
Abstract
The robotic technique, which was first introduced in laparoscopic heart surgery, has revolutionized laparoscopic surgery over the last 5 years. In May 2000, our department accomplished the first robot assisted laparoscopic radical prostatectomy. Since that time we have performed more than 118 such procedures and several other laparoscopic operations using the robotic technique. We here summarize our experience in robot assisted laparoscopic radical prostatectomy as it has been developed over the past 3 years. Between May 2000 and May 2003, 118 patients with clinically localized prostate cancer were operated using the telerobotic da Vinci Surgical System. Operations were performed with a senior surgeon at the console, assisted by an assistant and a nurse at the operating table. Bilateral pelvic lymph node dissection was undertaken as a first step in all patients. In the initial 60 cases, we investigated different laparoscopic approaches. We used transperitoneal as well as extraperitoneal approaches. For dissection of the prostate we used ascending, descending as well as combined techniques. The combined ascending and descending technique via the transperitoneal route was chosen in 30 patients, and via the extraperitoneal route in seven patients. A modification of the descending Montsouris technique was performed in 81 patients. The robot assisted laparoscopic radical prostatectomy with the da Vinci system has been well standardized. After performing more than 100 radical prostatectomies with this system, we conclude that in our hands the Mountsouris technique with only minor adoptions is the most appropriate technique for performing robot assisted radical prostatectomy.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Prostate cancer is the most common tumor of the genitourinary tract. Therefore, radical prostatectomy has become one of the most frequent procedures performed by urologists today [7]. Although the open retropubic radical prostatectomy is the gold standard procedure, laparoscopic radical prostatectomy has been introduced into clinical practice and has been standardized by Guillonneau and Vallancien [5, 6], Rassweiler [10] and others [1, 8, 3]. It has been shown that in addition to the general advantages of laparoscopic surgery, oncologic efficacy and functional outcome are compatible with the results of open surgery [6, 12].
A sophisticated telerobotic surgical system (da Vinci Surgical System, Intuitive Surgical, Mountain View, Calif., USA) has been developed to facilitate minimal invasive procedures. In our hospital the system was introduced by cardiac surgeons who were able to perform total endoscopic bypass surgery for the first time [9, 4].
We performed the first robot assisted laparoscopic radical prostatectomy with the da Vinci system in May 2000 [2]. Subsequently, more than 100 cases of robot assisted laparoscopic radical prostatectomy have been carried out and a technique of remote-controlled laparoscopic radical prostatectomy has been developed.
The method we present here was developed with our growing experience using the da Vinci system and our long experience with anatomic retropubic radical prostatectomy. The objective was to combine the advantages of laparoscopic surgery, e.g., small incisions, reduced blood loss, and quicker patient recovery with the advantages of modern robot technology, such as excellent 3-D vision, instrument dexterity, and an undisturbed eye-hand coordination.
Technique
The da Vinci system
The da Vinci Surgical System was developed to simplify laparoscopic surgery for the conventionally trained surgeon. The Endowrist instrument technology introduces additional grades of freedom and thereby a high degree of articulation of the laparoscopic tools, while the 3-D vision system gives the surgeon full control over the laparoscope as well as an excellent magnified view (10×).
Patient preparation
Patients are hospitalized the day before surgery. Usual bowel preparation with 3–6 l of Golytely solution readies the patient for the operation. The operation is performed under general anesthesia.
DJ-stenting
The initial 37 patients underwent cystoscopy and bilateral DJ-stenting prior to laparoscopic surgery to avoid postoperative infrarenal obstruction due to mucosal swelling. However, in the following 81 patients this precautionary step was omitted as ureteral orifices can be visualized and spared easily during laparoscopy. However, if stenting becomes necessary during the procedure it can easily be performed laparoscopically.
Patient positioning and Foley catheter
The patient is placed in the Trendelenburg position with both arms attached to the sides and both legs slightly straddled to provide access for the surgical cart column. Before the start of the procedure, a 18 F Foley catheter is placed and blocked with 10 cc of distilled water. An extension tube is connected to the catheter so that the bladder can be filled at any time.
Trocar placement
A 1–2 cm paraumbilical midline minilaparotomy is made (Hassan technique) and two special da Vinci 8 mm trocars are inserted by digital guidance or under visual control in the pararectal lines on both sides (Fig. 1). Next, a 12 mm standard trocar is placed in the median laparotomy (Fig. 1). Cranial and caudal to this trocar, the skin is closed to establish impermeability for the gas insufflation. Before the 3-D laparoscopic camera is placed in the midline trocar, the pneumoperitoneum is accomplished by insufflation with CO2 until the intraperitoneal pressure is 12 mmHg. Intraperitoneal organs are carefully inspected before the robot is attached.

Positioning of the trocars. In the midline the camera-trocar (12 mm), pararectal on both sides da Vinci-trocars (8 mm) and the two assistant-trocars laterally on both sides
Cart placement and connections
After attaching the 3-D-endocamera (InSite Vision System) to the medial robotic arm, two laparoscopic tools are inserted via the lateral 8 mm trocars under direct visual control and are connected to the left and right robotic arms. We usually start the procedure with a DeBakey forceps or a bipolar forceps on the left and a cautery hook on the right side. During the procedure, the DeBakey forceps on the left side is rarely changed, while the cautery hook on the right side is changed to round tip scissors or a needle driver.
In contrast to the first cases in which we used a 30° wide angle camera, we now use a 0° wide angle camera because of better imaging of the descending preparation at the rectal wall and the perfect view onto the urethral stump that supports the exact suture of the anastomosis.
Additional trocars
For the supportive actions of the assistant and the surgical nurse (e.g. holding structures or evacuation of lymph nodes), we insert two additional 10 mm standard trocars (Fig. 1). Conventional laparoscopic graspers are used for these supportive actions. The trocars are inserted bilaterally into the lower lateral abdomen just superior to the spina iliaca superior anterior under visual control.
Lymphadenectomy
After inspection of the abdominal organs and, if necessary, dissection of bowel adhesions of the ventral abdominal wall, we perform bilateral lymphadenetomy. The peritoneum is opened just above the iliac artery. The assistant holds the medial bladder ligament and the medial peritoneal fringe of the incision away from the vessels to allow a free view into the fossa obturatoria. Omitting the obturatoric nerve, the fat and lymphatic tissue of the fossa are dissected up to the bifurcation of the external and internal iliac artery. The tissue is removed via one of the lateral 10 mm trocars under visual control and sent to pathology for frozen section examination.
Prostatovesiculectomy
Distinct operative strategies were evaluated with the assistance of the da Vinci system. At the initiation of our program, we applied the surgical steps of our open retropubic procedure which is a combination of the ascending (Walsh) and descending (Campbell) techniques. This technique is feasible both via the transperitoneal (n=30) as well as the extraperitoneal route (n=7). As an alternative approach (n=81), we used a modification of the Montsouris technique, initially described by Guillonneau and Vallancien [5]. Using this technique, we started with the dissection of the vasa deferentes and the seminal vesicles from the recessus rectovesicalis and proceeded in an antegrad fashion after ligation of the venous plexus. However, after performing more than 118 procedures, the transperitoneally modified Montsouris technique became our standard procedure. This will now be described in detail.
Surgical strategy
Posterior dissection
The peritoneum is opened by a cross incision near the rectovesical peritoneal fold just beneath the bladder where the vasa deferentes are visible. Next, the vasa deferentes are mobilized and dissected. The dissected vasa are grasped by the assistant and pulled upwards. This opens a view onto the Denovilliers fascia, and the seminal vesicles can be prepared laterally. For the preparation of the seminal vesicles, the cautery hook is usually used. In cases of nerve sparing prostatectomy, the neurovascular bundles are bluntly separated laterocaudally with scissors and small clips are used for hemostasis. The cautery hook is not used in these cases.
After the vasa deferentes are dissected and the seminal vesicles completely mobilized, these structures are grasped and pulled forwards to attain a clear view of the Denonvilliers fascia. This is then opened to reach the dorsal aspect of the prostate. The prerectal fat is prepared with the cautery hook until the rectouretheral muscle is reached. At this point, the anterior approach is started. However, before the anterior dissection starts, careful blood coagulation is performed on the posterior aspect.
Anterior approach
The bladder is filled with 100 cc of saline to help with the identification of the frontal bladder wall. To enter Retzius' space, the peritoneum is incised at the anterior flexion just above the bladder between both medial umbilical ligaments by a semicircular incision using the electrocautery hook (Fig. 2). The urachus is divided as cranially as possible to avoid incidental bladder opening. The pubic bone is identified and the infrapubic fatty tissue removed to clear the endopelvic fascia and the puboprostatic ligaments. The superficial veins near the puboprostatic ligaments are carefully coagulated or clipped by the assistant. The endopelvic fascia is opened bilaterally under careful coagulation and the lateral aspect of the prostate is developed by gently removing the muscle fibers of the levator ani muscle. Lateral prostatic vessels are coagulated by the assistant using the bipolar grasper, then the puboprostatic ligaments are dissected. The notch between the venous plexus and the underlying urethra is visualized. The electrocautery hook is removed and replaced by a needle driver. The venous plexus is stitched twice with a 2/0 vicryl suture with a RB1 needle (Fig. 3). For better intra-abdominal handling all sutures should be shortened to a length of about 10–15 cm before use. The plexus is not dissected at this point.

Opening of the extraperitoneal space ventral to the urinary bladder

Ligation of the dorsal venous plexus with two needle holders
Bladder neck dissection
The prostate is pulled inferiorly with the help of the Foley catheter. The balloon of the Foley catheter helps identify the bladder neck. The plane between the prostate and the bladder is entered in the midline using the electrocautery hook. The bladder is opened at a comfortable distance from the prostate to avoid positive margins. After dissection of the anterior bladder wall the catheter is pulled up wards with a strong grasper and the incision of the bladder neck is continued laterally to both sides. When the opening of the bladder is large enough both ureteral ostiums are identified and the dorsal aspect of the bladder is dissected at a comfortable distance from the ostiums. After dissection of the posterior bladder wall, the already dissected ducts and the seminal vesicles are pulled through the opening and held upwards so that the lateral aspects of the bladder wall and the pedicles are clearly visible. The remaining sectors of the bladder wall and the pedicles on both sides are dissected in a descending manner using the cautery hook. However, if nerve sparing prostatectomy is performed, the neurovascular bundles are bluntly separated laterocaudally with scissors and small clips are used for hemostasis. The cautery hook is not used in these cases. The pedicles are dissected until the already identified musculus rectovesicalis is reached.
Apical dissection
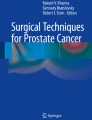
The venous plexus has already been ligated and is dissected at this point of the procedure. Hereafter, the prostate can be pushed downwards and the apex of the prostate becomes clearly visible. The anterior circumference of the urethra is divided with round tip scissors right at the prostatic apex (Fig. 4). The Foley catheter is pulled upwards and the dorsal aspect of the urethra is dissected with the scissors. In case of nerve sparing prostatectomy, the neurovascular bundles have to be separated from the urethra carefully (Fig. 4). Denonvillier's fascia and fibers of the rectourethral muscle are then divided to mobilize the prostate gland in an ascending manner under careful protection of the anterior rectal wall. An organ bag is inserted via one of the assistant trocars and the specimen is packed and parked in the mid abdomen. Now the prostate bed is inspected for bleeding and the rectal wall is checked.

View onto the urethral stump and the spared neurovascular bundles on both sides. Correct separation of the the dorsal urethra using a cold scissor
Anastomosis
For suturing the urethrovesical anastomosis both lateral da Vinci trocars are armed with needle drivers. The anastomosis is sutured with Vicryl 3/0 stitches (Fig. 5). The first stitch is positioned at the dorsal aspect of the bladder (6 o'clock position). The urethra is held upwards by the assistant with a metal uretheral dilator to avoid catching the opposing portion of the uretheral wall. Five to seven sutures follow in the same way to complete the anastomosis. The last stitch is done ventrally at 12 o'clock, after the Foley catheter has been inserted and its proper positioning is checked. The balloon is filled and the anastomosis is checked for leaks by filling the bladder with 100 ml of saline. A single Robinson drainage is inserted over the left assistant port and placed into the Rezius' space. After removal of the specimen bag, the midline minilaparotomy is closed by a fascia suture and intracutaneous stitches, while the other four trocar incisions are closed only by cutaneous stitches. All wounds are dressed.

Dorsal aspect of the anastomosis between urethra and bladder neck
Postoperative care
Postoperative care is similar to that for the open procedure. Pain medication is given intravenously or through a peridural-catheter. The drainage is removed when less than 50 ml/d is drained. On the seventh postoperative day, a cystography is performed to control the urethrovesical anastomosis for urinary leakage.
Discussion
We present here our experience with the remote controlled da Vinci Surgical System after performing 118 radical prostatectomies. Based upon our data, the remote control system could improve laparoscopic surgery in many ways: (1) dexterity of instrument handling, (2) additional grades of freedom (Endowrist technology), (3) excellent 3-D vision (InSite Vision System), (4) confortable positioning of the surgeon. However, to perform a safe radical prostatectomy with an optimal oncologic and functional result, the surgical technique needs to be adapted to the instrumental conditions. Although there are excellent methods for conventional laparoscopic radical prostatectomy that have been described by Guillonneau, Vallancien, Rassweiler and others [1, 3, 5, 6, 8, 10, 11, 12], no standarized surgical technique for robot assisted radical prostatectomy has been developed.
After performing 118 robot assisted radical prostatectomies using different surgical strategies, we conclude that the Montsouris technique with only minor adoptions (e.g. trocar placement and instrument use) seems to be optimal for performing robot assisted radical prostatectomy.
Applying this surgical method, we attained the following results in 81 robot assisted radical prostatectomies. The median age of the 81 patients was 63 years (range 45–75 years) and the median PSA was 8.96 ng/ml (range 1.5–40 ng/ml). A total of 55 (68.5%) of the tumors were organ confined (pT2), while 26 (31.5%) demonstrated capsula penetration (pT3). A positive margin was found in 18 of the 81 patients. Seven of these (12.7%) had organ confined (pT2) tumors and 11 (42%) pT3 tumors. The median estimated average blood loss was 300 ml (range 100–1,500 ml). The transfusion rate was 12% and one to two units of blood were transfused. The median operating time was 250 min (range 150–390 min). The median time of indwelling Foley catheter was 14 days (range 6–28 days).
All of these results are comparable with data from open as well as conventional laparoscopic radical prostatectomy. Therefore, robot assisted radical prostatectomy might become the operative strategy of the future.
References
Abbou C, Hoznek A, Salomon L. (1999) Laparoscopic radical prostatectomy. J Urol 161:17A
Binder J, Kramer W (2001) Point of technique: robotically-assisted laparoscopic radical prostatectomy. BJU International 87:1-4
Cacchione RN, Mungara A, De Turris S, Savino M Ferzli GS (2001) Laparoscopic prostatectomy. J Am Coll Surg 4:454–757
Dogan S, Aybek T, Westphal K, Mierdl S, Moritz A, Wimmer-Greinecker G (2001) Computer-enhance totally endoscopic sequential arterial coronary bypass. Ann Thorac Surg 72:610–611
Guillonneau B, Vallancien G (2000) Laparoscopic radical prostatectomy: the montsouris technique. J Urol 163:1643–1649
Guillonneau B, Cathelineau X, Barret E, Rozet F, Vallancien G (1999) Laparoscopic radical prostatectomy: technical and early oncological assessment of 40 operations. Eur Urol 36:14–20
Janatschek G, Marberger M (2000) Laparoscopic surgery in urology. Curr Opin Urol 10:351–357
Jewett MA (2002) Laparoscopic prostatectomy: here to stay. Can J Urol 1:14–17
Loulmet D, Carpentier A, d'Attellis N, Berrebi A, Cardon C, Ponzio O, Aupecle B, Relland JY (1999) Endoscopic coronary artery bypass grafting with the aid of robotic assisted instruments. J Thorac Cardiovasc Surg 118:4-10
Rassweiler J, Sentker L, Seemann (2000) Laparoscopic radical prostatectomy: technique and early experience. Akt Urol 31:237–245
Schulam PG, Link RE (2000) Laparoscopic radical prostatectomy. World J Urol 18:278–282
Turk I, Deger S, Winkelmann B, Schonberger B, Loening SA (2001) Laparoscopic radical prostatectomy. Technical aspects and experience with 125 cases. Eur Urol 40:46–52
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Wolfram, M., Bräutigam, R., Engl, T. et al. Robotic-assisted laparoscopic radical prostatectomy: the Frankfurt technique. World J Urol 21, 128–132 (2003). https://doi.org/10.1007/s00345-003-0346-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00345-003-0346-z