
Abstract
In computed tomography(CT) several contrast media with different iodine concentrations are available. The aim of this study is to prospectively compare contrast media with iodine concentrations of 300, 370 and 400 mg iodine/ml for chest- CT. 300 consecutive patients were prospectively enrolled, under a waiver of the local ethics committee. The first (second, third) 100 patients, received contrast medium with 300(370, 400)mg iodine/ml. Injection protocols were adapted for an identical iodine delivery rate(1.3 mg/s) and total iodine load(33 g) for all three groups. Standardized MDCT of the chest (16 × 0.75 mm, 120 kVp, 100 mAseff.) was performed. Intravascular attenuation values were measured in the pulmonary trunk and the ascending aorta; subjective image quality was rated on a 3-point-scale. Discomfort during and after injection was evaluated. There were no statistically significant differences in contrast enhancement comparing the three contrast media at the pulmonary trunk(p = 0.3198) and at the ascending aorta(p = 0.0840). Image quality(p = 0.0176) and discomfort during injection(p = 0.7034) were comparable for all groups. General discomfort after injection of contrast media with 300 mg iodine/ml was statistically significant higher compared to 370 mg iodine/ml(p = 0.00019). Given identical iodine delivery rates of 1.3 g/s and iodine loads of 33 g, contrast media with concentrations of 300, 370 and 400 mg iodine/ml do not result in different intravascular enhancement in chest-CT.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
With the introduction of rapid multi-detector row spiral computed tomography (MDCT) the timing and planning of the application of contrast media became more crucial. Arterial contrast enhancement is determined by patient-related factors (e.g. blood volume, cardiac output) as well as by contrast injection parameters (e.g. contrast material concentration, contrast material volume, flow rate, added saline chaser bolus) [1–4]. Contrast media with different iodine concentrations are available on the market and numerous different injection protocols have been proposed. Intravascular or parenchymal enhancement is clearly affected by all major parameters of the injection protocol applied, including the total volume of contrast material, the iodine concentration, the injection rate and accordingly the duration of injection [1–3, 5–13]. Different contrast material volumes or flow rates also contrast media with different iodine concentrations have been compared [10, 14–23]. Some studies reported that intravenous administration of contrast media with high iodine concentration yields higher intravascular and parenchymal attenuation than contrast media with a lower iodine concentration [16, 17, 19, 21, 22]. Up to date, no wide consensus on the optimum contrast medium concentration for the different types of examination in MDCT scanning has been reached. One major drawback of most of the published studies, however, is that comparing contrast media with different iodine concentrations and applying identical injection flow rates (in ml per second) leads to unequal iodine delivery rates (in mg per second). As iodine is the main attenuation component of all current X-ray contrast agents, it is not a surprise that a higher iodine delivery rate leads to higher contrast enhancement. Moreover most of the papers published are either retrospective analyses or compare only two different concentrations of contrast media [16, 17, 19, 21, 22].
For a reliable comparison of contrast media with different iodine concentrations, an adapted injection protocol insuring an identical iodine delivery rate (in mg per second) and an identical total iodine load is mandatory. Adapting the iodine dose to the body weight and using a fixed injection duration Awai et al. found an increased enhancement in the abdominal aorta for contrast material with a lower concentration compared to a higher concentration [14]. In accordance to these finding Han et al. reported an increased contrast enhancement for a contrast medium with a lower concentration (150 mg iodine/ml) in comparison with a higher concentration (300 mg iodine/ml) given the same total iodine dose and iodine delivery rate in an animal study [10].
The aim of our study was to evaluate intravascular contrast enhancement, image quality and patient discomfort in routine chest CT examinations using different contrast media with iodine concentrations ranging from 300 to 400 mg iodine per ml, administered with an identical iodine delivery rate and an identical total iodine load. A prospective study design with a patient cohort of 300 consecutively enrolled individuals was chosen.
Materials and methods
Patient demographics
The study was performed under a waiver of the local ethics committee. Between October 2006 and November 2007 300 consecutive patients, who were scheduled for contrast-enhanced chest CT, were prospectively enrolled in this study. All patients signed an informed consent to participate. Exclusion criteria were general contraindications to iodinated contrast media, cardiac failure (stage NYHA IV) or the inability to place an 18 G i.v. needle in a cubital vein.
The leading indications for CT included bronchial cancer (n = 63) and lung metastasis (n = 35); the top 20 diagnoses of all patients are listed in Table 1. Additional patient demographics for all three groups are displayed in Table 2.
CT
All examinations were performed using a 16-slice multidetector-row CT system (SOMATOM Sensation 16; Siemens Medical Solutions, Forchheim, Germany). All patients were positioned supine and examined in cranio-caudal direction at end-inspiration. A standard chest CT protocol with a collimation of 16 × 0.75 mm, a table feed of 12 mm per rotation with a rotation time of 0.5 s was applied. An effective tube current-time product of 100 mAseff and a tube voltage of 120 kVp were chosen. Image reconstruction was performed using a medium-smooth soft tissue kernel (Siemens B30) at a slice thickness of 5 mm with an overlapping increment of 4 mm.
Contrast medium admininstration
The first 100 consecutive patients (Group A) received contrast material with 300 mg iodine per ml (Ultravist 300, Bayer Schering Pharma AG, Berlin, Germany), the second 100 patients (Group B) received contrast material with 370 mg iodine per ml (Ultravist 370) and the last 100 patients received contrast material with 400 mg iodine per ml (Imeron 400, Bracco ALTANA Pharma GmbH, Konstanz, Germany). Total contrast medium volume and Injection flow rate were adapted to ensure an identical iodine delivery rate of 1.3 mg/s and a total iodine load of 33 g for all three groups (Table 3), based on the standard protocol at our institution. Pre-heated contrast material (37°C) was applied intravenously via a 18 G syringe into an antecubital vein using a programmable dual head power injector (CT2; Medtron, Saarbruecken, Germany) and was followed by a 30 ml saline chaser injected at the same flow rate as the contrast medium.
For bolus timing the bolus tracking technique was applied: after a localization CT image, a region of interest (ROI) was placed in the pulmonary trunk and the threshold for initiation of the CT data acquisition was set to 140 Hounsfield Units (HU); the delay after the trigger, before the actual CT was initiated, was set to 5 seconds.
Image analysis and evaluation of patient discomfort
Intravascular contrast enhancement was measured in the pulmonary trunk and in the ascending aorta by placing circular regions of interest (ROI) on three adjacent slices at each anatomic site. At all anatomic sites a constant ROI-size of approximately 1.0 cm2 was maintained and visible artifacts (e.g. from beam hardening of pacemaker leads or contrast material in the superior vena cava) were excluded from the measurements. The measured attenuation values were averaged for further statistical analysis.
Subjective image quality was assessed on a 3-point-scale that is displayed in Table 4; for quality assurance of this scale an image gallery was created before the study. Image evaluation and all measurements were performed by a board certified radiologist.
After completion of the whole CT examination each patient was questioned by the radiology technician and local discomfort at the site of injection plus general discomfort after injection were rated by each patient on a scale from 0 (no discomfort) to 10 (worst imaginable discomfort).
Statistical analysis
Descriptive statistical analysis was done separately for the three different iodine concentrations. Demographic patient data (age, height, weight, BMI) as well as contrast enhancement values obtained at both anatomic sites (pulmonary trunk, ascending aorta) were summarized by arithmetic means and corresponding standard deviations (SD). Mean contrast enhancement values and according SD were compared graphically between the three iodine concentrations. Additionally the gender of the patients was documented and given as absolute frequencies of males and females. For the subjective scores (image quality, patient discomfort at side of injection, general discomfort) the median and the corresponding interquartile range (upper quartile – lower quartile) were computed.
One-way analysis of variance (one-way ANOVA) was used for comparison of age, height, weight, BMI as well as contrast enhancement values between the three patient groups. In case of a statistically significant test result in the corresponding global F-test, post-hoc t-tests were carried out for pair wise comparison of the three groups.
Male and female frequencies were compared between the three groups by applying Fisher’s exact test.
Results of the subjective scores were analyzed by use of the nonparametric Kruskal-Wallis test. If a statistically significant test result was observed, the Kruskal-Wallis test was followed by post-hoc unpaired Wilcoxon tests for pair wise comparison of the three groups.
A global significance level of α = 0.05 was chosen for all statistical test procedures conducted.
An α-adjustment was carried out using the Bonferroni correction method to account for the problem of multiple testing. According to this, due to the number of ten parameters evaluated and the number of three groups compared, p-values of p ≤ 0.005 in the global tests (one-way ANOVA, Fisher’s exact test, Kruskal-Wallis test) as well as p-values of p ≤ 0.00167 in the post-hoc tests can be regarded as statistically significant test results.
All statistical analyses were conducted using the SAS statistical analysis software package (SAS Version 9.1; SAS Institute, Cary, NC, USA).
Results
All 300 CT examinations could be completed without occurrence of any complications. The mean craniocaudal range (± SD) covered by CT was 322.4 ± 29.7 mm with a mean CT data acquisition time of 13.7 ± 1.5 seconds. Demographic patient data for all three groups is displayed in Table 2; No statistically significant differences between the three groups were observed with respect to gender, age, weight, height or body mass index (BMI).
The mean intravascular contrast enhancement (± SD) in the pulmonary trunk for group A (B and C) was 341.5 ± 114.6 (320.5 ± 99.5 and 338.9 ± 107.2) HU. Corresponding enhancement values measured in the ascending aorta were 275.7 ± 63.5 (290.8 ± 62.6 and 294.2 ± 60.5) HU (Fig. 1). No statistically significant differences in contrast enhancement values were found between the three groups both at the pulmonary trunk (p = 0.3198) and the ascending aorta (p = 0.0840) (Fig. 2).

Graphical comparison of contrast enhancement in the pulmonary trunk (TP) and the ascending aorta (AA) between all three groups (A-C) given as mean ± standard deviation

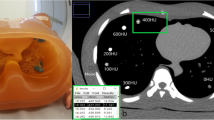
Three sample CT images at the level of the pulmonary trunk for group A (a), B (b) and C (c) demonstrating diagnostic image quality with comparable intravascular contrast enhancement for all different contrast media used. Note the bilateral lung tumor manifestation in (a) and the old posterior/lateral rib fracture on the right in (b)
The medians and interquartile ranges of the rated overall image quality were 1.0 and 0 for all three groups with diagnostic image quality for all 300 CT examinations. The Kruskal-Wallis test performed with respect to image quality revealed a p-value of 0.0176; given the applied Bonferroni correction this test result is statistically not significant. Evaluation of the patient discomfort at the site of injection revealed a median of 0 and an interquartile range of 0 in each of the three groups (p = 0.7034). The general discomfort after injection of contrast media was rated with a median of 1 and an interquartile range of 2 for group A whereas the general discomfort in group B and C was rated with a median of 0 and an interquartile range of 1 (p = 0.0003). Pair wise post-hoc Wilcoxon tests revealed a statistically significant difference in general discomfort only between group A and B (p = 0.00019) whereas comparison of group A and C (p = 0.0025) as well as group B and C (p = 0.3412) showed no statistically significant differences.
Discussion
As mentioned above, several studies comparing the influence of different iodine concentrations of contrast medium on vascular and parenchymal enhancement have already been performed comparing different injection protocols for various body regions [10, 14–23]. Most of these studies set their focus on parenchymal contrast enhancement in the abdomen. Only few studies focused on CT angiography injection protocols and surprisingly often low and high concentration contrast media are compared without adaptation of the iodine delivery rate, putting of course the higher concentrated products in favor for higher intravascular enhancement. Rist and Tsai investigated CT angiography protocols for coronary enhancement [20, 23]. Tsai et al. [23] compared iodine concentrations of 320 and 350 mg iodine per ml in 100 patients. As a drawback of this study no adaptation to ensure a constant iodine delivery rate for both contrast media was applied. However, no statistically significant different in intracoronary contrast enhancement was found, probably due to the only minor difference in iodine concentration and the relatively small sample size. In a prospective trial including 60 patients Rist et al. [20] adapted their injection protocol comparing contrast media with 300 and 400 mg iodine per ml to preserve an identical iodine delivery rate. In accordance with the findings of our study no statistically significant difference between the two contrast media was found with respect to intravascular enhancement. In a study comparing contrast media with 300 and 370 mg iodine per ml Setty et al. [19] adapted the total amount of iodine to the patients’ body weight without, however, ensuring an identical iodine delivery rate. Not surprisingly the contrast medium with higher concentration resulted in higher intravascular enhancement in the superior vena cava, the pulmonary artery, the pulmonary veins and the aorta. Awai at al. [14] explored contrast enhancement in the liver and the aorta comparing contrast media with 300 and 350 mg iodine per ml, making a proper adaptation of the iodine delivery rate. They observed even improved intravascular enhancement in the aorta for the iodine concentration of 300 mg/ml. A possible explanation for observing higher mean attenuation values for contrast media with lower iodine concentration especially in the early phase of CT data acquisition can be found in flow-characteristics based on differences in viscosity. The viscosity of contrast media exponentially increases with higher iodine concentration and can be decreased by elevation of the temperature. The viscosity of the contrast media used in our study with 300, 370 and 400 mg iodine per ml is 9.2, 22 and 27.5 mPa*s at 20°C. With preheating before injection, as done in our study, lower levels of viscosity for the three different concentrations 300, 370 and 400 mg iodine per ml can be reached: 4.9, 10 and 12.6 mPa*s at 37°C. A fluid with lower viscosity can be injected at a lower pressure and might distribute more easily and more evenly in the vessels. This phenomenon could explain the higher contrast enhancement in the early phase after contrast medium administration in the study by Awai et al. In our study, with preheating, injection flow rates of up to 4.3 ml/s and use of a saline chaser the viscosity did not relevantly influence flow dynamics.
One might argue that using low concentration contrast media higher injection flow rates, in order to preserve an identical iodine delivery rate in comparison to high concentration contrast media, are mandatory and might lead to an increased occurrence of extravasations or at least to increased discomfort of the patient at the site of injection during the mechanical injection. Only very few studies did evaluate the discomfort associated with application, and especially injector application, of different iodine containing contrast media [24–27]. Our results show no difference for all three contrast media used in terms of discomfort at the site of injection. Interestingly, however, the contrast medium with 300 mg iodine per ml showed an increased level of general discomfort after injection in comparison to the contrast medium with 370 mg iodine per ml; in direct comparison to the contrast medium with 400 mg/ms, however, no significant difference was found. One possible explanation for this might be the overall higher injection flow rate or injection volume applied when using a contrast medium with lower iodine concentration; overall volume differences between the different injection protocols used in our study account for up to 28 ml possibly leading to different levels of vessel dilatation in the afferent veins causing general discomfort.
One potential limitation of the data presented is the mono-centric setting of the study. A multi-center setting of course would have improved the impact of the study even more. Enrollment of 300 patients undergoing an exclusive contrast-enhanced chest CT, without additional CT imaging of the abdomen, neck or other body regions, took more than a year at our institution; an even larger patient collective could only be recruited in a multi-centre setting within a reasonable amount of time. Moreover, an intra-individual comparison between the different contrast media would have been more desirable than an inter-individual setting. However, prospective enrollment of 100 patients with three consecutive CT examinations would have been even more challenging. On the other hand the results of the study presented did not reveal any statistically significant differences in patient demographics between the three patient groups.
To our knowledge the study presented here is the first to investigate the properties of contrast media with three different iodine concentrations in a prospective setting with correction of the iodine delivery rate in a routine chest CT setting. The study design with prospective patient acquisition, a reasonably large number of individuals, no statistically significant differences between the three groups in terms of patient demographics and the performed Bonferroni correction for multiple testing do allow to propagate the findings of this study for the medical community.
In summary, comparison of contrast media with 300, 370 and 400 mg/ml iodine concentration did not lead to statistically significant differences in intravascular enhancement, image quality or discomfort at site of injection. The only difference identified was that general patient discomfort after injection was higher using a concentration of 300 compared to 370 mg iodine per ml but not compared to the 400 mg iodine per ml group.
References
Awai K, Hiraishi K, Hori S (2004) Effect of contrast material injection duration and rate on aortic peak time and peak enhancement at dynamic CT involving injection protocol with dose tailored to patient weight. Radiology 230:142–150
Heiken JP, Brink JA, McClennan BL, Sagel SS, Forman HP, DiCroce J (1993) Dynamic contrast-enhanced CT of the liver: comparison of contrast medium injection rates and uniphasic and biphasic injection protocols. Radiology 187:327–331
Heiken JP, Brink JA, McClennan BL, Sagel SS, Crowe TM, Gaines MV (1995) Dynamic incremental CT: effect of volume and concentration of contrast material and patient weight on hepatic enhancement. Radiology 195:353–357
Haage P, Schmitz-Rode T, Hubner D, Piroth W, Gunther RW (2000) Reduction of contrast material dose and artifacts by a saline flush using a double power injector in helical CT of the thorax. AJR Am J Roentgenol 174:1049–1053
Bae KT, Heiken JP, Brink JA (2000) Aortic and hepatic contrast medium enhancement at CT. Part II. Effect of reduced cardiac output in a porcine model. Radiology 207:657–662
Bae KT, Heiken JP, Brink JA (1998) Aortic and hepatic contrast medium enhancement at CT. Part I. Prediction with a computer model. Radiology 207:647–655
Bae KT, Heiken JP, Brink JA (1998) Aortic and hepatic peak enhancement at CT: effect of contrast medium injection rate–pharmacokinetic analysis and experimental porcine model. Radiology 206:455–464
Brink JA, Heiken JP, Forman HP, Sagel SS, Molina PL, Brown PC (1995) Hepatic spiral CT: reduction of dose of intravenous contrast material. Radiology 197:83–88
Brink JA (2003) Use of high concentration contrast media (HCCM): principles and rationale–body CT. Eur J Radiol 45(Suppl 1):S53–S58
Han JK, Kim AY, Lee KY et al (2000) Factors influencing vascular and hepatic enhancement at CT: experimental study on injection protocol using a canine model. J Comput Assist Tomogr 24:400–406
Fleischmann D (2003) Use of high-concentration contrast media in multiple-detector-row CT: principles and rationale. Eur Radiol 13(Suppl 5):M14–M20
Fleischmann D (2003) High-concentration contrast media in MDCT angiography: principles and rationale. Eur Radiol 13(Suppl 3):N39–N43
Fleischmann D (2003) Use of high concentration contrast media: principles and rationale-vascular district. Eur Radiol 45(Suppl 1):S88–S93
Awai K, Inoue M, Yagyu Y et al (2004) Moderate versus high concentration of contrast material for aortic and hepatic enhancement and tumor-to-liver contrast at multi-detector row CT. Radiology 233:682–688
Awai K, Takada K, Onishi H, Hori S (2002) Aortic and hepatic enhancement and tumor-to-liver contrast: analysis of the effect of different concentrations of contrast material at multi-detector row helical CT. Radiology 224:757–763
Cademartiri F, de Monye C, Pugliese F et al (2006) High iodine concentration contrast material for noninvasive multislice computed tomography coronary angiography: iopromide 370 versus iomeprol 400. Invest Radiol 41:349–353
Furuta A, Ito K, Fujita T, Koike S, Shimizu A, Matsunaga N (2004) Hepatic enhancement in multiphasic contrast-enhanced MDCT: comparison of high- and low-iodine-concentration contrast medium in same patients with chronic liver disease. AJR Am J Roentgenol 183:157–162
Sandstede JJ, Werner A, Kaupert C et al (2006) A prospective study comparing different iodine concentrations for triphasic multidetector row CT of the upper abdomen. Eur J Radiol 60:95–99
Setty BN, Sahani DV, Ouellette-Piazzo K, Hahn PF, Shepard JA (2006) Comparison of enhancement, image quality, cost, and adverse reactions using 2 different contrast medium concentrations for routine chest CT on 16-slice MDCT. J Comput Assist Tomogr 30:818–822
Rist C, Nikolaou K, Kirchin MA et al (2006) Contrast bolus optimization for cardiac 16-slice computed tomography: comparison of contrast medium formulations containing 300 and 400 milligrams of iodine per milliliter. Invest Radiol 41:460–467
Sultana S, Morishita S, Awai K et al (2003) Evaluation of hypervascular hepatocellular carcinoma in cirrhotic liver by means of helical CT: comparison of different contrast medium concentrations within the same patient. Radiat Med 21:239–245
Tsurusaki M, Sugimoto K, Fujii M, Sugimura K (2004) Multi-detector row helical CT of the liver: quantitative assessment of iodine concentration of intravenous contrast material on multiphasic CT–a prospective randomized study. Radiat Med 22:239–245
Tsai IC, Lee T, Tsai WL et al (2008) Contrast enhancement in cardiac MDCT: comparison of iodixanol 320 versus iohexol 350. AJR Am J Roentgenol 190:W47–W53
Valentine A, Jakobsen JA, Klaveness AJ (1997) Iopentol (Imagopaque 350) compared with diatrizoate (Urografin 370) in cerebral CT. A clinical trial assessing immediate and late (7 days) adverse events and diagnostic information (visualization quality and Hounsfield unit measurements). Eur Radiol 7(Suppl 4):S145–S148
Tytle T, Prati RC Jr., Azodo MV, Gutierrez O (1996) A prospective, parallel, double-blind comparison of iodixanol and iohexol in extremity phlebography. Acad Radiol 3(Suppl 3):S519–S523
Sundgren PC, Baath L, Tornquist C, Hougens Grynne B, Kjaersgaard P, Almen T (1996) Image quality and safety after iodixanol in intravenous urography; a comparison with iohexol. Br J Radiol 69:699–703
Tveit K, Bolz KD, Bolstad B et al (1994) Iodixanol in cardioangiography. A double-blind parallel comparison between iodixanol 320 mg I/ml and ioxaglate 320 mg I/ml. Acta Radiol 35:614–618
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Mühlenbruch, G., Behrendt, F.F., Eddahabi, M.A. et al. Which Iodine concentration in chest CT? – A prospective study in 300 patients. Eur Radiol 18, 2826–2832 (2008). https://doi.org/10.1007/s00330-008-1080-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-008-1080-0