committee on Fetus and Newborn (2003) Controversies concerning vitamin K and the newborn. American Academy of Pediatrics Committee on Fetus and Newborn. Pediatrics 112:191–192
Danielsson N, Hoa DP, Thang NV, Vos T, Loughnan PM (2004) Intracranial haemorrhage due to late onset vitamin K deficiency bleeding in Hanoi province, Vietnam. Arch Dis Child Fetal Neonatal Ed 89:F546–F550
Pooni PA, Singh D, Singh H, Jain BK (2003) Intracranial hemorrhage in late hemorrhagic disease of the newborn. Indian Pediatr 40:243–248
Choo KE, Tan KK, Chuah SP, Ariffin WA, Gururaj A (1994) Haemorrhagic disease in newborn and older infants: a study in hospitalized children in Kelantan, Malaysia. Ann Trop Paediatr 14:231–237
Zidan AS, Abdel-Hady H (2011) Surgical evacuation of neonatal intracranial hemorrhage due to vitamin K deficiency bleeding. J Neurosurg Pediatr 7:295–299
Golding J, Greenwood R, Birmingham K, Mott M (1992) Childhood cancer, intramuscular vitamin K, and pethidine given during labour. BMJ 305:341–346
World Health Organization (1985) Appropriate technology for birth. Lancet 2:436–437
Turkey Demographic and Health Survey-2008 (internet): Hacettepe Institute of Population Studies, Ministry of Health, 2008. Available at http://www.hips.hacettepe.edu.tr/tnsa2008/index.htm
Conflicts of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ozdemir, M.A., Karakukcu, M., Per, H. et al. Late-type vitamin K deficiency bleeding: experience from 120 patients. Childs Nerv Syst 28, 247–251 (2012). https://doi.org/10.1007/s00381-011-1575-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00381-011-1575-x