
Abstract
Objectives
To evaluate the effect of preoperative ureteral stenting duration on the outcomes of retrograde intrarenal surgery (RIRS).
Patients and methods
We reviewed our database of patients who underwent RIRS between May 2011 and April 2017 at our institution. The patients were divided into three groups according to preoperative ureteral stenting duration: group 1: no stenting, group 2: short preoperative stenting (< 7 days) and group 3: long preoperative stenting (≥ 7 days). We compared the rate of ureteral injury, other perioperative complications, ureteral dilation and readmission, stone-free rate (SFR) and operative time among the groups.
Results
A total of 560 patients (215 in group 1, 177 in group 2 and 168 in group 3) were included in this study. The mean of maximum stone size was 13.1 (± 6.2) mm, the mean number of stones was 2.3 (± 1.9) and preoperative ureteral stenting duration was 7.2 (± 3.7) days. There were no significant differences in operative time (75.6, 78.5 and 82.4 min, p = 0.280), SFR (79.1, 84.2 and 81.0%, p = 0.433), ureteral injury rate (7.0, 5.1 and 2.4%, p = 0.123) and other perioperative complication rates (12.1, 6.8 and 6.0%, p = 0.061). The only one case of grade IV ureteral injury occurred in group 1 and the rate of ureteral dilation was significantly higher than in group 2 and 3 (14.9, 5.7 and 6.0%, p < 0.001).
Conclusion
Although preoperative ureteral stenting duration has no significant effect on operative outcomes, it is an effective procedure for reducing the rate of intraoperative ureteral balloon dilation and preventing high-grade ureteral injuries.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The prevalence of kidney stone is increasing and is seen up to 14% within a lifetime [12]. Extracorporeal shock wave lithotripsy (ESWL) and retrograde intrarenal surgery (RIRS) are recommended in the treatment of stones between 1 and 2 cm according to the European Association of Urology (EAU) guidelines [19]. Percutaneous nephrolithotomy (PNL) is the traditional treatment recommended for renal stones larger than 2 cm and has a stone-free rate comparable to that of the RIRS method for upper calyceal renal stones between 1 and 2 cm. The SFR after one session of PNL was 91.2%, which was significantly higher than after one session of RIRS for renal stones ranging from 2 to 4 cm in diameter [14]. However, this is a more invasive procedure and has a higher complication rate than the RIRS, sometimes reaching 83% [9]. Furthermore, the SFRs following multi-session treatments were not significantly different between the groups even for renal stones larger than 2 cm [14].
The surgical instruments and techniques for minimal invasive treatment of renal stones have been improved. Pietropaolo et al. [12] reported that there has been a steep rise of URS from 2000 to 2015 because of innovation in flexible ureteroscopes. The ureteral access sheath (UAS) also has become an important device for RIRS. The UAS facilitates easy reentry into the ureter for stone fragments’ removal or upper tract biopsies [17]. Furthermore, the use of UAS has resulted in improved stone-free rate and operative visibility by efficient irrigation, which consequently maintains lower intrarenal pressures and shortened operative times [2].
However, the placement of the UAS may have adverse effects including ureteral injuries [18]. Some studies showed that UAS may transiently decrease ureteral blood flow by overdistension. These changes can cause long-term problems including ureteral stricture, although the rate of ureteral stricture is equivalent in URS regardless of access sheath application. For this reason, preoperative double-J stenting with UAS is performed in many centers for passive dilation of ureter to prevent these ureteral traumas and improve SFR. However, preoperative stenting unavoidably leads to extra costs and complications such as flank pain, hematuria, urinary symptoms and urinary tract infection [1]. These problems are one of the reasons that patients complain about the procedure and sometimes refuse to get ureteroscopic treatment.
The aim of this study was to assess the effect of preoperative ureteral stenting duration on the outcomes of RIRS for the renal stones.
Patients and methods
Patients
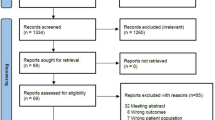
This study was approved by our institutional review board and we reviewed the data from 593 patients who underwent RIRS for renal stones between May 2011 and April 2017 at our institution. Among these patients, those who underwent RIRS for renal stones more than 30 days after preoperative double-J stenting or had a ureteral stricture, congenital UPJO and duplicated ureter in a preoperative imaging study such as CT were excluded from the study. Patients who underwent hemodialysis for ESRD, passed the stones or were treated with ureteroscopic lithotripsy for rigid ureteroscope cases were also excluded from this study.
Overall, 560 patients were included in our study. The patients’ classification was decided according to surgeon’s preference or change of practice.
Outcome analysis
Each patient was directed into one of the three groups according to their preoperative ureteral stenting duration. The no stenting group (group 1) included patients who underwent RIRS without stent before the operation. The short preoperative stenting group (group 2) included patients who underwent RIRS within 7 days after stenting. The long preoperative stenting group (group 3) included patients who underwent RIRS more than 7 days after stenting. Those who underwent RIRS just 7 days after stenting were included in Group 3.
We analyzed data on age, gender, body mass index (BMI) and stone parameters (e.g., stone size). The rate of intraoperative ureteral balloon dilation, ureteral injuries, readmission, other complications and SFR according to the groups were compared. Stone-free rate was defined as the absence of stone fragments or stone fragment of ≤ 1 mm on postoperative imaging at 1–4 weeks after discharge (Fig. 1).

Comparison of surgical outcomes according to the duration of preoperative ureteral stenting
The ureteral injuries were described in a previous study [2] and classified as Grade I: injury involving just the mucosal layer without smooth muscle; Grade II: injury involving just the smooth muscle without involvement of the adventitia; Grade III: ureteral penetration involved the full thickness of the ureteral wall; and Grade IV: avulsion involving the total ureter with complete rupture. The highest grade injury was recorded if different grade of injuries were mixed. The other perioperative complications were classified according to the modified Clavien-Dindo classification [4] and postoperative ureteral stricture was included.
Additionally, the infective complications were reported using rigorous criteria according to the literature. We used the definition of sepsis provided by the international sepsis definitions conference. Sepsis was defined as the presence of a source of infection with systemic inflammatory response syndrome (SIRS). The hydronephrosis was classified grade IIIa because we treated it with endoscopic intervention under local anesthesia and the ureteral stricture was classified grade IIIb because the correction was done under general anesthesia. The perirenal abscess was also treated with percutaneous intervention under local anesthesia.
RIRS procedure
All procedures were performed by three experienced urologists in our department according to standard operative protocols. Antibiotic prophylaxis with second-generation cephalosporin was administered 1 h before RIRS procedure was started. Most of all RIRS were performed with Olympus® URF-P3 flexible ureteroscope and using a safety guidewire. Ancillary devices included UASs, laser fibers and stone retrieval baskets. UASs included the Cook Flexer® with an inner and outer diameter of 12 and 14Fr, 14Fr and 16Fr. Laser fibers included the Coherent® 200 and 365 µ holmium light guide laser fibers with the Trimedyne® holmium laser generator were used. Ncircle® 2.4Fr nitinol tipless stone extractor was also used.
Majority of the patients received a 6Fr double-J stent at the end of operations and all patients underwent kidney, ureter and bladder (KUB) or non-contrast CT about 1–4 weeks after treatment. At 1–2 weeks after RIRS, the double-J stent was removed in the clinic’s offices.
Statistics
Data were collected retrospectively, entered into an Excel (Microsoft) spreadsheet, and analyzed with the Statistical Package for the Social Science version 22.0. The analysis of variance (ANOVA) test was used for comparing surgical outcomes and characteristics of patients and stones among the groups. To provide detailed information about the ANOVA results, Tukey, Bonferroni and Dunnett tests were also used. All tests were two-sided with significance reported for p < 0.05.
Results
A total of 560 patients who underwent RIRS for renal stones were included in this study: 215 patients (38.4%) in the no stenting group (group 1), 177 patients (31.6%) in the short preop-stenting group (group 2) and 168 patients (30.0%) in the long preop-stenting group (group 3). Table 1 shows there were no statistically significant differences among the groups for age (p = 0.361), BMI (p = 0.977), gender (p = 0.233), total number of stones (p = 0.440), and bilaterality of stones (p = 0.292). The overall mean duration of preoperative ureteral stenting was 4.4 (± 4.4) days and 4.9 (± 0.9) days in group 2, and 9.7 (± 3.2) days in group 3 (p < 0.001).
Table 2 shows that the overall mean operative time was 78.6 (± 41.9) min and it was 82.4 (± 45.6) min in group 3. This was longer than group 1 and 2, but there were no significant differences among the groups (p = 0.280). The overall SFR was 81.3% (p = 0.433) and the rate of readmission was 5.9% (p = 0.583) and no statistically significant differences were seen. To contrast, the rate of intraoperative ureteral dilation was significantly higher in group 1 (9.3%) than group 2 and 3 (5.7%, 6.0%, respectively, p < 0.001). Although there were no statistically differences in the rate of ureteral injuries (7.0, 5.1 and 2.4%, respectively, p = 0.123), the only case of ureteral injury grade IV occurred in group 1. And surprisingly, 9 of 10 cases of grade II ureteral injuries occurred in group 1.
Table 3 shows that the type of overall perioperative complications which occurred in patients of this study excluded ureteral injuries. All of the complications were graded by the modified Clavien-Dindo classification system. Perioperative complications occurred in 48 patients (8.6%), without any differences among the groups (12.1, 6.8 and 6.0%, respectively, p = 0.061). Two patients in group 1 showed postoperative hydronephrosis and were treated with D-J stent insertion under local anesthesia. 24 patients (4.3%) who were diagnosed with urinary tract infection and acute pyelonephritis were treated with antipyretics and antibiotics during re-hospitalization. In four patients (0.7%), sepsis was diagnosed and these patients underwent blood culture, managed by intravenous fluids with broad-spectrum antibiotics until urine or blood cultures indicated that oral therapy was appropriate. All of these patients required the intensive care unit.
Discussion
RIRS is increasingly being used as the first-line treatment for patients with renal stones [6]. In RIRS, placing the UAS improves the operative outcomes, including operative time and it can be explained by the fact that UAS diverts the irrigation fluid stream externally and decreases the requirement for intermittent bladder drainage during the procedure.
In cases of RIRS for infectious stones, massive fluid irrigation during RIRS increases renal pelvic pressure and results in fluid extravasation and absorption. This can be detrimental and contributes to the development of sepsis during the procedures. One of the animal studies demonstrated that irrigation pressure greater than 150 mmHg significantly influenced pathologic changes in the kidneys of mini pigs, such as submucosal edema, congestion, and focal renal scarring, compared with low-pressure (90 mmHg) irrigation [13]. These adverse effects can be reduced using the UAS during RIRS by decompressing renal pelvic pressure but can sometimes lead to ureteral injuries. Previous studies have shown that UAS-related ureteral injuries were 46.5% and high-grade injuries were seen in 13.3% of patients [18].
The ureter can be overdistended by UAS placing and some studies reported that it decreases blood flow to the ureter by as much as 35.5% of the baseline blood flow. The patients who had a 14/16F UAS used for RIRS showed more a rapid decrease of blood flow than with a 12/14F UAS and the ureteral ischemic damage can be explained.
Bach et al. [3] reported that the use of new digital flexible ureteroscopes made improvement in image quality, better durability and improved stone-free rate, but there are some drawbacks in these scopes such as increased use of ureteral access sheath and distal ureteral injuries because of the larger size of the distal tip diameter. However, several studies already have proven the safety of these scopes and we did not experience these complications.
Traxer et al. [18] reported that the risk of ureteral injury decreased about seven times using preoperative double-J stenting. Additionally, another study suggested that there are no differences in late complications between the patients with and without UAS (90 days postoperative symptoms 43% vs. 30%, p = 0.2), despite intraoperative complications being more common in patients with UAS [21]. However, recent studies have reported that preoperative double-J stenting is not necessary to prevent ureteral injuries during ureteroscopic surgery. We summarized these results in Table 4.
The potential impact of preoperative double-J stenting is an important issue. The ureteral stent led to various urinary tract symptoms including flank pain, hematuria and results in a decreased quality of life in up to 80% of patients [7]. Zhang et al. [22] reported that there are no significant differences in operative outcomes between the stenting and no stenting groups, including the rate of complications and SFRs (73.2% vs. 71.0%, p = 0.854). Other studies reviewed the impact of double-J stenting before ureteroscopic procedure and did not find any association between preoperative stenting and an increased rate of complications [8, 10]. We found the same results for SFR, and the rate of ureteral injuries and complications were not significantly different among the groups. Nevertheless, preoperative double-J stenting is significantly effective in preventing intraoperative ureteral balloon dilation. This result means that double-J stenting can sufficiently widen the intramural ureter without the need for UAS.
Recently, an animal study by Vachon C. et al. [20] reported that the ureteral diameters did not show any significant differences in the duration of stenting. (before stenting: 1.70, 2 weeks after stenting: 2.86 and 6 weeks after stenting: 2.80 mm). Some of articles suggested that preoperative double-J stenting can reduce the rate of intraoperative ureteral balloon dilation and also improve the convenience of RIRS procedure. This passive dilation by double-J stenting allowed for successful ureteroscopic lithotripsy but this was not the impressive factor related to SFR. Shields et al. [16] reported that a successful RIRS procedure was negatively associated with primary stone size (p = 0.020), total stone number (p = 0.001) and cumulative stone burden (p < 0.001), but preoperative double-J stenting was not statistically associated with success rates (adjusted OR 2.22; 95% CI 0.88, 5.63; p = 0.254).
However, Rubenstein et al. [15] reported a significant improvement of SFR in preoperative double-J stenting patients (47% vs. 67%, p = 0.048). Perlmutter et al. [11] also reported that passive dilation of the ureter by preoperative double-J stenting improves the success rate of ureteroscopic lithotripsy but it was not statistically significant. Fabrizio et al. [5] also evaluated the effect of passive ureteral dilation using preoperative double-J stenting and did not suggest any further impacts on SFR.
There are inherent limitations to our study. This is a retrospective study and did not minimize bias, as may be done when performing a prospective and randomized study and this study included three surgeons and the surgical techniques may not have been uniformed. Comparison of surgical outcomes associated with the type of UAS used and the past history of nephroureterolithiasis is also needed. This study has lack of information regarding quality of life of patients and numerical pain scores that may have significant factors for undergoing preoperative double-J stenting or not.
Conclusions
This study showed that preoperative stenting can prevent high-grade ureteral injuries and reduce the rate of intraoperative balloon dilation. However, preoperative stenting duration has no significant effect on operative outcomes such as operative time, the rate of ureteral injuries, other perioperative complications, readmission and SFR. If a preoperative double-J stenting is optional, our study may help the patients and clinicians to make a final decision. Large prospective randomized controlled studies are required to further figure out the effect of preoperative ureteral stent.
References
Al-Marhoon MS, Shareef O, Venkiteswaran KP (2012) Complications and outcomes of JJ stenting of the ureter in urological practice: a single-centre experience. Arab J Urol 10:372–377
Auge BK, Pietrow PK, Lallas CD et al (2004) Ureteral access sheath provides protection against elevated renal pressures during routine flexible ureteroscopic stone manipulation. J Endourol 18:33–36
Bach C, Nesar S, Kumar P et al (2012) The new digital flexible ureteroscopes: ‘Size Does Matter’—increased ureteric access sheath use! Urol Int 89:408–411
Dindo D, Demartines N, Clavien PA (2004) Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 240:205–213
Fabrizio MD, Behari A, Bagley DH (1998) Ureteroscopic management of intrarenal calculi. J Urol 159:1139–1143
Ghani KR, Wolf JS Jr (2015) What is the stone-free rate following flexible ureteroscopy for kidney stones? Nat Rev Urol 12:281–288
Joshi HB, Stainthorpe A, MacDonagh RP (2003) Indwelling ureteral stents: evaluation of symptoms, quality of life and utility. J Urol 169:1065–1069
Lumma PP, Schneider P, Strauss A et al (2013) Impact of ureteral stenting prior to ureterorenoscopy on stone-free rates and complications. World J Urol 31:855–859
Mousavi-Bahar SH, Mehrabi S, Moslemi MK (2011) Percutaneous nephrolithotomy complications in 671 consecutive patients: a single-center experience. Urol J 8:271–276
Netsch C, Knipper S, Bach T et al (2012) Impact of preoperative ureteral stenting on stone-free rates of ureteroscopy for nephroureterolithiasis: a matched-paired analysis of 286 patients. Urology 80:1214–1219
Perlmutter AE, Talug C, Tarry WF et al (2008) Impact of stone location on success rates of endoscopic lithotripsy for nephrolithiasis. Urology 71:214–217
Pietropaolo A, Proietti S, Geraghty R et al (2017) Trends of ‘urolithiasis: interventions, simulation, and laser technology’ over the last 16 years (2000–2015) as published in the literature (PubMed): a systematic review from European section of Uro-technology (ESUT). World J Urol 35:1651–1658
Rehman J, Monga M, Landman J et al (2003) Characterization of intrapelvic pressure during ureteropyeloscopy with ureteral access sheaths. Urology 61:713–718
Resorlu B, Unsal A (2012) Comparison of percutaneous nephrolithotomy and retrograde flexible nephrolithotripsy for the management of 2–4 cm stones: a matched-pair analysis. BJU Int 109:4–6
Rubenstein RA, Zhao LC, Loeb S et al (2007) Prestenting improves ureteroscopic stone-free rates. J Endourol 21:1277–1280
Shields JM, Bird VG, Graves R et al (2009) Impact of preoperative ureteral stenting on outcome of ureteroscopic treatment for urinary lithiasis. J Urol 182:2768–2774
Stern JM, Yiee J, Park S (2007) Safety and efficacy of ureteral access sheaths. J Endourol 21:119–123
Traxer O, Thomas A (2013) Prospective evaluation and classification of ureteral wall injuries resulting from insertion of a ureteral access sheath during retrograde intrarenal surgery. J Urol 189:580–584
Türk C, Petrik A, Knoll T et al (2016) EAU guidelines on interventional treatment for urolithiasia. Eur Urol 69:475–482
Vachon C, Defarges A, Brisson B et al (2017) Passive ureteral dilation and ureteroscopy after ureteral stent placement in five healthy Beagles. Am J Vet Res 78:381–392
Wang HH, Huang L, Routh JC et al (2011) Use of the ureteral access sheath during ureteroscopy in children. J Urol 186:1728–1733
Zhang J, Xu C, He D et al (2016) Flexible ureteroscopy for renal stone without preoperative ureteral stenting shows good prognosis. PeerJ 29:e2728
Author information
Authors and Affiliations
Contributions
MHL: project development, data analysis, manuscript writing/editing. IJL, TJK: data analysis. CWJ, SCL, SKH, SSB: data collection. JJO: project development, data collection, data analysis, manuscript editing
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest with any institution or product.
Ethical approval
We obtained Institutional Review Board approval. All procedures performed in studies were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. For this type of study formal consent is not required.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Lee, M.H., Lee, I.J., Kim, T.J. et al. The effect of short-term preoperative ureteral stenting on the outcomes of retrograde intrarenal surgery for renal stones. World J Urol 37, 1435–1440 (2019). https://doi.org/10.1007/s00345-018-2519-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00345-018-2519-9