
Abstract
Purpose
To describe the surgical technique, to analyze outcomes and to provide an overview of the current status of laparoendoscopic single site (LESS) adrenalectomy.
Methods
A comprehensive PubMed search was performed for all relevant urological literature regarding LESS and adrenal surgery. In addition, experience gained at the authors’ own institutions was considered. Clinical descriptive and comparative reports on LESS adrenal surgery procedures were analysed.
Results
LESS adrenal surgery has been effectively performed for a number of indications. A wide variety of approaches (transperitoneal versus retroperitoneal, multichannel trocar versus multiple ports, trans- or extraumbilical) have been described. LESS adrenalectomy seems to be safe, taking more time than the standard laparoscopic counterpart but appears to offer the patient less postoperative discomfort. Technical difficulties of the procedure include the requirement of more time for adjustment of articulating instruments, longer ‘one-handed’ manipulation time, and a high peroperative tissue re-grasping rate.
Conclusions
The feasibility and safety of LESS adrenalectomy has been demonstrated. Only long-term follow-up outcomes will prove its benefits over conventional laparoscopy and define the role and the oncological safety of LESS adrenal surgery.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Since the first pioneering experiences [1], all extirpative and reconstructive urological procedures has been described and shown to be feasible and safely performed with Laparoendoscopic single-site surgery (LESS). Over the last few years there has been an increasing enthusiasm and growing interest in this novel minimally invasive surgical technique [2].
Laparoscopic access to the adrenal gland was described about two decades ago [3] and has now virtually replaced open surgery in the management of adrenal lesions; most would agree that it currently represents the standard of care for adrenalectomy in most cases [4]. That said, laparoscopic adrenalectomy is regarded as a challenging procedure because of the anatomical topography of the gland itself, making dissection somewhat inherently difficult [5].
In 2005, Hirano et al. [6] reported the first series of ‘single site’ retroperitoneal adrenalectomies using conventional laparoscopic instruments without gas insufflation by using a 4-cm rectoscope tube as an access device. In 2008, Castellucci et al. [7] conducted a single-site transperitoneal adrenalectomy using three 5-mm trocars through a 2-cm incision. The first successful single-multilumen port transperitoneal-adrenalectomy was reported by Cindolo et al. [8] in 2009 for the excision of a 4-cm nonfunctional left adrenal mass using a 3-cm incision. Over the last 2 years, several series of LESS adrenalectomy have been reported, so that available evidence on this surgical procedure is larger.
Aim of this study is to describe the surgical techniques, to analyze the outcomes and to provide an overview of the current status of LESS adrenalectomy.
Methods
A comprehensive electronic literature search was conducted in January 2011 using the Medline database—through either PubMed or Ovid as a search engine—to identify all publications relating to LESS adrenalectomy. The search was conducted using a free-text protocol that included the following terms: adrenalectomy; laparoendoscopic single-site surgery (LESS); single-port access (SPA) surgery; single-incision laparoscopic surgery (SILS); single-port laparoscopy (SPL); single-incision laparoscopy(SIL); single-trocar laparoscopic surgery. The experience gained at authors’ own institutions was also considered.
Indications
As a general principle, all eligible laparoscopic surgery patients may be considered for LESS depending on surgeons’ own experience (Fig. 1).

CT scan: coronal view showing 3.17 cm right adrenal mass amenable for LESS adrenalectomy
Laparoscopic adrenalectomy is nowadays considered the reference standard surgical procedure for patients with benign adrenal adenomas. Moreover it is increasingly being used as treatment for pheochromocytomas and some malignant cortical tumors preoperatively classified as benign [9]. Nevertheless, debate over the use of laparoscopic surgery for pheochromocytoma continues due to concern of possible hemodynamic instability as a result of catecholamine release. For adrenocortical carcinoma, the role of laparoscopy remains controversial and probably limited to skilled surgeon for lesions less than 10 cm [10].
Available studies show that LESS adrenal surgery can be effectively performed for variable indications (Table 1) [11–17].
When starting out with LESS, patient selection criteria are expected to be stringent. Disease features (i.e., locally advanced disease requires more extensive dissection) as well as the type of patient (i.e., body habitus, BMI, comorbidity score, previous surgery, or radiation, personal preferences for better cosmetic outcome) should considered. Early in one’s own experience with LESS adrenalectomy, and to minimize the risks of complications and conversion, one should select an ‘easy’ case. With growing experience, indications can be expanded to include more challenging cases (Table 2) [9–17]. In general, there should be a low threshold for conversion to standard laparoscopy, or even open surgery if necessary.
In the pioneering study by Jeong et al. [11] half of their patients were found to have pheochromocytoma at histology. Difficulties in dissection during LESS adrenalectomy might lead to excessive catecholamine secretion and an increased risk of a hypertensive crisis. In this report, the authors highlighted how experienced anesthesiology teams, appropriate perioperative medical management, and efforts to minimize adrenal manipulation during surgery are of utmost importance to minimize the risk of hypertensive crises.
As previously reported even with conventional laparoscopic surgery [18], in case of patients with tumor greater than 4 cm, the limited working space does represent a significant challenge, an issue that needs to be considered carefully.
Initial experience with LESS partial adrenalectomy to treat aldosterone-producing adenomas has been recently described by Yuge et al. [19]. The first report of successful simultaneous bilateral LESS, consisting of right partial, and left total adrenalectomy for bilateral primary aldosterone-producing adrenal adenomas has been also reported [20].
Surgical technique
Access
As for conventional laparoscopic adrenalectomy, both the transperitoneal and the retroperitoneal routes have been described for LESS adrenalectomy with variable strategy in terms of patient positioning, incision site and port placement (Table 3) [11–17, 20–23].
The most common position for LESS access has been the umbilicus, for obvious cosmetic benefits. Nozaki et al. recently describe a detailed technique of intraumbilical access to solve the problem associated with crossover instrumentation during LESS adrenalectomy. This includes a longitudinal incision of the umbilicus and a wider area of subcutaneous tissue dissection to accommodate multiple ports. The incision length remains within the depression of the umbilicus, therefore, preserving normal umbilical appearance.
Nevertheless, LESS adrenalectomy through an umbilical access can be extremely challenging due to the angle of approach and difficult organ retraction. Indeed, as the position of the area of dissection becomes more cranial, the difficulty of dissection with transumbilical LESS procedures increases almost exponentially [24].
Because of anatomical topography of the adrenal gland, the distance from the entry port to the target organ issue in a transumbilical LESS approach is longer than, for example, one can have in kidney procedures. Moreover, the transumbilical approach becomes more tangential in direction. And, given, the currently available instrumentation, this translates into significantly unfavorable ergonomics and ultimately a more demanding procedure. Indeed, as the position of the area of dissection becomes more cranial, the difficulty of dissection with transumbilical LESS procedures increases almost exponentially.
This issue raises the question of whether a subcostal or retroperitoneal approach for LESS adrenalectomy provides any benefits over a transumbilical approach.
Some have proposed a subcostal incision [8, 23], which is still considered a LESS approach according to the current terminology, even if it is cosmetically less appealing.
Experience with retroperitoneal urologic LESS remains limited [25, 26]. The retroperitoneal approach has some advantages including more direct access to the retroperitoneal organs, less need for visceral retraction, and elimination of the risk for intraperitoneal contamination with tumor cells or infectious organisms [27]. Because the retroperitoneal space is limited, articulating, and curved instruments are not as useful as in transperitoneal procedures. Similarly to what has been shown for conventional laparoscopy [28], Shi et al. [21] suggested that morbidly obese patients could benefit from LESS retroperitoneoscopic access. Nine of the patients in their series had a BMI greater than 30 kg/m2 and this did not cause any difficulties during port set or dissection in any of them.
Agha et al. [16] reported a small series of eight patients undergoing single-incision adrenalectomy, four of them retroperitoneoscopically, four transperitoneally. Tumor localization was an important factor for choice of access. Patients undergoing left adrenalectomy were included in the transperitoneal group, whereas tumors of the right adrenal gland were operated retroperitoneoscopically.
Surgical technique and instrumentation
LESS adrenalectomy necessarily aims to duplicate a standard transperitoneal or retroperitoneoscopic adrenalectomy.
For this reason the surgeon faces the problem of following the same surgical steps but within the recognized ergonomic constraints and limitations related to LESS, mainly arise from instrument clashing and lack of true triangulation [2]. These major challenges can be addressed in part by the use of articulating instruments. Nevertheless, currently, laparoscopic articulating instruments can be difficult to use, bulky, and ergonomically suboptimal.
Aauthors have adopted intraoperative strategies, such as “crossover” [13] or “one” handed [14] manipulation, which remain challenging and ergonomically poor. This might contribute to an increase in tissue re-grasping due to the inadequate or insufficient counter-traction and suboptimal angle for a precise and safe dissection and it can ultimately translate into prolonged operative time [19].
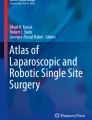
As mentioned above, in spite of a better cosmetic effect and better working space, during transumbilical LESS adrenalectomy the distance between the umbilicus and the adrenal gland is longer, which usually makes the conventional laparoscopic instrument unable to reach the upper pole of the adrenal gland. Thus, an extra-long laparoscope and laparoscopic instruments usually are required for effective traction and dissection. Moreover, in transperitoneal LESS adrenalectomy, liver, or spleen retraction usually are inevitable [15]. However, any additional instrument through the same incision in LESS increases the fighting of instruments, thus the difficulty performing LESS. In this respect, the use of 2 or 3 mm needlescopic instruments can represent an effective solution (Fig. 2) [12, 13].

External view of the surgical field during LESS right adrenalectomy. a use of a extraumbilical multichannel port (Endocone®, Karl Storz, Tuttlingen, Germany) and of an extra 3.5 mm trocar for liver retraction. b use of another extraumbilical multichannel port (Triport®, Olympus, Tokyo, Japan)
Specific access devices used in single-port surgery allow multiple instruments to be passed through them at the same time. Several types of these ports currently are commercially available and their use have been described for LESS adrenalectomy: TriPort® (Olympus, Tokyo, Japan) [8, 17, 21], SILS Port® (Covidien, Gosport, UK) [12, 16], and OCTOport® (Dalim Surg, Seoul, South Korea) [20]. Others have effectively used homemade single port devices [11, 15].
Disadvantages related to the loss of the triangulation during LESS can be overcome by using special instruments. Several reports have described the use of fixed-shaft bent instruments to facilitate single-port surgery and several actively articulating instruments also have been developed [2]. Although the aforementioned instruments are helpful for attempting to resolve the problems of triangulation, the lack of sufficient strength to provide robust retraction and dissection persist.
Outcomes
Case series
Over the last 2 years, several groups reported their early outcomes of LESS adrenalectomy. These series are all limited by the small sample size and mostly address the feasibility of the procedure [13, 15–17, 29].
Comparative studies (Table 4)
Jeong et al. [11] reported the first a matched case–control study to demonstrate the technical feasibility of LESS compared with the conventional laparoscopic procedure in the removal of a benign adenoma. Nine patients undergoing LESS adrenalectomy were compared with 17 patients undergoing conventional laparoscopic adrenalectomy. No significant differences were found between the groups in terms of mean operative time, blood loss, and postoperative hospital stay. Postoperative pain, as measured by the number of days of intravenous patient controlled anesthesia use, was significantly lower in the LESS group (0.9 vs. 1.9 days, P = 0.047). Perioperative complications were similar between the two groups.
Shi et al. [21] evaluated LESS retroperitoneoscopic adrenalectomy in comparison with the current standard operation procedure. Nineteen patients underwent LESS and their outcomes were compared with a contemporary 1:2 matched-pair cohort of 38 patients who underwent standard retroperitoneoscopic adrenalectomy. The two groups were comparable in terms of the estimated blood loss, postoperative hospital stay, and postoperative complications. The LESS group had a longer median operative time (55 vs. 41.5 min; P = 0.0004), whereas the in-hospital use of analgesics was significantly less (5 vs. 12 morphine equivalents; P = 0.03).
Ishida et al. [12] reported a study was comparing ten consecutive transumbilical LESS adrenalectomies and ten conventional laparoscopic adrenalectomies for benign adrenal tumors. No significant differences in operative time, estimated blood loss, or resumption of oral intake were observed between two groups. In LESS group only, time was needed for adjustment of roticulator (14.5 ± 8.1 min). After subtracting the time needed for adjustment, operative time between two groups was more comparable (76.7 vs. 74.3 min, P = 0.880). One-handed manipulation time in LESS group decreased in a time-dependent manner (r = −0.806, P = 0.0049). Tissue re-grasping during operation was more frequently observed in LESS group (16.2 vs. 2.2 times, P = 0.001).
Walz et al. [14] reported the largest comparative matched-control study so far comparing their method of endoscopic single-access adrenalectomy with the conventional retroperitoneoscopic approach. Fifty single-access retroperitoneoscopic adrenalectomies were performed in 47 selected patients. Patients treated by the traditional retroperitoneoscopic three-port approach served as control group. No major complications occurred in both groups. Operative time was longer for the LESS group (56 ± 28 vs. 40 ± 12 min; P < 0.05). Postoperatively, pain medication was less frequently administered in LESS patients (47 vs. 75%; P = 0.01). Mean hospital stay was also shorter for the LESS group (2.4 ± 0.7 vs. 3.1 ± 1.2 days; P < 0.01).
Current controversies
LESS adrenalectomy appears to an effective treatment option in small adrenal masses requiring extirpation. Good laparoscopic skills and careful patient selection are essential; additional small trocars should be considered to help suturing and for liver retraction.
It remains to be said, however, that despite promising early outcomes, the benefits of LESS are not clear at present, apart from cosmesis [1]. Prospective randomized studies are largely awaited to define the benefits of this technique for patients as well as to elucidate the cost-effectiveness of the approach. Refinement of instruments and application of robotics are likely to improve intraoperative ergonomics, allowing easier training and facilitating the current steep learning curve [30]. Agha et al. [16] reported to have embarked in LESS adrenal surgery after having performed more than 300 conventional adrenalectomies and speculated that this have lead to a short learning curve. Similarly, Walz et al. [14, 29] reported to have developed their LESS technique for adrenalectomy after having performed more than 800 adrenalectomies by the posterior retroperitoneoscopic approach.
In reporting one of the largest series of LESS retroperitoneoscopic adrenalectomy, Zhang et al. [17] observed that in the initial ten cases median operative time was significantly longer (62 vs. 50 min) and median blood loss was significantly higher (75 vs. 10, each P < 0.001) than in the subsequent 15. Thus, they found a significant association between operative time and the number of procedures performed.
Future studies will define the oncological safety of the LESS technique for adrenal surgery. However, as it appears to duplicate the laparoscopic technique, it is likely that also oncological outcomes will be unchanged. In the meantime, ethical and consent related issues will continue to be need to be addressed [2, 31, 32].
Conclusions
The feasibility and safety of LESS adrenalectomy has been demonstrated by a number of surgeons. Further clinical research is warranted to define the role of LESS in the field of minimally invasive adrenal surgery and prove its efficacy over conventional laparoscopic surgery.
References
Tracy CR, Raman JD, Cadeddu JA, Rane A (2008) Laparoendoscopic single-site surgery in urology: where have we been and where are we heading? Nat Clin Pract Urol 5:561–568
Autorino R, Cadeddu JA, Desai MM, Gettman M, Gill IS, Kavoussi LR, Lima E, Montorsi F, Richstone L, Stolzenburg JU, Kaouk JH (2011) Laparoendoscopic Single-site and Natural Orifice Transluminal Endoscopic Surgery in Urology: A Critical Analysis of the Literature. Eur Urol 59:26–45
Gagner M, Lacroix A, Bolte E (1992) Laparoscopic adrenalectomy in Cushing’s syndrome and pheochromocytoma. N Engl J Med 327(14):1033
McCauley LR, Nguyen MM (2008) Laparoscopic radical adrenalectomy for cancer: long-term outcomes. Curr Opin Urol 18(2):134–138
Strebel RT, Müntener M, Sulser T (2008) Intraoperative complications of laparoscopic adrenalectomy. World J Urol 26(6):555–560
Hirano D, Minei S, Yamaguchi K et al (2005) Retroperitoneoscopic adrenalectomy for adrenal tumors via a single large port. J Endourol 19:788–792
Castellucci SA, Curcillo PG, Ginsberg PC et al (2008) Single port access adrenalectomy. J Endourol 22:1573–1576
Cindolo L, Gidaro S, Tamburro FR, Schips L (2010) Laparo-endoscopic single-site left transperitoneal adrenalectomy. Eur Urol 57(5):911–914
Guazzoni G, Cestari A, Montorsi F et al (2001) Current role of laparoscopic adrenalectomy. Eur Urol 40:8–16
Demeure MJ (2010) Surgery: does laparoscopic adrenalectomy have a role in suspected ACC? Nat Rev Urol 7(10):538–539
Jeong BC, Park YH, Han DH, Kim HH (2009) Laparoendoscopic single-site and conventional laparoscopic adrenalectomy: a matched case-control study. J Endourol 23:1957–1960
Ishida M, Miyajima A, Takeda T, Hasegawa M, Kikuchi E, Oya M (2010) Technical difficulties of transumbilical laparoendoscopic single-site adrenalectomy: comparison with conventional laparoscopic adrenalectomy. World J Urol. doi: 10.1007/s00345-010-0636-1
Cindolo L, Gidaro S, Neri F, Tamburro FR, Schips L (2010) Assessing feasibility and safety of laparoendoscopic single-site surgery adrenalectomy: initial experience. J Endourol 24(6):977–980
Walz MK, Groeben H, Alesina PF (2010) Single-access retroperitoneoscopic adrenalectomy (SARA) versus conventional retroperitoneoscopic adrenalectomy (CORA): a case–control study. World J Surg 34(6):1386–1390
Chung SD, Huang CY, Wang SM, Tai HC, Tsai YC, Chueh SC (2010) Laparoendoscopic single-site (LESS) retroperitoneal adrenalectomy using a homemade single-access platform and standard laparoscopic instruments. Surg Endosc 25(4):1251–1256 Epub ahead of print
Agha A, Hornung M, Iesalnieks I, Glockzin G, Schlitt HJ (2010) Single-incision retroperitoneoscopic adrenalectomy and single-incision laparoscopic adrenalectomy. J Endourol 24(11):1765–1770
Zhang X, Shi TP, Li HZ, Ma X, Wang BJ (2011) Laparo-endoscopic single site anatomical retroperitoneoscopic adrenalectomy using conventional instruments: initial experience and short-term outcome. J Urol 185(2):401–406
Porpiglia F, Destefanis P, Fiori C et al (2002) Does adrenal mass size really affect safety and effectiveness of laparoscopic adrenalectomy? Urology 60:801–805
Yuge K, Miyajima A, Hasegawa M et al (2010) Initial experience of transumbilical laparoendoscopic single-site surgery of partial adrenalectomy in patient with aldosterone-producing adenoma. BMC Urol 10(1):19
Jeong CW, Park YH, Shin CS, Kim HH (2010) Synchronous bilateral laparoendoscopic single-site adrenalectomy. J Endourol 24(8):1301–1305
Shi TP, Zhang X, Ma X et al (2010) Laparoendoscopic single-site retroperitoneoscopic adrenalectomy: a matched-pair comparison with the gold standard. Surg Endosc. doi:10.1007/s00464-010-1506-z
Nozaki T, Ichimatsu K, Watanabe A, Komiya A, Fuse H (2010) Longitudinal incision of the umbilicus for laparoendoscopic single site adrenalectomy: a particular intraumbilical technique. Surg Laparosc Endosc Percutan Tech 20(6):e185–e188
Tunca F, Senyurek YG, Terzioglu T, Sormaz IC, Tezelman S (2010) Single-incision laparoscopic left adrenalectomy. Surg Laparosc Endosc Percutan Tech 20(4):291–294
Autorino R, Stein RJ, Kaouk JH (2010) Re: Luca Cindolo, Stefano Gidaro, Fabiola R. Tamburro, Luigi Schips. Laparo-endoscopic single-site left transperitoneal adrenalectomy. Eur Urol 57: 911–4. Eur Urol 57(5):e47
Ryu DS, Park WJ, Oh TH (2009) Retroperitoneal laparoendoscopic single-site surgery in urology: initial experience. J Endourol 23:1857–1862
White WM, Goel RK, Kaouk JH (2009) Single-port laparoscopic retroperitoneal surgery: initial operative experience and comparative outcomes. Urology 73:1279–1282
Rubinstein M, Gill IS, Aron M et al (2005) Prospective, randomized comparison of transperitoneal versus retroperitoneal laparoscopic adrenalectomy. J Urol 174:442–445
Berglund RK, Gill IS, Babineau D, Desai M, Kaouk JH (2007) A prospective comparison of transperitoneal and retroperitoneal laparoscopic nephrectomy in the extremely obese patient. BJU Int 99:871–874
Walz MK, Alesina PF (2009) Single access retroperitoneoscopic adrenalectomy (SARA)-one step beyond in endocrine surgery. Langenbecks Arch Surg 394(3):447–450
Rane A, Autorino R (2011) Robotic natural orifice translumenal endoscopic surgery and laparoendoscopic single-site surgery: current status. Curr Opin Urol 21(1):71–77
Gettman MT, White WM, Aron M et al (2011) Where do we really stand with LESS and NOTES? Eur Urol 59(2):231–234
Autorino R, Cadeddu JA, Desai MM et al (2011) Reply from Authors re: Jens J. Rassweiler. Is LESS/NOTES Really More? Eur Urol. doi: 10.1016/j.eururo.2010.08.040
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Rane, A., Cindolo, L., Schips, L. et al. Laparoendoscopic single site (LESS) adrenalectomy: Technique and outcomes. World J Urol 30, 597–604 (2012). https://doi.org/10.1007/s00345-011-0678-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00345-011-0678-z