
Abstract
Objective
The long-term predictive value of the new proposed algorithm in the updated 2016 guidelines of the European Association of Cardiovascular Imaging to assess diastolic dysfunction (DD) in patients with heart failure with preserved ejection fraction (HFpEF) has not been validated.
Methods
The analysis included 451 patients who were diagnosed with HFpEF as confirmed via echocardiography. The endpoints were mortality and hospitalization for HF. The Kaplan–Meier curves and Cox regression models were generated to determine the risk of all-cause mortality based on the 2016 and 2009 DD grading algorithm, respectively. We evaluated the net reclassification index of outcomes on the basis of 2009 DD grade after abiding by the 2016 recommendations.
Results
After a follow-up of 2976 days, 119 patients (26.4%) died. According to the 2016 DD grading, grade III DD was associated with a significantly higher risk of mortality (hazard ratio [HR], 2.209; 95% CI 1.144–4.266) and HF hospitalization (HR, 2.047; 95% CI 1.348–3.870), as compared with grade I DD. Grade II DD was also associated with a higher risk of mortality (HR, 1.538; 95% CI 1.313–1.924). However, only grade III DD was independently associated with worse mortality based on 2009 DD grading. The net reclassification index for mortality increased significantly after grading by 2016 algorithm (10.6%, p < 0.001).
Conclusions
The 2016 DD grading algorithm showed improved prognostic value of long-term mortality in patients with HFpEF. Based on the findings of the study, the appropriate grading of DD is important in the prognostication of patients with HFpEF.
Key Points
• The application of the 2016 European Association of Cardiovascular Imaging recommendations diastolic dysfunction (DD) grading algorithm improves the predictive value for mortality.
• Our analysis suggests DD grades II and III based on 2016 guidelines is associated with poor outcomes as compared with grade I. The echocardiographic indices of the new algorithm should be obtained and applied to effectively evaluate DD.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
It has been reported that among the general heart failure population, over half have heart failure with preserved ejection fraction (HFpEF), and this prevalence has been on the rise in the aging population [1,2,3]. Some studies have even concluded that the morbidity associated with HFpEF (i.e., mainly the rate of hospitalization) is similar to that associated with systolic heart failure (SHF) [4]. The practical gold standard of grading of diastolic dysfunction (DD) is echocardiography, which has been recommended by major echocardiographic societies [5, 6]. The conventional diastolic function parameters including mitral inflow ratio, mitral inflow deceleration time, left atrium volume index (LAVI), and early transmitral velocity/tissue Doppler mitral annular early diastolic velocity (E/e’) have been applied to the grading of diastolic dysfunction and their prognostic importance has been proven in a variety of populations [7, 8]. Otherwise, more recent studies have emphasized the influence of right ventricular (RV) function, which is caused by both RV contractile impairment and afterload mismatch from pulmonary hypertension. Echocardiographic RV dysfunction is also considered to be the strongest predictor of mortality [9]. The latest recommendations for the evaluation of LV diastolic function from the American Society of Echocardiography (ASE) and the European Association of Cardiovascular Imaging (EACVI) suggest assessing the LV diastolic function grade using the aforementioned parameters plus peak tricuspid regurgitation (TR) jet [10]. Whether these classifications are associated with long-term outcomes remains unknown. In addition, there was no study applying the newest recommendations to grade DD severity and investigate the prognostic value in an Asian cohort. In the current study, we followed an Asian cohort of patients with HFpEF and analyzed the long-term prognostic factors, including medication and other comorbidities. Additionally, we classified the patients into three groups according to their diastolic dysfunction grade on the basis of the 2009 and 2016 guideline recommendations [5, 10] and examined the prognostic value of these two different grading systems for the long-term survival and identification of major cardiovascular risks in patients with HFpEF.
Methods
Study subjects
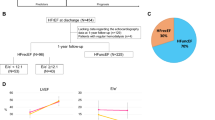
Subjects in this study were enrolled from registrants of the Taiwan Diastolic Heart Failure Registry (TDHFR) who were added from January 2008 to October 2016. Patients with a diagnosis of HFpEF (as defined in previous reports as well as by the consensus statement of the European Society of Cardiology) were enrolled from the TDHFR [6]. Details of the inclusion and exclusion criteria of TDHFR have been reported previously [11]. Patients who had renal failure, significant hepatic disease, secondary hypertension, pericardial disease, severe valvular heart disease, cancer, chronic obstructive pulmonary disease, and/or chronic atrial fibrillation were excluded. In order to exclude subjects with critically ill status or end-stage heart failure and ensuring stable outpatient follow-up, individuals who died or experienced cardiovascular events within 60 days after enrollment were also excluded. Finally, 451 patients from the TDHFR were enrolled in the current study. The algorithm was listed in Fig. 1.

Patient flow diagram. Asterisk indicates renal failure, significant hepatic disease, secondary hypertension, pericardial disease, severe valvular heart disease, cancer, chronic obstructive pulmonary disease, and/or chronic atrial fibrillation. E, early mitral inflow velocity; e’, early diastolic mitral annular velocity; LAVI, left atrium volume index; TR, tricuspid regurgitation
Demographic data were collected from the patients’ medical chart records. Hypertension was defined as a systolic blood pressure of ≥ 140 mmHg, a diastolic blood pressure of ≥ 90 mmHg, or the use of at least one class of antihypertensive agents. Non-insulin-dependent diabetes mellitus was defined as a fasting blood glucose concentration > 126 mg/dL and/or the use of at least one oral antihyperglycemic agent. Information regarding medications, such as the use of angiotensin-converting enzyme inhibitors (ACEI) and/or angiotensin II receptor blockers (ARB), calcium channel blockers (CCB), diuretics, nitrates, and/or beta-blockers, was also recorded.
Echocardiographic diastolic dysfunction grade
Subjects were divided into normal diastolic function and other three DD groups according to their grade, as newly proposed by ASE and EACVI in 2016 [10]. Owing to the lack of invasive hemodynamic investigation, indeterminate diastolic function based on 2016 algorithm was considered normal. Therefore, the normal diastolic function was defined as subjects who only meet one or two of the four criteria, i.e., (1) average E/e’ > 14, (2) septal e’ velocity < 7 cm/s or lateral e’ velocity < 10 cm/s, (3) TR velocity > 2.8 m/s, and (4) LAVI > 34 mL/m2(Fig. 1). The 2016 DD grade was evaluated using several parameters including the ratio of mitral inflow velocity to mitral peak velocity of late filling (E/A), peak E velocity, peak velocity of TR jet, medial and lateral e’, E/e’ ratio, and LAVI.
Likewise, subjects with septal e’ ≥ 8 or lateral e’ ≥ 10 and LAVI < 34 mL/m2 were classified as normal diastolic function group according to the 2009 DD grading recommendation [5]. The rest of the subjects were divided into three groups with different grades of DD (Fig. 1). Certain different echocardiographic parameters were evaluated, including deceleration time (DT), difference between the duration of atrial reversal velocity and mitral A-wave (Ar-A), and isovolumetric relaxation time (IVRT).
Endpoints
The primary outcome of this study was defined as all-cause mortality and hospitalization for heart failure.
Follow-up
The follow-up period ended on December 31, 2017. All of the patients visited our outpatient clinic at least every 3 months; otherwise, they were interviewed by telephone annually. All of the patients were carefully followed up. Information regarding the primary and secondary study outcomes was documented in chart records and/or via telephone interviews. For each patient, the time to death or cardiovascular event(s) was calculated from the initial date of diagnosis of HFpEF to the date on which the primary or secondary outcome occurred.
Statistical analysis
Data is expressed either as mean ± SD or as frequencies and/or percentages. To enable a comparison of the baseline characteristics between the three groups of different diastolic dysfunction grades, we performed one-way analysis of variance or Kruskal–Wallis test for continuous variables and the χ2 test or Fisher’s exact test for categorical variables, as appropriate. Then, for double comparison, the post hoc pairwise t test was used which was corrected for multiple testing by the Bonferroni correction. We firstly performed a univariate Cox regression analysis to examine the factors associated with all-cause mortality and HF hospitalization. Predictors in the multiple Cox model were selected from the set of variables that reached statistical significance in the univariate analysis via a forward selection procedure, with the significance limit to enter the model set at 0.05. The survival time was defined as the duration between enrollment and the occurrence of an event (defined as either a primary or secondary endpoint). Survival curves were estimated using the Kaplan–Meier method while the log-rank test was used to compare survival differences. Using grade I group as the reference, multivariate Cox’s proportional hazard regression analyses were performed to derive the adjusted HRs for the risk of outcomes in the different groups. We adjusted for age, sex, comorbidities (hypertension, diabetes, hyperlipidemia, coronary artery disease [CAD], and renal failure), medication usage, left ventricle mass index (LVMI), and LAVI. The incremental discriminatory ability of application of the 2016 guideline for predicting mortality and HF hospitalization above the 2009 guideline was evaluated with net reclassification index [12]. The 95% confidence interval (CI) of net reclassification index was calculated as well [12]. A receiver operating characteristic (ROC) curve and Harrel’s C statistic were constructed to assess the prognostic accuracy of 2016 and 2009 DD grading algorithms. In addition, 95% CI of these C statistics were calculated by the “somersd” package in STATA [13]. Statistical analysis was performed using IBM SPSS Statistics version 21.0 (IBM) and STATA version 14 (StataCorp LP). Two-sided p values < 0.05 were considered statistically significant.
Results
Baseline characteristics
Overall, 451 patients with HFpEF were enrolled in the present study. The median follow-up period was around 8 years (median 2976 days, mean 3012 ± 512 days). Patients were classified into normal diastolic function and three DD groups according to 2016 DD grades, and their baseline characteristics and echocardiographic and clinical data are presented in Table 1. The most common comorbidity was hypertension (65%), which is consistent with previous studies on diastolic heart failure. On the other hand, patients with diastolic dysfunction grade II (n = 308) or grade III (n = 37) in this study were found to be significantly older and predominantly female, compared with those with grade I (n = 66). Furthermore, patients with more advanced DD were more likely to have other cardiovascular-associated risks, including hypertension, diabetes, hyperlipidemia, and CAD. The renal function was normal and there was no difference among the four groups. While there was missing data of pro-BNP in 107 (23%) patients, the overall pro-BNP was high in our cohort (3653 ± 161 pg/mL). Subjects with grade III DD had significantly increased pro-BNP than those with grade I and II. The most common medications used were diuretics (52%); 35% of patients had been prescribed ACEI or ARB and approximately 46% of patients were taking beta-blockers or CCB. Notably, up to 80% of patients with DD grade III were taking diuretic agents, reflecting elevated left atrial pressure (LAP) and a greater frequency of congestive symptoms. In general, patients with diastolic dysfunction had an intact LV ejection fraction of > 60%. With regard to other echocardiographic findings, patients with advanced DD showed significantly higher early mitral inflow velocity (E) and E/E’, E/A ratios, and tricuspid regurgitation pressure gradient (TRPG). In terms of cardiac size, there was no difference in left ventricular mass index, but large LA size was noted in patients with grade III DD (Table 1).
2009 and 2016 DD grades and other clinical risk factors as predictors of outcomes
Table 2 summarizes the factors associated with mortality and HF hospitalization, as determined via univariate and multivariate analyses. The 2016 DD grade was an independent predictor of both mortality (p = 0.038) and HF hospitalization (p = 0.006), whereas the 2009 DD grade was not. Additional parameters associated with mortality were older age, hypertension, and LAVI. Likewise, those parameters plus diabetes were associated with HF hospitalization.
DD grade and outcomes
After approximately a median of 2976 days of follow-up, 119 patients (26.4%) experienced mortality with an incidence of 29 events per 1000 patient-years, and 93 patients (20.6%) experienced HF hospitalization with an incidence of 27 events per 1000 patient-years (Table 3). Compared with the 2009 classification of DD grades, a greater number of patients were reclassified into DD grade II according to the 2016 recommendation.
After controlling for the influence of age, sex, comorbidities (hypertension, diabetes, hyperlipidemia, CAD, and renal failure), medications, LVMI, and LAVI on mortality and HF hospitalization, multivariate Cox analysis demonstrated that in comparison with patients with DD grade I, patients with DD grade III were associated with a higher risk of mortality (hazard ratio [HR] = 1.806, 95% CI = 1.554–2.982) and HF hospitalization (HR = 2.103, 95% CI = 1.099–3.982) when they were classified according to the 2009 DD grade recommendation. Likewise, patients with DD grade III were associated with higher mortality (HR = 2.209, 95% CI = 1.144–4.266) and HF hospitalization (HR = 2.047, 95% CI = 1.348–3.870) when they were reclassified according to the 2016 DD grade recommendation (Table 3). When comparing patients with DD grades I and II, no difference was found in the risks of HF hospitalization regardless of whether the 2009 or 2016 recommendation was applied. However, according to 2016 recommendation, patients with DD grade II were associated with higher risk of mortality (HR = 1.538, 95% CI = 1.313–1.924) than those with grade I, while there was no difference in mortality risk between the two according to the 2009 recommendation (HR = 1.109, 95% CI = 0.627–1.963) (Table 3). On the other hand, treated subjects with normal diastolic function as the reference group, those with grade II and III DD, were associated with increased risk of mortality based on 2016 recommendations while only subjects with grade III DD remained as the finding based on 2009 recommendations. Nevertheless, there was significantly higher risk of HF hospitalization among subjects with grade I to grade III DD based on 2016 recommendations and subjects with grade III DD based on 2009 recommendations when compared with those with normal diastolic function (Supplement Table 1).
In the Kaplan–Meier analysis, patients with DD grade III showed higher mortality (log-rank p < 0.001) (Fig. 2a) as compared with those in DD grade I according to both the 2016 and 2009 algorithms. Notably, according to the 2016 DD grade, patients with grade II DD still experienced higher mortality than those with grade I, while there was no difference according to the 2009 DD grade (Fig. 2b).

Kaplan–Meier analysis of mortality according to: 2016 DD grade (a) and 2009 DD grade (b). DD, diastolic dysfunction
Net reclassification index and receiver operating characteristic curve
We treated the classification of DD grade based on the 2009 guideline as reference and reclassified our cohort in accordance with the 2016 guideline. The resultant net reclassification index was significant for mortality (index = 0.106, 95% CI = 0.057–0.192, p = 0.006) but not for HF hospitalization (index = 0.029, 95% CI = 0.014–0.091, p value = 0.24). A complete overview is shown in Table 4. In view of the ROC curves based on the 2009 and 2016 DD grade in predicting mortality, the difference between the areas under the curves (AUC) reached statistical significance (2016 DD grade AUC = 0.645 vs. 2009 DD grade AUC = 0.573, p = 0.02). On the other hand, there was no difference between the AUC in the prediction of HF hospitalization (2016 DD grade AUC = 0.573 vs. 2009 DD grade AUC = 0.558, p = 0.22). In multivariate analyses, the application of the latest 2016 DD grading algorithm resulted in incremental improvement in the predictive performance for mortality (Harrel C statics, 0.667 vs. 0.714; p = 0.012 for 2009 algorithm vs. 2016 algorithm) but not for HF hospitalization (Harrel C statics, 0.674 vs. 0.658; p = 0.012 for 2009 algorithm vs. 2016 algorithm) (Supplemental Table 2).
Discussion
In the present study, the prognostic value of the 2009 and 2016 DD grading recommendations was compared, and the 2016 recommendation was validated independently and externally for the relation between DD grade and outcomes. The important findings are the 2016 grading algorithm downward reclassified nearly half subjects with grade III DD based on 2009 algorithm and better-identified subjects with grade II DD independently associated with higher risk of mortality. To the best of our knowledge, this is the first study to verify and compare the usefulness of the 2009 and 2016 DD grading systems in predicting mortality and HF hospitalization in patients with HFpEF after adjustment for simple clinical, demographic, and echocardiographic variables [14].
Prior studies have varied in characterizing the degree of risk of mortality according to the stage of DD. As compared with normal diastolic function, there was no significant association between diastolic function and outcomes in the I-PRESERVE trial [15]. And a number of cohorts demonstrated increased risk of mortality associated even with mild DD [7, 16]. Nevertheless, the majority of studies reported patients with moderate and severe DD independently conferred higher mortality risk as compared with those with normal or mild DD [8, 17, 18]. The severity of DD was identified based on 2009 algorithm or previous classification criteria, which often-used echocardiographic variables were the E/A and E/e’ ratios. In our analysis, based on the 2016 DD algorithm, we observed subjects with grade III DD are associated with a significantly higher risk of mortality as compared with those with grade I according to both DD grading algorithms, which was consistent with the restrictive pattern of DD associated with poor outcomes [8, 16]. The prognostic markers identified in our study are consistent with the previously published literature, including age, male gender, hypertension, and diabetes [17, 19]. In respect of echocardiographic indices, our analyses showed that LAVI, but not the 2009 DD grade, was independently associated with poor outcomes, which was also reported in the subanalysis of the I-PRESERVE trial [15]. The presence of moderate or severe DD based on 2016 grading algorithm was associated with increased risk of mortality and MACE in our analysis. The application of 2016 recommendation to reclassify the DD grade above the 2009 recommendation improved two metrics used to determine the ability for mortality: the net reclassification index and AUC for ROC curve. The AUC showed higher predictive value of 2016 recommendation than that of the 2009 DD grade, though it was modest overall for both grading systems. While the differences in the AUC are marginal, applying the 2016 recommendation showed a 10% increased net reclassification index for mortality. Based on the 2016 recommendation, the survival analysis showed the subjects with grade II DD was significantly associated with mortality as compared with grade I DD while there was no significant increased risk based on the 2009 recommendation. Therefore, our results demonstrated the newly proposed algorithm could provide superior predictive ability for mortality.
In our analysis, a part of subjects with grade I DD based on 2009 recommendation was reclassified into grade II DD according to the 2016 recommendation. The possible explanation was the addition of evaluation of TRPG in the new grading algorithm. In previous evaluations of DD, including the 2009 DD grading system, the severity of DD was only assessed by the pattern of mitral inflow and tissue Doppler image. In the 2016 algorithm for determining grade II DD, the evaluation criteria included peak velocity of TR jet, E/e’, and LAVI as an E/A ratio < 0.8 along with a peak E velocity of > 50 cm/s or an E/A ratio > 0.8, but < 2. Elevation of these three parameters suggests grade II DD with increased left atrium pressure. In particular, increased peak velocity of TR jet indicates elevation of TRPG, pulmonary artery systolic pressure, pulmonary capillary wedge pressure, and in turn, left ventricular filling pressure [20]. Elevated TRPG and PASP also suggest pulmonary hypertension, which is common and associated with mortality in HFpEF [21].
Emerging evidence has shed light on the prognostic importance of right ventricle dysfunction or afterload in patients with HFpEF, which is assessed via right ventricular catheterization as well. The presence of right ventricle dysfunction is associated with increased mortality and heart failure hospitalization rates [9, 22]. Abnormality of coupling between right ventricle contraction and pulmonary circulation indicated worse outcomes [23]. Furthermore, several studies demonstrated that pulmonary capillary wedge pressure (PCWP) but not LV end-diastolic pressure was associated with mortality in HFpEF [24]. The 2009 and 2016 DD grading algorithms both emphasize the measurement of mitral inflow velocities in order to estimate LAP. Regarding the 2016 algorithm, the addition of peak velocity of TR jet to evaluate the right ventricle afterload and PCWP of 2016 DD grading algorithm could refine the risk stratification. The use of echocardiography to evaluate DD is a non-invasive application of the new algorithm to grade DD that provides prognostic information in most patients with HFpEF.
In respect of HF hospitalization, there was no difference of risk of HF hospitalization in patients with grade II or III DD compared with grade I DD irrespective of 2009 and 2016 algorithms. Diuretics are the major decongestive therapy to rapidly attain stable euvolemic status of patients with acute decompensation. Our cohort showed significantly more prevalent use of diuretics in patients with grade III DD. As a result, it may prevent further HF hospitalization after physicians increased the dose of diuretics according to echo results. However, there was significantly increased risk of HF hospitalization when compared with the normal group (Supplemental Table 1). Of note, even patients with grade I DD according to 2016 algorithm had higher risk of HF hospitalization when compared with those with normal diastolic function. However, only patients with grade III DD had higher risk of HF hospitalization when applying 2009 DD grading algorithm. Compared with 2009 algorithm, the latest 2016 algorithm could more efficiently and reliably estimate the increased LV filling pressure, usually preceding clinical congestion [25, 26]. Therefore, physicians were able to increase the dose of diuretics owing to more advanced DD grade and severe congestive symptoms. On the other hand, applying the 2016 grading algorithm could more accurately classify and diagnose patients with advanced DD, especially for those patients previously classified with grade I DD according to 2009 algorithm [27, 28]. Our results showed higher value of pro-BNP of subjects with advanced DD stage and significantly increased NRI, which were consistent with the aforementioned studies and previous observations [29,30,31]. Furthermore, our findings demonstrate the latest 2016 DD grading algorithm possess better prognostic ability for mortality, which really matters in the long-term follow-up.
Study limitations
Our study had several limitations. First, there was a certain proportion of data missing among some patients during the decade of follow-up. Some limitations of our study also arose from the type of data (i.e., registry-derived) that we analyzed. On the other hand, the lack of the invasive hemodynamic investigation made the classification of DD difficult when echocardiographic indices were incomplete or ambiguous. Moreover, the comparison between different DD evaluation algorithms is limited due to the small numbers of outcomes. Second, echocardiography was not systematically performed on the index date. Although the Doppler tissue image, LAVI, and peak TR velocity were recorded, some indices were not fully evaluated, including regional wall motion abnormality, the function of right heart, and LV strain. Third, in line with current the recommendations, we adopted ejection fraction (EF) ≥ 50% as the cut-off value to diagnose HFpEF, but the laboratory data were lacking [24]. We also excluded patients with HF and borderline ejection fraction (40–50%). Fourth, the referral bias of a hospital-based study cannot be eliminated because our hospital is a tertiary center. The restriction of the study to include hospitalized patients might have introduced a bias, since the results from this population may not reflect larger trends in disease prevalence in the community.
Conclusion
The recommendations for the 2016 DD grading system are based on expert consensus and have not yet been validated [10]. Our study is the first to evaluate the prognostic value of the algorithm with respect to outcomes among Asian patients with preserved ejection fraction. The present study shows that the 2016 DD grading algorithm significantly improves the classification of DD patients at higher risk of mortality. The non-invasive assessment of LAP is the premise of the algorithm and it correlated well with clinical symptoms and outcomes. Hence, the echocardiographic indices of the new algorithm should be obtained and applied to effectively evaluate DD.
Abbreviations
- ACEI:
-
Angiotensin-converting enzyme inhibitors
- ARB:
-
Angiotensin II receptor blockers
- ASE:
-
American Society of Echocardiography
- CCB:
-
Calcium channel blockers
- CI:
-
Confidence interval
- DD:
-
Diastolic dysfunction
- EACVI:
-
European Association of Cardiovascular Imaging
- HFpEF:
-
Heart failure with preserved ejection fraction
- HR:
-
Hazard ratio
- I-PRESERVE:
-
Irbesartan in Heart Failure With Preserved Ejection Fraction
- LAP:
-
Left atrial pressure
- LAVI:
-
Left atrium volume index
- LVDD:
-
Left ventricular diastolic dysfunction
- MACE:
-
Major cardiovascular events
- NYHA:
-
New York Heart Association
- PCWP:
-
Pulmonary capillary wedge pressure
- ROC:
-
Receiver operating characteristic
- RV:
-
Right ventricular
- SHF:
-
Systolic heart failure
- TDHFR:
-
Taiwan Diastolic Heart Failure Registry
- TR:
-
Tricuspid regurgitation
- TRPG:
-
Tricuspid regurgitation pressure gradient
References
Owan TE, Hodge DO, Herges RM, Jacobsen SJ, Roger VL, Redfield MM (2006) Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med 355:251–259
Zile MR (2003) Heart failure with preserved ejection fraction: is this diastolic heart failure? J Am Coll Cardiol 41:1519–1522
Wu CK, Lee JK, Chiang FT et al (2014) Prognostic factors of heart failure with preserved ejection fraction: a 12-year prospective cohort follow-up study. Int J Cardiol 171:331–337
Vasan RS, Larson MG, Benjamin EJ, Evans JC, Reiss CK, Levy D (1999) Congestive heart failure in subjects with normal versus reduced left ventricular ejection fraction: prevalence and mortality in a population-based cohort. J Am Coll Cardiol 33:1948–1955
Nagueh SF, Appleton CP, Gillebert TC et al (2009) Recommendations for the evaluation of left ventricular diastolic function by echocardiography. J Am Soc Echocardiogr 22:107–133. https://doi.org/10.1016/j.echo.2008.1011.1023
Paulus WJ, Tschope C, Sanderson JE et al (2007) How to diagnose diastolic heart failure: a consensus statement on the diagnosis of heart failure with normal left ventricular ejection fraction by the Heart Failure and Echocardiography Associations of the European Society of Cardiology. Eur Heart J 28:2539–2550
Redfield MM, Jacobsen SJ, Burnett JC Jr, Mahoney DW, Bailey KR, Rodeheffer RJ (2003) Burden of systolic and diastolic ventricular dysfunction in the community: appreciating the scope of the heart failure epidemic. JAMA 289:194–202
Halley CM, Houghtaling PL, Khalil MK, Thomas JD, Jaber WA (2011) Mortality rate in patients with diastolic dysfunction and normal systolic function. Arch Intern Med 171:1082–1087. https://doi.org/10.1001/archinternmed.2011.1244
Melenovsky V, Hwang SJ, Lin G, Redfield MM, Borlaug BA (2014) Right heart dysfunction in heart failure with preserved ejection fraction. Eur Heart J 35:3452–3462. https://doi.org/10.1093/eurheartj/ehu3193
Nagueh SF, Smiseth OA, Appleton CP et al (2016) Recommendations for the evaluation of left ventricular diastolic function by echocardiography: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr 29:277–314. https://doi.org/10.1016/j.echo.2016.1001.1011
Wu CK, Wang YC, Lee JK et al (2014) Connective tissue growth factor and cardiac diastolic dysfunction: human data from the Taiwan diastolic heart failure registry and molecular basis by cellular and animal models. Eur J Heart Fail 16:163–172
Pencina MJ, D'Agostino RB Sr, D'Agostino RB Jr, Vasan RS (2008) Evaluating the added predictive ability of a new marker: from area under the ROC curve to reclassification and beyond. Stat Med 27:157–172 discussion 207-112
Newson RB (2010) Comparing the predictive powers of survival models using Harrell’s C or Somers’ D. Stata J 10:339–358
Komajda M, Carson PE, Hetzel S et al (2011) Factors associated with outcome in heart failure with preserved ejection fraction: findings from the Irbesartan in Heart Failure with Preserved Ejection Fraction Study (I-PRESERVE). Circ Heart Fail 4:27–35
Zile MR, Gottdiener JS, Hetzel SJ et al (2011) Prevalence and significance of alterations in cardiac structure and function in patients with heart failure and a preserved ejection fraction. Circulation 124:2491–2501
Bella JN, Palmieri V, Roman MJ et al (2002) Mitral ratio of peak early to late diastolic filling velocity as a predictor of mortality in middle-aged and elderly adults: the Strong Heart Study. Circulation 105:1928–1933. https://doi.org/10.1161/CIRCULATIONAHA.2110.011031
Persson H, Lonn E, Edner M et al (2007) Diastolic dysfunction in heart failure with preserved systolic function: need for objective evidence: results from the CHARM Echocardiographic Substudy-CHARMES. J Am Coll Cardiol 49:687–694
Aljaroudi W, Alraies MC, Halley C et al (2012) Impact of progression of diastolic dysfunction on mortality in patients with normal ejection fraction. Circulation 125:782–788. https://doi.org/10.1161/CIRCULATIONAHA.1111.066423
Jones RC, Francis GS, Lauer MS (2004) Predictors of mortality in patients with heart failure and preserved systolic function in the Digitalis Investigation Group trial. J Am Coll Cardiol 44:1025–1029
Bouchard JL, Aurigemma GP, Hill JC, Ennis CA, Tighe DA (2008) Usefulness of the pulmonary arterial systolic pressure to predict pulmonary arterial wedge pressure in patients with normal left ventricular systolic function. Am J Cardiol 101:1673–1676. https://doi.org/10.1016/j.amjcard.2008.1601.1054
Lam CS, Roger VL, Rodeheffer RJ, Borlaug BA, Enders FT, Redfield MM (2009) Pulmonary hypertension in heart failure with preserved ejection fraction: a community-based study. J Am Coll Cardiol 53:1119–1126. https://doi.org/10.1016/j.jacc.2008.1111.1051
Mohammed SF, Hussain I, AbouEzzeddine OF et al (2014) Right ventricular function in heart failure with preserved ejection fraction: a community-based study. Circulation 130:2310–2320. https://doi.org/10.1161/CIRCULATIONAHA.2113.008461
Guazzi M, Dixon D, Labate V et al (2017) RV contractile function and its coupling to pulmonary circulation in heart failure with preserved ejection fraction: stratification of clinical phenotypes and outcomes. JACC Cardiovasc Imaging 10:1211–1221. https://doi.org/10.1016/j.jcmg.2016.1212.1024
Mascherbauer J, Zotter-Tufaro C, Duca F et al (2017) Wedge pressure rather than left ventricular end-diastolic pressure predicts outcome in heart failure with preserved ejection fraction. JACC Heart Fail 5:795–801. https://doi.org/10.1016/j.jchf.2017.1008.1005
Lancellotti P, Galderisi M, Edvardsen T et al (2017) Echo-Doppler estimation of left ventricular filling pressure: results of the multicentre EACVI Euro-Filling study. Eur Heart J Cardiovasc Imaging 18:961–968. https://doi.org/10.1093/ehjci/jex1067
Balaney B, Medvedofsky D, Mediratta A et al (2018) Invasive validation of the echocardiographic assessment of left ventricular filling pressures using the 2016 diastolic guidelines: head-to-head comparison with the 2009 guidelines. J Am Soc Echocardiogr 31:79–88. https://doi.org/10.1016/j.echo.2017.1009.1002
Almeida JG, Fontes-Carvalho R, Sampaio F et al (2018) Impact of the 2016 ASE/EACVI recommendations on the prevalence of diastolic dysfunction in the general population. Eur Heart J Cardiovasc Imaging 19:380–386. https://doi.org/10.1093/ehjci/jex1252
Sanchis L, Andrea R, Falces C, Poyatos S, Vidal B, Sitges M (2018) Differential clinical implications of current recommendations for the evaluation of left ventricular diastolic function by echocardiography. J Am Soc Echocardiogr 31:1203–1208. https://doi.org/10.1016/j.echo.2018.1208.1011
Wu CK, Su MY, Lee JK et al (2015) Galectin-3 level and the severity of cardiac diastolic dysfunction using cellular and animal models and clinical indices. Sci Rep 5:17007. https://doi.org/10.1038/srep17007
Wu CK, Lee JK, Chiang FT et al (2011) Plasma levels of tumor necrosis factor-α and interleukin-6 are associated with diastolic heart failure through downregulation of sarcoplasmic reticulum Ca2+ ATPase. Crit Care Med 39:984–992. https://doi.org/10.1097/CCM.0b013e31820a91b9
Wu CK, Tsai HY, Su MM et al (2017) Evolutional change in epicardial fat and its correlation with myocardial diffuse fibrosis in heart failure patients. J Clin Lipidol 11:1421–1431. https://doi.org/10.1016/j.jacl.2017.08.018
Funding
This work was supported, in part, by the IBMS CRC Research Program of Institute of Biomedical Science, Academia Sinica (IBMS-CRC99-P02), and grants (NSC 99-2314-B-002-131-MY3, NSC 100-2341-B-002-160-) from the National Science Council of R.O.C.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Guarantor
The scientific guarantor of this publication is Dr. Cho-Kai Wu.
Conflict of interest
The authors of this manuscript declare no relationships with any companies, whose products or services may be related to the subject matter of the article.
Statistics and biometry
No complex statistical methods were necessary for this paper.
Informed consent
Written informed consent was obtained from all subjects (patients) in this study.
Ethical approval
Institutional Review Board approval was obtained.
Methodology
• Prospective
• Observational
• Performed at one institution
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
ESM 1
(DOCX 23 kb)
Rights and permissions
About this article

Cite this article
Lin, TT., Wang, YC., Juang, JM.J. et al. Application of the newest European Association of Cardiovascular Imaging Recommendation regarding the long-term prognostic relevance of left ventricular diastolic function in heart failure with preserved ejection fraction. Eur Radiol 30, 630–639 (2020). https://doi.org/10.1007/s00330-019-06261-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-019-06261-1