
Abstract
Short echo time single voxel methods were used in previous MR spectroscopy studies of phenylalanine (Phe) levels in phenylketonuria (PKU) patients. In this study, apparent T 2 relaxation time of the 7.3-ppm Phe multiplet signal in the brain of PKU patients was assessed in order to establish which echo time would be optimal. 1H chemical shift imaging (CSI) examinations of a transverse plain above the ventricles of the brain were performed in 10 PKU patients and 11 persons not suffering from PKU at 1.5 T, using four echo times (TE 20, 40, 135 and 270 ms). Phe was detectable only when the signals from all CSI voxels were summarized. In patients suffering from PKU the T 2 relaxation times of choline, creatine and N-acetyl aspartate (NAA) were similar to those previously reported for healthy volunteers (between 200 and 325 ms). The T 2 of Phe in brain tissue was 215±120 ms (standard deviation). In the PKU patients the brain tissue Phe concentrations were 141±69 μM as opposed to 58±23 μM in the persons not suffering from PKU. In the detection of Phe, MR spectroscopy performed at TE 135 or 270 ms is not inferior to that performed at TE 20 or 40 ms (all previous studies). Best results were obtained at TE=135 ms, relating to the fact that at that particular TE, the visibility of a compound with a T 2 of 215 ms still is good, while interfering signals from short-TE compounds are negligible.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Phenylketonuria (PKU) is the most common inborn error of aminoacid metabolism, with a frequency of 1:4,000 in Europe, and always has been a model for the understanding and treatment of inborn errors of metabolism. PKU results form a deficiency of the hepatic enzyme phenylalanine hydroxylase (PAH), which converts phenylalanine (Phe) into tyrosine (Tyr). When deficient, the resulting high Phe concentrations are associated with severe intellectual handicap. This phenotype is prevented by neonatal screening and maintaining almost normal Phe concentrations in the blood. Treatment is by severe (up to 90%) dietary restriction of natural protein supplemented with a Tyr-enriched aminoacid mixture without Phe. Treatment is monitored by measurement of Phe in the blood. Notwithstanding its effectiveness, the diet is burdensome. Other treatment options could improve the quality of life, while approximately one out of six untreated patients may escape severe mental retardation [1]. In the current literature, there is no consensus about the question whether or not the level of Phe in the brain that is crucial because it determines the neurotoxicity of Phe is reflected by its level in the blood. This has triggered several groups to start applying MR spectroscopy for attempting to quantify the level of Phe in brain tissue.
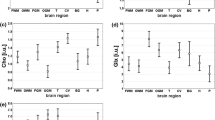
The longitudinal and transverse relaxation times (T 1s, T 2s) of the signals of choline (Cho), creatine (Cr) and N-acetyl aspartate (NAA) in normal human brain tissues have been documented by numerous groups [2–9]. The concentration of Phe in normal brain tissue is more than one order of magnitude lower than those of Cho, Cr and NAA and according to one study [10] similar to its level in blood, i.e., 50–90 μM. The poor sensitivity of MR spectroscopy to low-concentration metabolites probably explains why the relaxation behavior of Phe in brain tissue has not yet been documented. In patients suffering from PKU, brain tissue Phe levels in the order of 250–600 μM have been observed, however [10–12]. PKU patients have blood Phe levels that are roughly three times as high as those in brain tissue [10–14] and cerebrospinal fluid [15].
In previous MR spectroscopy studies focusing on the detection of Phe in the brain tissue of PKU patients, Phe was measured with the shortest TE available (20–40 ms), apparently to cope with the possibility that the T 2 of Phe might be very short. Under those conditions, Phe could be observed by most investigators [10–14], though not by all [16], provided that the selected volume of interest was large. Optimization of the detection of Phe in the brain of PKU patients was the purpose of this study. Automated chemical shift imaging (CSI) of a transverse plane above the ventricles is used (1) to compare the spectra of separate voxels to those of the whole plane combined, (2) to calculate the T 2 of Phe from the results of CSIs made at TEs of 20, 40, 135 and 270 ms and (3) to assess at what TE Phe is visualized best.
Materials and methods
MR spectroscopy examinations of 10n PKU patients (4 male, 6 female) and 11 persons not suffering from PKU (6 male, 5 female) were performed at 1.5 T using the standard head coil of a Siemens Magnetom Vision MR scanner (Siemens AG, Erlangen, Germany). Mean age of PKU patients was 27±8 (SD) years. The other persons examined by MRS consisted of two apparently healthy people and nine ones suffering from diseases known not to cause elevation of Phe levels and had a mean age of 16±7 years. Informed consent was obtained after the nature of the procedures had been fully explained. Blood Phe concentrations of PKU patients at the time of MR spectroscopy varied between 358 and 1,362 μM (mean 718, SD 310).
1H chemical shift imaging
Four automated hybrid point resolved spectroscopy (PRESS) 2D-CSI measurements with a repetition time (TR) of 1,500 ms and echo times of 20 ms (STEAM, stimulated echo acquisition mode) and of 40, 135 and 270 ms (SE, spin echo) were performed. Hybrid-CSI includes pre-selection of a volume of interest (VOI) that is located within the brain to prevent the strong interference from subcutaneous fat and is smaller than the phase-encode field of view (FOV) that must be large enough to prevent wraparound artifacts [17]. The CSI sequence produced a 16×16 transversely oriented matrix that was defined by phase encoding with a FOV of 16×16 cm2. The VOI was positioned in a plane above the ventricles, resulting in maps of 8×8 spectra (VOI 8×8×2 cm3) selected with respective field gradients of 0.8, 0.8 and 3.0 mT/m. The field homogeneity achieved in automated non-localized multiple angle projection (MAP) shimming resulted in water peak linewidths of typically less than 8 Hz in the VOI. Spectral maps were collected with 2.56 ms sinc-Hanning shaped RF pulses preceded by 25.6 ms Gaussian shaped RF pulses for chemical shift selective excitation (CHESS) and subsequent spoiling of the resultant water signal. The second spin echo was collected using 1,024 data points and a spectral width of 500 Hz. All 16×16 2D-CSI measurements were one acquisition per phase-encoded step with four prescans and TRs of 1,500 ms (acquisition time 6.5 min). Time domain data were multiplied with a Gaussian function (center 0 ms, half width 256 ms), 2D-Fourier transformed, phase and baseline corrected and quantified by means of frequency domain curve fitting with the assumption of Gaussian line shapes, using the standard “Numaris-3” software package provided with the MR system. In the curve fitting the number of peaks fitted included the chemical shift ranges restricted to 7.2–7.4 ppm for Phe, 3.1–3.3 for Cho, 2.9–3.1 for Cr, 1.9–2.1 for NAA, and their line widths and peak intensities unrestricted. (Signal-to-noise considerations led us to approximate the multiplet signal of Phe by fitting to a single peak.) Although automated phase and baseline correction provided good starting values, manual fine adjustment of the phase and of the peak ranges excluded in polynomial baseline correction was needed in some cases. We used an assumption made in previous quantitative MRS studies of PKU (e.g., 12) that the Cr levels in patients and controls are 6.1 mM. Our additional assumption that at the TR used (1,500 ms) differential peak saturation due to a difference in T 1 value between Phe and Cr is negligible was based on results obtained in CSI measurements repeated at TR 5,000 ms. The use of Cr as internal reference is reasonable in view of the fact that nobody has reported any difference between the brain tissue Cr levels in PKU patients and controls. Apparent T 2s for the metabolites in brain tissue in PKU patients and controls were assessed from fitting of the metabolite areas obtained at TEs 20, 40, 135 and 270 ms to the equation: \(M_{y} = M_{0} \exp {\left[ { - {\text{TE}}/T_{2} } \right]}\), with correction for the fact that STEAM signals are 50% reduced relative to SE signals [18]. In this formula the above areas correspond to the M y values at t=20, 40, 135 and 270 ms, respectively.
Results
The spectral maps and the sums of the Cho, Cr and NAA signals of the quantified inner 6×6=36 CSI voxels (total volume 72 cm3) for one of the PKU patients measured at TEs 20, 40, 135 and 270 ms are shown in Fig. 1. The smaller portions of the spectrum shown at the shorter TEs (1.5–3.6 ppm rather than 0.5–4.3 ppm) reflect restrictions in the baseline ranges used for optimal baseline correction. The peak intensity scales for each spectrum are arbitrary, i.e., neither related to absolute concentrations nor suited for direct quantitative comparisons of measurements performed at different TEs.

a Spectral maps and b corresponding summarized spectrum in supraventricular VOI of PKU patient showing the resonances of Cho, Cr and NAA measured at TR=1,500 ms and TEs of 20 ms (upper left), 40 ms (upper right), 135 ms (lower left) and 270 ms (lower right). The frequency ranges vary per sequence with the applied baseline correction limits. Peak intensities, arbitrary units. Acquisition time: 6:31 min
It shows that with increasing TE the signals of Cho and especially Cr drop relatively to NAA. This reflects the order of the T 2 values that we observed in the PKU patients (Cr<Cho<NAA), similar to that in published control values (Table 1). At any TE the signal of Phe was close to the noise level, even in PKU patients (Fig. 2). The signal-to noise ratio in the 7.3-ppm Phe multiplet signal varied between 3 and 5, without a significant difference amongst the four TEs used. At TE=135 ms Phe was generally observed more clearly than at TE 270 ms or at the shorter TEs (20–40 ms). In analogy to the practice in previous MRS studies of PKU patients of measuring very large voxels in order to get sufficient signal per unit of measuring time, in our study the Phe signals from the individual voxels (2 cm3 each) of our CSI maps had to be summarized. Spectral map display of the array of individual Phe signals is therefore not meaningful.

A different frequency range of the spectra of Fig. 1 showing, among the noise, the main resonance of Phe (7.3 ppm). Measured at TR=1,500 ms and TEs of 20 ms (upper left), 40 ms (upper right), 135 ms (lower left) and 270 ms (lower right)
As a group, apparent brain concentrations of Phe in PKU patients, shown in Table 2, were not correlated to the corresponding concentrations in blood sampled on the day of MRS (r=0.16 in PKU patients, NS).
Discussion
The purpose of this study was optimization of the detection of Phe in the brain of PKU patients. Unlike in all previous studies, a multiple voxel method, CSI, was used here, and measurements were repeated at four different TEs. The spectral maps of Fig. 1a demonstrate that B 0 homogeneity of the magnetic field was excellent. This is evident from the resolution between the Cho and Cr peaks throughout the 8×8×2 cm3 VOI. Furthermore, the B 1 field was highly homogeneous as proven by the even distributions of peak heights throughout the VOI, indicating that the PRESS 90° pulses were effectively the same within the VOI. The good B 0 field allowed us to summarize the signals, a standard Vision “Numaris-3” option, of all CSI voxels without experiencing significant loss of spectral resolution (Fig. 1b). This validated our approach to summarize the spectra of all voxels prior to starting our Phe T 2 calculations (Fig. 2). In a single voxel of a CSI map the Phe signal was so weak that we had no alternative for summing the signals of all voxels. We conclude that for the detection of Phe multivoxel CSI offers no benefits compared with the large single voxel methods applied in previous studies [2–9].
Curious is the presence of a strong resonance at a position of 8.5 ppm, in Fig. 2 most prominent at TEs of 20 ms and 40 ms. This could be signal contributed by the aromatic protons of other molecules known to accumulate in PKU patients such as phenylpyruvate or phenylacetate.
Fitting the summarized Phe signals obtained at the four TE values to the above-mentioned equation yielded a median Phe T 2 value of 215 ms in our PKU patients. This value is similar to the transverse relaxation times of Cho, Cr and NAA in our PKU patients, as well as to the values published for normal brain (Table 1). We have thus shown that the apparent T 2 of Phe in brain tissue is such that short-TE examinations as applied in all previous MRS studies are not necessary for the detection of Phe. Our impression that visibility of Phe was best at TE=135 ms probably relates to the fact that at that particular TE the visibility of a compound with a T 2 of 215 ms still is good, \(M_{y} = M_{0} \exp {\left[ { - t/T_{2} } \right]} = M_{0} \exp {\left[ { - 135/224} \right]} = 0.55\), while interfering signals from short-TE compounds are negligible.
Mean blood brain ratio for Phe obtained in this study is comparatively high compared with the ratios reported in previous studies of PKU patients. This can be attributed to several factors, including (1) coincidence, in view of the weak correlation between blood and brain Phe levels reported here and in most previous MRS studies [10, 12, 13], (2) the poor signal-to-noise ratio of the Phe peak in all previous studies as well as in this study and (3) the use of shorter TE only in previous studies potentially leading to overestimation of the Phe peak because of the inclusion of signals from broad components with short T 2s (a problem reduced by most authors by subtracting the signals encountered in control spectra). Subpopulations of PKU patients with highly individual (normal and abnormal) blood to brain ratios for Phe as reported by others [10, 13, 14, 19, 20] could not be discriminated in this study, probably because in our case treatment of patients never resulted in very high blood Phe levels. This is noted here because, currently, the blood to brain ratio of Phe is an issue of intense discussion [14, 21–23].
References
Van Spronsen FJ, van Rijn M, van Dijk T, Smit GP, Reijngoud DJ, Berger R, Heymans HS (1993) Plasma phenylalanine and tyrosine responses to different nutritional conditions (fasting/postprandial) in patients with phenylketonuria: effect of sample timing. Pediatrics 92:570–573
Frahm J, Bruhn H, Gyngell ML, Merboldt KD, Hänicke W, Sauter R (1989) Localized proton spectroscopy in different regions of the human brain in vivo. Relaxation times and concentrations of cerebral metabolites. Magn Reson Med 11:47–63
Narayana PA, Johnston D, Flamig DP (1991) In vivo proton magnetic resonance spectroscopy studies of human brain. Magn Reson Imaging 9:303–308
Hennig J, Pfister H, Ernst T, Ott D (1992) Direct absolute quantitation of metabolites in the human brain with in vivo localized proton spectroscopy. NMR Biomed 5:193–199
Barker PJ, Soher BJ, Blackband SJ, Chatham JC, Mathews VP, Bryan RN (1993) Quantitation of proton NMR spectra of the human brain using tissue water as an internal concentration reference. NMR Biomed 6:89–94
Kreis R, Ernst T, Ross BD (1993) Development of the human brain: in vivo quantification of metabolite and water content with proton magnetic resonance spectroscopy. Magn Reson Med 30:424–437
Christiansen P, Toft PB, Larsson HBW, Stubgaard M, Henriksen O (1993) The concentration of N-acetylaspartate, creatine + phosphocreatine, and choline in different parts of the brain in adulthood and senium. Magn Reson Imaging 11:799–806
Kamada K, Houkin K, Hida K, Iwasaki Y, Abe H, Kashiwaba T (1994) In vivo proton magnetic resonance spectroscopy for metabolic changes of human brain edema. Neurol Med Chir (Tokyo) 34:676–681
Sijens PE, Oudkerk M (2002) 1H chemical shift imaging characterization of human brain tumor and edema. Eur Radiol 12:2056–2061
Koch R, Moats R, Guttler F, Guldberg P, Nelson M Jr (2000) Blood-brain phenylalanine relationships in persons with phenylketonuria. Pediatrics 106:1093–1096
Pietz J, Kreis R, Rupp A, Mayatepek E, Rating D, Boesch C, Bremer HJ (1999) Large neutral amino acids block phenylalanine transport into brain tissue in patients with phenylketonuria. J Clin Invest 103:1169–1178
Novotny EJ, Avison MJ, Herschkowitz N, Petroff OAC, Prichard JW, Seashore MR, Rothman DL (1995) In vivo measurement of phenylalanine in human brain by proton nuclear magnetic resonance spectroscopy. Pediatr Res 37:244–249
Moats RA, Koch R, Moseley K, Guldberg P, Guttler F, boles RG, Nelson MD Jr (2000) Brain phenylalanine concentration in the management of adults with ketonuria. J Inherit Metab Dis 23:7–14
Weglage J, Wiedermann D, Denecke J, Feldman R, Koch HG, Ullrich K, Harms E, Möller HE (2001) Individual blood-brain barrier phenylalanine transport determines clinical outcome in phenylketonuria. Ann Neurol 50:463–467
Antoshechkin AG, Chentsova TV, Tatur VY, Naritsin DB, Railian GP (1991) Content of phenylalanine, tyrosine and their metabolites in CSF in phenylketonuria. J Inherit Metab Dis 14:749–754
Johannik K, Van Hecke P, Marchal G, Smet MH, Jaeken J, Breysem L, Wilms G, Baert AL (1994) Localized brain proton NMR spectroscopy in young adult phenylketonuria patients. Magn Reson Med 31:53–57
Sijens PE, van den Bent MJ, Nowak PJCM, van Dijk P, Oudkerk M (1997) 1H chemical shift imaging reveals loss of brain tumor choline signal after administration of Gd-contrast agent. Magn Reson Med 37:222–225
Hentschel D, Ladebeck R (1990) In vivo localized 1H MR with spin echoes and stimulated echoes: a quantitative comparison. Appl Magn Reson 1:41–46
Moller HE, Weglage J, Wiedermann D, Ullrich K (1998) Blood-brain barrier phenylalanine transport and individual vulnerability in phenylketonuria. J Cereb Blood Flow Metab 18:1184–1191
Weglage J, Wiedermann D, Denecke J, Feldmann R, Koch HG, Ullrich K, Moller HE (2002) Individual blood-brain barrier phenylalanine transport in siblings with classical phenylketonuria. J Inherit Metab Dis 25:431–436
Rupp A, Kreis R, Zschocke J, Slotboom J, Boesch C, Rating D, Pietz J (2001) Variability of blood-brain ratios of phenylalanine in typical patients with phenylketonuria. J Cereb Blood Flow Metab 21:276–284
Pietz J, Rupp A, Burgard P, Boesch C, Kreis R (2002) No evidence for individual blood-brain barrier phenylalanine transport to influence clinical outcome in typical phenylketonuria patients. Ann Neurol 52:382–383
Weglage J, Wiedermann D, Feldman R, Ullrich K, Möller HE (2002) Reply. Ann Neurol 52:383–384
Acknowledgments
The authors thank Peter Kappert (Department of Radiology, University Hospital Groningen) for participating in the data acquisition.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Sijens, P.E., Oudkerk, M., Reijngoud, DJ. et al. 1H MR chemical shift imaging detection of phenylalanine in patients suffering from phenylketonuria (PKU). Eur Radiol 14, 1895–1900 (2004). https://doi.org/10.1007/s00330-004-2388-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-004-2388-z