
Abstract
Introduction
Information about pediatric survivors of brain tumors in developing countries is scant.
Purpose
In this study, we aimed to investigate the availability of resources for treatment and long-term follow-up of children with central nervous system tumors in developing countries.
Materials and methods
A web-based questionnaire on available services and follow-up of brain tumor survivors was posted at www.cure4kids.org, and registered users were invited to participate.
Results
A total of 140 evaluable responses from developing countries (n = 103) and high-income countries (n = 37) were obtained. There was a significant correlation between gross national income and the availability of services for treatment and follow-up and between patient load and the availability of some services.
Conclusion
The resources for treatment and long-term follow-up of children with brain tumors need to be improved in developing countries.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
In developed countries, many children with brain tumors survive [18] with risk of complications; so, dedicated follow-up programs have been implemented [3, 7]. Only limited data on incidence [9, 10] and survival [1, 17] for children with brain tumors in developing countries (DCs) are available, and none is available on long-term follow-up (LTFU).
As seen in other malignancies [5], there may be significant differences among DCs in resource availability and outcome related to their degree of development. Therefore, after the publication of a survey from the Children's Oncology Group (COG) depicting the situation in North America [4], we investigated the availability of resources for treatment and LTFU of children with CNS tumors in DCs.
Methods
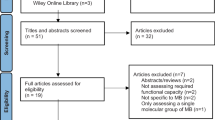
A questionnaire based on a survey conducted at the COG [4] was posted on Oncopedia, a pediatric oncology education cases and discussion forum at the www.cure4kids.org website used by over 4,000 health professionals. A link to the full text publication of the results of the COG survey was provided. This survey was available for 1 month, and two invitations were sent to cure4kids users via email. Only one response was evaluated from each participating center.
Countries were classified as per the World Bank into: low-, middle-, and high-income countries (LICs, MICs, and HICs). MICs are further divided into low or upper middle-income countries (LMICs and UMICs). For comparison with the COG and HIC institutions, LICs and MICs were grouped as DCs. For comparison among DCs, we grouped LICs and LMICs (and this group is referred to as L-LMICs) and compared them with UMICs.
Contingency tables were constructed, chi-square or Fisher exact tests were used for categorical variables, and the Mann–Whitney test was used for continuous variables. The p values lower than 0.05 were considered significant.
Results
Characteristics of responding centers
A total of 151 users returned the survey. Eleven responses were excluded due to duplication; therefore, a total of 140 surveys were evaluable including LICs (n = 6; Asia = 5, Africa = 1), LMICs (n = 39; Asia = 26, Central America = 5, South America = 4, and Africa = 4), UMICs (n = 58; South America = 28, Central America and Mexico = 16, Asia = 7, Europe = 5, and Africa = 2), and HICs (n = 37; Europe = 12, USA = 13, Arabian Gulf = 5, Australia = 3, Israel = 2, and Canada = 2).
Comparison among different groups according to yearly patient load
Centers from DCs had a significantly higher load of pediatric oncology patients than those of the COG survey (Table 1). However, there were no significant differences in the size of their neuro-oncology programs. The same was true among the DC group centers (Table 2).
Available resources for treatment of pediatric brain tumors
Children in DC centers had less access to a dedicated team and disease-specific guidelines for brain tumors (Table 1). Within the DC group, children in UMICs had greater access to such resources (Table 2).
Interestingly, within DCs, the number of patients with brain tumors treated per year positively influenced the availability of a dedicated team (20/61 in centers seeing <15 patients/year and 28/42 in centers seeing ≥15 patients/year, p < 0.001) and disease-specific guidelines (36/61 in centers seeing <15 patients/year and 35/42 in centers seeing ≥15 patients/year, p = 0.004).
Programs for long-term follow-up of pediatric brain tumor patients
A dedicated LTFU team was significantly less available in DCs compared to HICs (Table 1). However, there were no significant differences among UMICs and L-LMICs (Table 2). Children and survivors over 21 years from DCs were less likely to be followed up by a dedicated neuro-oncology follow-up program than were those treated at centers in HICs responding to our survey (Table 1).
Resources for long-term follow-up of pediatric brain tumor patients
Only a minority of institutions in LICs were able to offer formal neuropsychological evaluation at the time of school entry or >2 years after radiotherapy. The availability of this service correlated significantly with the presence of a dedicated neuro-oncology team (p = 0.02), but no correlation was found with the size of the program or the country's economical classification within the DC subgroup (Table 1).
Routine growth hormone (GH) replacement was offered significantly less frequently at centers in DCs compared to HICs (Table 1) and in fewer L-LMICs compared to UMICs (Table 2). Moreover, in 16 out of 63 centers from DCs where GH was available, the cost of the drug must be covered by the affected families or foundations, so not all patients have access to it.
Perceived barriers to follow-up of childhood brain tumor survivors
The perceived barriers (i.e., limited access or lack of insurance, lack of funding or dedicated time for survivors, patient's uncertainties, patient's desire, inability to locate adult survivors) did not differ significantly between countries' subgroups, but the inability to locate survivors was significantly perceived more frequently as a barrier in our survey compared to the COG study (p < 0.001). However, there were no significant differences when compared to the group from HIC that completed our survey.
Discussion
Differences in treatment resources between DCs and HICs or COG institutions included a significantly lower availability of a dedicated neuro-oncology team and disease-specific treatment guidelines in DCs. There were also differences among the different subgroups of DCs, since UMICs were significantly more likely to have treatment guidelines and a trend for a dedicated neuro-oncology program compared to L-LMICs.
Indicators of country development play a critical role in childhood cancer survival [5, 12, 19], and even though we have not assessed survival in our study, the limited availability of treatment resources found in our study may indicate a worse survival in DCs. Centers in DCs had a significantly higher patient load than centers in HICs and than COG centers. An interesting finding in our study is the positive impact of patients' load on some of the services available for children with brain tumors. Although income classification of the country influenced the availability of disease-specific treatment guidelines in DCs, such impact of income could be ameliorated by the development of large supraregional neuro-oncology programs in DCs. It is indeed important to treat pediatric brain tumors in specialized units because these children require special neurosurgical [2], neuroradiological [16], neuropathological [8], and radiation oncology [6] expertise. Such expertise is affected by the number of patients treated [6, 16]. Concentrating care in large centers has the advantages of cost effectiveness, comprehensive care, enough patient number to create disease-specific subspecialties, and many other benefits. On the other hand, such concentration may deprive underserved populations who cannot reach such centers due to distance, transportation, or financial obstacles [15]. Therefore, consideration in DCs for housing, transportation, and financial coverage should be considered when establishing specialized cancer centers or units to provide equal opportunity for all patients to be treated at these centers.
However, even in centers with more than 15 children with brain tumors a year, disease-specific guidelines were not available in half of the cases. Different studies have documented the positive impact of place of treatment and use of standard treatment guidelines on cancer survival in children [6, 11, 14]. Also, Ribeiro et al. [19] showed that a subgroup of DCs could improve childhood cancer survival through concentrated pediatric oncology units, creating local support, and other strategies. Twinning initiatives that proved successful for leukemias and other solid tumors may be implemented to improve the care that children with CNS tumors receive worldwide [13].
There is an increasing interest from different groups like the Society of Neuro-oncology to encourage twinning initiatives for brain tumors in DCs. Our study provides baseline data that may help guide such efforts more effectively.
Our study also detected significant differences in the availability of LTFU resources for survivors of brain tumors in DCs. DCs were significantly less likely to have LTFU services, a dedicated LTFU by a neuro-oncology service, and LTFU after reaching 21 years old compared to their counterparts in HICs. The same was also true for availability of neuropsychological testing and GH. Treatment of children with CNS tumors is associated to long-term sequelae such as GH deficiencies as well as neuropsychological deficits [3, 7], and efforts to improve the adequate care of survivors should be encouraged. We also found that the inability to locate survivors was perceived as a more important barrier for the follow-up of survivors in our setting. Affected families become lost to follow-up more frequently in DCs as reported for other tumors [5].
Though collected through an innovative resource, our results have limitations. Procurement of data from DCs is limited by the lack of national data, cooperative groups, and national registries [13, 19]. Even though our website has a global outreach, some areas of the world that have stronger links to the St. Jude Children's Research Hospital International Outreach Program might have been overrepresented. Participation in the survey did not imply that the responses were the official data from each institution, and there may be inaccuracies in the responses. Therefore, surveying professionals related to pediatric oncology from DCs using dedicated websites like Oncopedia may be considered as an alternative to procure data from DCs that are difficult to obtain by other ways.
References
Akyuz C, Varan A, Kupeli S, Akalan N, Soylemezoglu F, Zorlu F, Kutluk T, Buyukpamukcu M (2008) Medulloblastoma in children: a 32-year experience from a single institution. J Neurooncol 90:99–103
Albright AL, Sposto R, Holmes E, Zeltzer PM, Finlay JL, Wisoff JH, Berger MS, Packer RJ, Pollack IF (2000) Correlation of neurosurgical subspecialization with outcomes in children with malignant brain tumors. Neurosurgery 47:879–885, Discussion, 885–877
Armstrong GT, Liu Q, Yasui Y, Huang S, Ness KK, Leisenring W, Hudson MM, Donaldson SS, King AA, Stovall M, Krull KR, Robison LL, Packer RJ (2009) Long-term outcomes among adult survivors of childhood central nervous system malignancies in the Childhood Cancer Survivor Study. J Natl Cancer Inst 101:946–958
Bowers DC, Adhikari S, El-Khashab YM, Gargan L, Oeffinger KC (2009) Survey of long-term follow-up programs in the United States for survivors of childhood brain tumors. Pediatr Blood Cancer 53:1295–1301
Canturk S, Qaddoumi I, Khetan V, Ma Z, Furmanchuk A, Antoneli CB, Sultan I, Kebudi R, Sharma T, Rodriguez-Galindo C, Abramson DH, Chantada GL (2010) Survival of retinoblastoma in less-developed countries impact of socioeconomic and health-related indicators. Br J Ophthalmol 94:1432–1436
Danjoux CE, Jenkin RD, McLaughlin J, Grimard L, Gaspar LE, Dar AR, Fisher B, Whitton AC, Kraus V, Springer CD et al (1996) Childhood medulloblastoma in Ontario, 1977–1987: population-based results. Med Pediatr Oncol 26:1–9
Ellenberg L, Liu Q, Gioia G, Yasui Y, Packer RJ, Mertens A, Donaldson SS, Stovall M, Kadan-Lottick N, Armstrong G, Robison LL, Zeltzer LK (2009) Neurocognitive status in long-term survivors of childhood CNS malignancies: a report from the Childhood Cancer Survivor Study. Neuropsychology 23:705–717
Fouladi M, Hunt DL, Pollack IF, Dueckers G, Burger PC, Becker LE, Yates AJ, Gilles FH, Davis RL, Boyett JM, Finlay JL (2003) Outcome of children with centrally reviewed low-grade gliomas treated with chemotherapy with or without radiotherapy on Children's Cancer Group high-grade glioma study CCG-945. Cancer 98:1243–1252
Kadri H, Mawla AA, Murad L (2005) Incidence of childhood brain tumors in Syria (1993–2002). Pediatr Neurosurg 41:173–177
Karkouri M, Zafad S, Khattab M, Benjaafar N, El Kacemi H, Sefiani S, Kettani F, Dey S, Soliman AS (2010) Epidemiologic profile of pediatric brain tumors in Morocco. Childs Nerv Syst 26(8):1021–1027
Kramer S, Meadows AT, Pastore G, Jarrett P, Bruce D (1984) Influence of place of treatment on diagnosis, treatment, and survival in three pediatric solid tumors. J Clin Oncol 2:917–923
Masera G (2008) Income matters: reducing the mortality gap. Lancet Oncol 9(8):703–704
Masera G, Baez F, Biondi A, Cavalli F, Conter V, Flores A, Fontana G, Fossati Bellani F, Lanfranco P, Malta A, Mendez G, Ocampo E, Pacheco C, Riva L, Sala A, Silva F, Sessa C, Tognoni G (1998) North-South twinning in paediatric haemato-oncology: the La Mascota programme, Nicaragua. Lancet 352:1923–1926
Meadows AT, Kramer S, Hopson R, Lustbader E, Jarrett P, Evans AE (1983) Survival in childhood acute lymphocytic leukemia: effect of protocol and place of treatment. Cancer Invest 1:49–55
Onega T, Duell EJ, Shi X, Wang D, Demidenko E, Goodman D (2008) Geographic access to cancer care in the U.S. Cancer 112:909–918
Packer RJ, Gajjar A, Vezina G, Rorke-Adams L, Burger PC, Robertson PL, Bayer L, LaFond D, Donahue BR, Marymont MH, Muraszko K, Langston J, Sposto R (2006) Phase III study of craniospinal radiation therapy followed by adjuvant chemotherapy for newly diagnosed average-risk medulloblastoma. J Clin Oncol 24:4202–4208
Qaddoumi I, Musharbash A, Elayyan M, Mansour A, Al-Hussaini M, Drake J, Swaidan M, Bartels U, Bouffet E (2008) Closing the survival gap: implementation of medulloblastoma protocols in a low-income country through a twinning program. Int J Cancer 122:1203–1206
Qaddoumi I, Sultan I, Gajjar A (2009) Outcome and prognostic features in pediatric gliomas: a review of 6212 cases from the Surveillance, Epidemiology, and End Results database. Cancer 115:5761–5770
Ribeiro RC R, Steliarova-Foucher E, Magrath I, Lemerle J, Eden T, Forget C, Mortara I, Tabah-Fisch I, Divino JJ, Miklavec T, Howard SC, Cavalli F (2008) Baseline status of paediatric oncology care in ten low-income or mid-income countries receiving My Child Matters support: a descriptive study. Lancet Oncol 9(8):721–729
Acknowledgments
The authors wish to acknowledge Dorothy May and Jay Knight from the St. Jude Children's Research Hospital for their technical support.
Conflict of interest
There is no conflict of interest to report from any author.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Qaddoumi, I., Unal, E., Diez, B. et al. Web-based survey of resources for treatment and long-term follow-up for children with brain tumors in developing countries. Childs Nerv Syst 27, 1957–1961 (2011). https://doi.org/10.1007/s00381-011-1479-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00381-011-1479-9