
Abstract
Peripheral nerve tumors are not frequent, but due to their association with a nerve they are somewhat special. They may be encountered incidentally during evaluation of a soft-tissue mass or when a nerve lesion is clinically suspected and the recognition of such a lesion and its differential diagnosis is key for successful therapy and patient prognosis. As sonography is often the first line modality in the work-up of a soft-tissue mass, the sonographer should be aware of the typical features of such lesions in order to arrive at the correct diagnosis, and this article tries to give an overview of the histological subtypes of peripheral nerve tumors and their sonographic characteristics.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Sonography is often the first line modality used for the evaluation of a palpable soft-tissue mass. Its application for the diagnosis and characterization of peripheral nerve tumors dates back to the 1980s, when Hughes et al. [1] gave a systematic description of the sonographic appearance of peripheral nerve tumors. In general, the diagnosis of a peripheral nerve tumor is easily made if the continuity of a mass with a peripheral nerve is established. The differential diagnosis, however, may be difficult and relies on knowledge of the sonographic features related with the histopathologic structure of the individual lesion. This article gives an overview of the current concepts in sonography of peripheral nerve tumors.
Types of lesions
Among the possibly encountered benign and malignant peripheral nerve tumors are “pseudotumors” such as neuromas, as well as “true” tumors. Among the latter, we find lesions derived from nonspecific neural tissue, such as fibrolipoma, peripheral nerve sheath ganglion and intraneural perineurioma. The group of peripheral nerve sheath tumors (PNST) includes benign lesions deriving from specific neural tissue, such as neurolemoma (neurinoma, schwannoma), neurofibroma and rare forms such as the granular-cell tumor [2, 3]. Malignant peripheral nerve sheath tumors (MPNST) consist of malignantly transformed specific neural tissue intermixed with different amounts of non-neurogenic neoplastic material [3–5].
Sonographic technique
In recent years, a substantial amount of publications have documented the value of high-resolution ultrasound (HR-US) for peripheral nerve assessment in general [6–10]. Consequently HR-US is currently the modality of choice for the examination of superficially running nerves. Because of ongoing improvement in sonographic hardware and software technology (i.e., linear array transducers of up to 17 MHz, artifact reduction software, image compounding, etc.), sonography is now capable of depicting sub-millimeter structures with an unrivaled resolution. Thus, imaging of even small peripheral nerves and nerve tumors, and their ultrastructure became feasible [8, 11]. In addition to simple B-mode imaging, HR-US also allows for functional assessment of tumor vascularization by use of color Doppler and duplex mode [12].
Sonographic features of normal nerves
The detailed description of the sonographic ultrastructure of peripheral nerves can be found elsewhere [9, 11]. An important element for neural function and the sonographic appearance of a nerve are the Schwann cells. A bundle of axons and Schwann cells grouped by a common sheath of connective tissue (the epineurium) forms the so-called “nerve fascicle” and these fascicles can be depicted by HR-US as hypoechoic bands on longitudinal ultrasound scans and bundles of uniformly hypoechoic dots on a hyperechoic background on transverse scans. Echogenic connective tissue normally surrounds the individual fascicles, which gives the nerve an internal structure. However, a nerve may be entirely hypoechoic if connective tissue is only sparse (e.g., in nerve sections next to hypomochlia) [3, 6, 9, 11, 13, 14]. The terminal outer layer—the perineurium—combines several nerve fascicles to a peripheral nerve. It is embedded loosely in the surrounding tissue, which assures sufficient mobility of a nerve during joint motion. HR-US usually depicts the outer nerve sheath as a relatively sharp hyperechoic band.
Benign peripheral neurogenic tumors
Traumatic neuroma
During trauma the axons of a peripheral nerve can be completely or incompletely disrupted. Only hours after such an incident the distal axonal segments disintegrate (Waller degeneration), fragmented axonal material is removed by Schwann cells and macrophages and regional Schwann cells try to bridge the discontinuity [15, 16]. If this procedure fails, a disorganized, pseudotumor-like, growth of Schwann cells and misled axons follows. Macroscopically this results in a slowly growing nodule; i.e., neuroma formation. The growth of a neuroma is limited and stops after 1 year and its final size is directly related to the number of injured axons [2, 3].
In special cases—especially in traction injuries—a discontinuous interruption of the fascicular neural elements is found, with intraneural hypoechoic nodules at different levels (bead-like neuroma formation, “neuroma in continuity”). This situation is frequently found in the brachial plexus [16–19].
The same pathologic process is also responsible for neuroma development after nerve grafting. In this case a neuroma develops if complete continuity of the Schwann tubes is not achieved by surgery [17]. Clinically, neuromas present with a Tinel-Hoffmann sign, i.e., a local electrifying sensation provoked by palpation or tapping [13, 20].
On HR-US examinations traumatic neuromas are concentric bulbous lesions, mainly located at the distal end (“pollywog” appearance of terminal type) or along the course (lateral excentric type) of a traumatized nerve [3]. The neuroma appears homogenously hypoechoic, sometimes with small hyperechoic internal bands (Fig. 1a,b). No degenerative or necrotic, pseudocystic foci are found. Usually the outer border of a neuroma is sharp but it may be distorted by scar formation in the surrounding soft tissues [3, 16, 18, 21]. Duplex HR-US usually does not show any perfusion [16, 21–23].

a Typical terminal bulbous neuroma with a “pollywog” appearance (white arrowheads) in continuity to the ulnar nerve (white arrow) in a patient after amputation of the forearm. Some inner hyperechoic bands which represent intraneural connective tissue, are seen (black arrow). b: A chain of neuromatous nodules (black arrowheads) along the fibular nerve after traumatic amputation. In such a “neuroma in continuity” most neuromas are of the lateral excentric type with usually one neuroma of the terminal type at the blind end of the nerve
Morton’s neuroma
This pseudotumor is a form of localized perineural fibrosis and usually found in the second and third metatarsal interspace. Morton’s neuromas are located at the division of the common into the proper plantar digital nerves. They are very painful under load and are mainly found in middle-aged women [2, 3]. The exact reasons for the development of Morton’s neuroma are still unknown, but chronic nerve compression at the intermetatarsal ligament plays a key role. This biomechanical theory is supported by the correlation of Morton’s neuroma with chronic traumatic changes of neighboring tendon sheaths (thickening, occurrence of ganglia or fluid collections) [3].
On HR-US exams Morton’s neuroma usually presents as a homogeneous, hypoechoic concentric nodule, located in the plantar subcutis at the level of the metatarsal heads (Fig. 2). Some lesions are deformed due to compression by adjacent bone (“sandglass” configuration) [24]. Delineation against the surrounding soft-tissues is sharp. The involved common plantar digital nerve is only seldomly depicted as a thin hypoechoic structure in continuity with the neuroma [24, 25]. Normally no internal vascularization is detected, however highly painful “acute” neuromas may show increased vascularization as a consequence of vascular ingrowth from peri-neural inflammation [16, 25–28]. Neuromas smaller than 5 mm in diameter may be difficult to localize, as they may be masked by the fibro-fatty, inhomogenously structured plantar subcutis. Sometimes neuromas are even found incidentally in asymptomatic individuals.

Hypoechoic nodular Morton’s neuroma (star) between the heads of the second and third metatarsal (white arrows) in a transverse scan. The neuroma is well bordered but shows an irregular form due to mechanical stress; hyperechoic linear segments of the intermetatarsal ligament are depicted (arrowheads)
Mesenchymal peripheral neurogenic tumors
Neural fibrolipoma
This tumor—also called intraneural fibrolipomatous hamartoma—is the most common lesion originating from nonspecific neural tissue [2, 3, 29]. It is usually found in the upper extremity in adolescents and young adults—mainly the wrist section of the median nerve—and may present clinically like a carpal tunnel syndrome. Segmental swelling of the affected nerve is caused by augmentation of intraneural fat and connective tissue. Neural fascicles are dispersed but unaltered (Fig. 3a). If no compression neuropathy ensues, affected patients may be asymptomatic. In up to two thirds of cases, the lesion is combined with segmental macrodystrophia lipomatosa of one or more fingers and therefore is one important differential diagnosis of macrodactily [3, 16, 21].

a Neural fibrolipoma (magnification 50×): note two nerve fascicles (asterisks) in the middle upper and lower right image part with thickening of lipomatous (arrows) and fibrous (arrowheads) perineural connective tissue. b “Zoomed” appearance of fibrolipoma in the median nerve at the level of the carpal tunnel in a transverse scan (superficial flexor tendons are indicated by black stars). The hyperechoic outer sheath of the median nerve (white arrowheads) defines the markedly enlarged cross-section of the nerve with swollen hypoechoic fascicles embedded in hyperechoic fibrolipomatous tissue
On transverse HR-US scans, the lesion appears like a “zoomed” nerve segment (Fig. 3b). The relationship of the intraneural elements appears normal, with unaltered hypoechoic nerve fascicles, separated by grossly thickened hyperechoic lipomatous tissue [15]. This tumor never shows augmented vascularization.
Nerve sheath ganglion
This is a very rare form of a mesenchymal nerve tumor [3, 21, 24], mainly found in the knee region and thought to represent secondary ingrowth of synovial material from the adjacent joint capsule (mainly the proximal tibiofibular joint). Ganglion-like structures are found within the nerve sheath or interposed between fascicles (Fig. 4). Fascicles may be swollen because of compression by the ganglia. On HR-US, this lesion consists of one or more sharply lined intraneural fluid containing hypoechoic structures [21].

Anechoic intraneural ganglion (arrow) interposed between the fascicles of the ulnar nerve in the wrist. The fascicles (arrowheads) are displaced and thus the nerve is divided into a medial and a lateral portion
Intraneural hemangioma and hemangioblastoma
These very rare lesions derive from hamartomatous vascular foci, which progress to intraneural hemangioma or hemangioblastoma by connecting to normal intraneural capillaries [2, 21]. They are usually found in young patients and become clinically evident if producing compression syndromes [30, 31]. Hemangioblastomas are even rarer and found in the spinal nerve or nerve roots at their exit out of the vertebral column [32]. They are seen more frequently in von Hippel Lindau’s disease together with similar lesions in the CNS. In their position to the according nerve and their enhanced perfusion they may resemble neurolemomas but are considered semimalignant as single cases with metastatic seeding are reported.
Perineurioma
This mesenchymal nerve tumor, forming out of perineural cell proliferations, produces localized nerve swellings [33]. Histologically the tumor has a typical onion-like inner structure and—as it grows between neural fascicles in a perineural growth pattern—the normal fascicular neural structure is preserved for a long time. This lesion is usually not specified by HR-US, as it merely presents a subtle swelling of a short neural segment with progressive hypoechoic loss of the typical inner nerve structure [29], which may equally be found with nerve compression.
Benign PNST
PNSTs comprise two major (neurolemoma and neurofibroma), and a minor form (granular cell tumor). All PNSTs derive from specific peripheral neural tissue [2, 3], and usually present as hypoechoic masses, connected with a peripheral nerve.
Neurolemoma (schwannoma, neurinoma)
This is typically a solitary lesion and usually occurs sporadically in young adults. Most often cervical nerve roots are affected. If located in more peripheral nerves (most frequently in ulnar and peroneal nerves), the lesion develops on the flexor sides of extremities [2, 3]. The autonomous nervous system may also be affected and sometimes large tumors develop in the neck, the mediastinum and retroperitoneum [36].
Neurolemomas grow slowly and may have a size of several centimeters when detected. Large lesions may be symptomatic. There are several distinct histological subtypes: common, plexiform, cellular, epithelioid, and ancient neurolemoma. Multiplicity of lesions and plexiform types are associated with NF1 in up to 20% and may even be the only expression of this disorder [3, 5, 37].
On HR-US, neurolemomas usually present as small, hypoechoic, spindle shaped nodules connected to a peripheral nerve. They are oriented along the long axis of a nerve with proximal and distal tail-like formations [2, 3, 16, 21, 24, 29, 34]. Neurolemomas typically only displace the nerve fascicles (Fig. 5a), which is an important diagnostic feature. They are encased by the sonographic outer nerve sheath. With increasing tumor size, the lesions are generally positioned eccentrically to the affected nerve segment (Fig. 5b). Another typical feature of large lesions are hyperechoic calcifications (Fig. 5c) and internal degenerative cystic foci (Fig. 5d,e). Ancient neurolemomas (Fig. 5f) show marked degenerative changes, such as internal bleeding, fibrosis or calcification and cystic necrotic alterations [3, 16, 29, 31, 36]. Especially in large lesions, nerve fascicles are impressively displaced, increased internal vascularization is seen with duplex HR-US [21, 29] and a definite distinction from a hypervascular malignant lesion may be difficult. However, tumor vessels entering from the proximal and distal pole, monomorphic duplex waveforms, together with a “benign” (hierarchic) vascular architecture (Fig. 5g), are typical for neurolemoma [12].

a Neurolemoma—macroscopic view. Pseudoencapsulated tumor with typical oval configuration in excentric alignment with the nerve. b Excentric neurolemoma (distance markers) displacing the according nerve fascicles (black arrowheads). The tumor has a homogeneous hypoechoic texture and a relatively sharp border. c Well bordered hypoechoic nodular neurolemoma of the femoral nerve. Sparse intralesional spots of calcification (white arrows) in a clearly nerve-connected tumor (conus-like tail). dA: Neurolemoma—microscopic view. Note the continuous pseudocapsule on the left side of the image by palisading cell layers (so-called Antoni A pattern) and the presence of degenerative pseudocystic and xanthomatous areas (black stars, so-called Antoni B pattern) on the right side of the image (magnification 100×); Inset: typical palisading to storiform texture pattern of the tumor (so-called Antony A pattern) (magnification 200×). B: Corresponding HR-US scan shows the degenerative pseudocystic inner changes (white stars). e Neurolemoma of median nerve. Well defined clearly nerve-connected tumor with homogeneous hypoechoic texture and posterior enhancement. Additionally a conus-like tumor-tail (arrowheads) grows along the axis of the nerve. Regressive intralesional pseudocysts are evident (arrows). f Ancient neurolemoma of the right thoracodorsal nerve. Although histologically benign this tumor presents features suspicious of malignancy with central regressive necrosis(arrow). g Marked perfusion in a neurolemoma with typical relatively high-resistance duplex waveform (low diastolic flow)
Neurofibroma
Typically found in the same population group as neurolemomas [1, 2, 4], the most common variant of neurofibroma is “solitary localized neurofibroma”; typically a slowly growing, small subcutaneous tumor in small nerve branches (Fig. 6a). This variant is rarely found in large nerves and associated with NF1 in only 10%. The “diffuse” type neurofibroma is usually also found sporadically and associated with NF1 in only 10%, while “plexiform neurofibroma” is characteristic of NF1 [3, 5].

aA: Typical aspect of multiple cutaneous neurofibromas (asterisks). B: Typical pseudonodular thickening of an affected nerve trunk by plexiform neurofibroma—macroscopic view. C: Plexiform neurofibroma (magnification 25×); note three fibromatous finger-like poorly delineated tumor nodules (asterisks) interfering with “normal” peripheral nerve tissue. D: Pathognomonic hypocellular appearance of the tumor tissue of neurofibroma with wavy fibers and nuclei (magnification 200×). b Hyper- and hypoechoic “onion-like” layering is the “target sign” of a neurofibroma (arrowheads) in a transverse scan. Although this tumor usually interferes with the fascicular structure, some not affected fascicles are displaced by the lesion (white star). c Longitudinal extended field of view scan of the brachial plexus shows a pearl-like arrangement of multiple oval neurofibromas (arrows) in a NF1 patient (“bag of worms”). d Corresponding transverse scan: multiple nerve connected nodules (arrows) in the brachial plexus in a NF1 patient. All fascicles are consumed by the tumor formation
In HR-US, localized neurofibroma presents as a homogeneous, (but in contrast to neurolemoma) concentric, clearly bordered nodular lesion that does not (like neurolemoma) displace the fascicular elements of the according nerve but interferes with them [3, 16, 21, 29, 36]. Another typical sonographic feature of neurofibromas is the so-called “target sign”; this layered aspect, with a hyperechoic centre and a peripheral hypoechoic rim (Fig. 6b), best seen on transverse scans, is due to the ultrastructure of neurofibromas with a fibrocollageneous center surrounded by a myxomateous periphery [16, 34, 35]. Large lesions often protrude beyond the surface of the nerve, without a clear capsule [3].
Plexiform neurofibromas start to develop in early childhood and present as inhomogeneous nodular tumor-bands within affected nerves (“bag of worms”). This form has a clear predilection for nerve segments next to the vertebral column with a slow outward progression [2, 3, 5]. The lesion can progressively affect the entire region of the brachial and cervical plexus, which results in huge tumor formations [16, 21, 34]. As it grows constantly, the individual nodules often break through the outer nerve sheath and extend into the peri-neural tissues (Fig. 6c,d). Due to this expansive growth, bizarre hypertrophy and deformation of affected body regions known as elephantiasis neuromatosa is seen [3, 38, 39]. Plexiform neurofibromas are known precursors of MPNST [2, 3, 5].
Granular cell tumor (GCT, Abrikossoff’s tumor)
This very rare and usually benign neoplasm is thought to derive from Schwann cells of peripheral nerves. It occurs most commonly in middle aged women [2, 15], derives from small nerve branches and develops in the subcutis of the head and neck, the submucosa of the gastrointestinal tract [40–42] and may also occur in the female breast. In the latter location, it presents as an irregularly bordered hypoechoic lesion with posterior acoustic shadowing suggestive for breast malignancy. Often small internal calcifications may be detected (Fig. 7). The definite diagnosis relies on US guided biopsy and immunhistochemical staining.

Granular cell tumor: concentric, tuberous dominantly hypoechoic peripheral neurogenic tumor in continuity to the affected femoral nerve (arrow) in a longitudinal scan. Typical small internal calcifications (arrowheads) resulting in impressive posterior shadowing
MPNST
The term MPNST (formerly “spindle cell sarcoma”) includes all malignant tumors with neural differentiation arising from peripheral nerves (Fig. 8a). Mostly high-grade soft-tissue sarcomas, they comprise between 5% and 10% of all soft tissue tumors and typically arise between 20 and 50 years of age [3, 4, 43]. MPNST are associated with more than two-thirds ofNF1 cases, and NF-patients have an estimated prevalence for malignant transformation of plexiform neurofibromas to MPNST of up to 50% [28]. Sporadic MPNST may occur as secondary neoplasms after radiation therapy with a latency of up to two decades and in this case are mainly found in the sacral plexus [3–5].

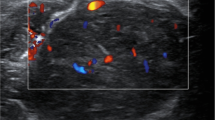
a Infiltration of fatty tissue by an MPNST. Tumor tissue presents a shoal-like arrangement with nuclear irregularities together with a criss-cross growth pattern of neoplastic pseudofascicles (double-headed arrows) (magnification 200×). b Extended field of view scan (panorama) of a MPNST with multiple metaplastic inner transformations. The lesion shows pseudocystic necrotic areas (white arrowheads) together with irregular calcifications and posterior shadowing (white arrow). c Color Doppler image, showing marked hypervascularisation and irregular vascular pattern in a huge MPNST. d Duplex US image in the same patient, showing arterial waveform with high diastolic forward flow suggestive of arterio-venous shunting
MPNST are predominantly found in the plexus regions and in large nerves. Usually—and in contrast to benign PNST—they develop fast, with progressively worsening neurological symptoms, beginning with weakness and sensory deficits in the inervation area of the involved nerve [3, 4].
On HR-US, small MPNST often present as inhomogeneous, hypoechoic, fusiform masses connected with a peripheral nerve. Some lesions show a pseudocapsule consisting of irregularly thickened segments of the hyperechoic outer nerve sheath, others present a poor outer margin [16, 21, 22, 24, 29, 36]. The growth along the course of the affected nerve is similar to benign PNST. Depending on the precursor lesion (neurolemoma-like or neurofibroma-like), a tendency to irregular cystic necrotic degeneration or a hyperechoic irregular inner pattern with calcifications may be encountered (Fig. 8b). Over time, the texture gets more and more inhomogeneous, with areas of internal bleeding, hypoechoic necrosis and calcifications. With increasing size, the heterogeneity becomes more evident and areas of heterotopic tissue—such as hypoechoic cartilage, hyperechoic bone formation, or (pseudo)glandular tissue—may be found [3, 4]. Duplex HR-US usually shows a sarcoma-type anarchic hypervascularization pattern. Such neo-angiogenetic arteries show high velocity duplex spectra with different flow velocities and spectral wave forms in different tumor areas. Resistance indices may be rather low, implying arterio-venous shunt vessels. Very typical for MPNST are corkscrew-like neo-vessels. These are often found entering the MPNST from the proximal or distal tumor-pole [3, 4, 12, 16, 21, 22, 24, 29, 36].
Conclusion
HR-US with application of color Doppler and duplex mode has a high potential for the detection and differentiation of peripheral nerve tumors. It should, therefore, be the first line imaging modality for the analysis of a superficial mass lesion, especially if there is clinical suspicion for a connection of the lesion with a peripheral nerve. HR-US combines high availability with unrivaled resolution, which allows for analysis of the internal structure of lesions and in most cases easily establishes the association of a lesion with a peripheral nerve. The orientation of a tumor along the nerve, together with assessment of the state of nerve fascicles and tumor perfusion, are easily feasible and important features for the differential diagnosis and treatment planning. For only incompletely accessible and large lesions—usually MPNST—magnetic resonance imaging (or computed tomography) should follow in the diagnostic work-up, especially for the assessment of the spatial extent of such a lesion.
References
Hughes DG, Wilson DJ (1986) Ultrasound appearances of peripheral nerve tumours. Br J Radiol 59:1041–1043
Enzinger FM, Weiss SW (1995) Benign tumors of peripheral nerves. In: Enzinger FM, Weiss SW (eds) Soft tissue tumors, 3rd edn. Mosby, St Louis, pp 821–888
Murphey MD, Smith WS, Smith SE, Kransdorf MJ, Temple HT (1999) From the archives of the AFIP. Imaging of musculoskeletal neurogenic tumors: radiologic-pathologic correlation. Radiographics 19:1253–1280
Enzinger FM, Weiss SW (1995) Malignant tumors of the peripheral nerves. In: Enzinger FM, Weiss SW (eds) Soft tissue tumors, 3rd edn. Mosby, St Louis, pp 889–928
Riccardi VM (1981) Von Recklinghausen neurofibromatosis. New Engl J Med 305:1617–1627
Fornage BD (1988) Peripheral nerves of the extremities: imaging with US. Radiology 167:179–182
Graif M, Seton A, Nerubali J et al (1991) Sciatic nerve: sonographic evaluation and anatomic-pathologic considerations. Radiology 181:405–408
Silvestri E, Martinoli C, Derchi LE et al (1995) Echotexture of peripheral nerves: correlation between US and histologic findings and criteria to differentiate tendons. Radiology 197:291–296
Martinoli C, Bianchi S, Derchi LE (1999) Tendon and nerve sonography. Radiol Clin North Am 37:691–711
Buchberger W, Judmaier W, Birbamer G et al (1992) Carpal tunnel syndrome: diagnosis with high-resolution sonography. AJR Am J Roentgenol 159:793–798
Martinoli C, Serafini G, Bianchi S, Bertolotto M, Gandolfo N, Derchi LE (1996) Ultrasonography of peripheral nerves. J Peripher Nerv Syst 1:169–178
Bodner G, Schocke MF, Rachbauer F, Seppi K, Peer S, Fierlinger A, Sununu T, Jaschke WR (2002) Differentiation of malignant and benign musculoskeletal tumors: combined color and power Doppler US and spectral wave analysis. Radiology 223:410–416
Kiechl S (2003) An introduction to electrodiagnostic testing. In: Peer S, Bodner G (eds) High-resolution sonography of the peripheral nervous system. Springer, Berlin Heidelberg New York, pp 121–134
Gruber H, Kovacs P (2003) Sonographic anatomy of the peripheral nervous system. In: Peer S, Bodner G (eds) High-resolution sonography of the peripheral nervous system. Springer, Berlin Heidelberg New York, pp 13–36
Riede UN, Schaefer HE (1995) Allgemeine und spezielle Pathologie. Thieme, Stuttgart New York
Bacigalupo L, Bianchi S, Valle M et al (2003) Ultraschall peripherer Nerven. Radiologe 43:841–849
Peer S, Bodner G, Meirer R et al (2001) Examination of postoperative peripheral nerve lesions with high-resolution sonography. AJR Am J Roentgenol 177:415–419
Shafighi M, Gurunluoglu R, Ninkovic M et al (2003) Ultrasonography for depiction of brachial plexus injury. J Ultrasound Med 22:631–634
Gruber H, Glodny B, Galiano K, Kamelger F, Bodner G, Hussl H, Peer S (2006) High-resolution ultrasound of the supraclavicular brachial plexus-can it improve therapeutic decisions in patients with plexus trauma? Eur Radiol DOI 10.1007/s00330-006-0464-2
Piza-Katzer H (2003) Clinical considerations: the surgeon’s perspective. In: Peer S, Bodner G (eds) High-resolution sonography of the peripheral nervous system. Springer, Berlin Heidelberg New York, pp 107–120
Bendix N, Wolf C, Gruber H, Bodner G (2005) Ultrasound of tumours and tumour-like lesions of peripheral nerves. Ultraschall Med 26:318–324
Chiou HJ, Chou YH, Chiou SY et al (2003) Peripheral nerve lesions: role of high-resolution ultrasound. Radiographics 23:15e
Gruber H, Kovacs P, Peer S, Frischhut B, Bodner G (2004) Sonographically guided phenol injection in painful stump neuroma. AJR Am J Roentgenol 182:952–954
Beggs I (1999) Sonographic appearances of nerve tumors. J Clin Ultrasound 27:363–368
Redd RA, Peters VJ, Emery SF, Branch HM, Rifkin MD (1989) Morton neuroma: sonographic evaluation. Radiology 171:415–417
Sobiesk GA, Wertheimer SJ, Schulz R et al (1997) Sonographic evaluation of interdigital neuromas. J Foot Ankle Surg 36:364–366
Read JW, Noakes JB, Kerr D et al (1999) Mortons metatarsalgia: sonographic findings and correlated histopathology. Foot Ankle Int 20:153–161
Quinn TJ, Jacobson JA, Craig JG, van Holsbeeck MT (2000) Sonography of Mortons neuromas. AJR Am J Roentgenol 174:1723–1728
Stuart RM, Koh ESC, Breidahl WH (2003) Sonography of peripheral nerve pathology. AJR Am J Roentgenol 182:123
Kline SC, Moore JR (1992) Intraneural hemangioma: a case report of acute cubital tunnel syndrome. J Hand Surg [Am] 17:305–307
Van Meir N, De Smet L (2003) Carpal tunnel syndrome in children. Acta Orthop Belg 69:387–395
Glasker S, Berlis A, Pagenstecher A et al (2005) Characterization of hemangioblastomas of spinal nerves. Neurosurgery 56:503–509
Heilbrun ME, Tsuruda JS, Townsend JJ et al (2001) Intraneural perineurioma of the common peroneal nerve. Case report and review of the literature. J Neurosurg 94:811–815
Reynolds DL, Jacobson JA, Inampudi P et al (2004) Sonographic characteristics of peripheral nerve sheath tumors. AJR Am J Roentgenol 182:741–744
Lin J, Jacobson JA, Hayes CW (1999) Sonographic target sign in neurofibromas. J Ultrasound Med 18:513–517
De Schepper AM (1997) Imaging of soft tissue tumors. Springer, Berlin Heidelberg New York
Hughes MJ, Thomas JM, Fisher C, Moskovic EC (2005) Imaging features of retroperitoneal and pelvic schwannomas. Clin Radiol 60:886–893
Lin J, Martel W (2001) Cross-sectional imaging of peripheral nerve sheath tumors: characteristic signs on CT, MR imaging, and sonography. AJR Am J Roentgenol 176:75–82
Hourani R, Rizk T, Kung S, Boudghene F (2006) Elephantiasis neuromatosa in neurofibromatis type I. MRI findings with review of the literature. J Neuroradiol 33:62–66
Brannon RB, Anand PM (2004) Oral granular cell tumors: an analysis of 10 new pediatric and adolescent cases and a review of the literature. J Clin Pediatr Dent 29:69–74
Porter GJ, Evans AJ, Lee AH, Hamilton LJ, James JJ (2006) Unusual benign breast lesions. Clin Radiol 61:562–569
Adeniran A, Al-Ahmadie H, Mahoney MC, Robinson-Smith TM (2004) Granular cell tumor of the breast: a series of 17 cases and review of the literature. Breast J 10:528–531
Wanebo JE, Malik JM, VandenBerg SR, Wanebo HJ, Driesen N, Persing JA (1993) Malignant peripheral nerve sheath tumors. A clinicopathologic study of 28 cases. Cancer 71:1247–1253
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Gruber, H., Glodny, B., Bendix, N. et al. High-resolution ultrasound of peripheral neurogenic tumors. Eur Radiol 17, 2880–2888 (2007). https://doi.org/10.1007/s00330-007-0645-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-007-0645-7